When and how to assess pancreatic function: an update for clinicians –Sohail Z. Husain, MD (page 31)
Reviewed methods of detecting pancreatic insufficiency
Indirect (non-stimulatory) Methods
Stool:
- Fecal Fat Analysis: Coefficient of fat absorption (CFA): (fat intake – fat in stool / fat intake) * 100
- Normal > 93% (> 85% in less than 6 mo.
- old)
- 72 hr collection gold standard
ELASTASE-1: Stable, specific for human pancreas
- Normal > 200 μg elastase/g stool
- Particularly good for monitoring the development of PI in patients with CF
- Low levels (false-positive) with diarrhea
- Only detects severe PI
Other tests
- Chymotrypsin: less sensitive; requires discontinuation of enzymes
- Steatocrit: cheap; has low sensitivity
- Serum
- Breath
- Direct (stimulatory)
- Dreiling tube
- Endoscopic pancreatic function testing (ePFT)
- Secretin-enhanced MRCP (sMRCP)
Causes of Pancreatic Insufficiency
-85% of patients with Cystic Fibrosis have pancreatic insufficiency
Shwachman-Diamond Syndrome
- Mutation in SBDS, found in ~90% of SDS patients
- PI affects almost all SDS pts
Johanson-Blizzard syndrome (JBS): Key findings
- PI
- Severe developmental delay
- Hypoplasia or aplasia of the nasal wings
Pearson marrow pancreas syndrome Key findings: Severe hypoplastic,macrocytic anemia, Pancreatic insufficiency (due to pancreatic fibrosis)
Diagnosis: Clinical picture, High serum lactate/pyruvate, Southern blot for mtDNA rearrangements
Other causes of pancreatic insufficiency
- Chronic pancreatitis
- Pancreatic obliteration after severe, acute pancreatitis
- Pancreatic tumors
- Celiac disease
- Diabetes
- IBD
Managing nutrition in cystic fibrosis: the role of the pediatric gastroenterologist — Sarah Jane Schwarzenberg, M.D. (page 41)
Good nutrition status correlates with better heights, better lung function, and better survival. (Presentation did not delve into the issue of potential reverse causation.)
- Patients with a Weight-for-Age percentile >50% at age 4 years reached a much higher height-for-age early in life and maintained this advantage into adulthood
- Pulmonary function (FEV1%predicted) was much lower in CF patients with WAP<10% at age 4 years. This finding tracked through age 18 years.
- Small bowel overgrowth is common in CF
- Small bowel bacterial overgrowth contributes to poor nutritional intake and increased nutrient losses
Options to improve nutrition in CF
- Review and optimize enzyme dose and adherence
- Review patient’s diet with an experienced CF dietician
- Consider adding a PPI to improve intestinal pH
- Consider confounding disease
- Evaluate for signs and symptoms of small bowel overgrowth and consider trial of metronidazole or rifaximin
- Ask patient about abdominal pain
- Evaluate for gastroparesis
- Evaluate for DIOS
- Consider non-CF gastrointestinal disease
- Consider oral glucose tolerance test
Therapy to improve nutrition
- Time-limited interventions
- Behavior therapy to improve intake
- Offer oral supplements
- Consider cyproheptadine as an appetite stimulant
- Consider a G-tube for nocturnal feeds
- Consider Endocrinology consult
Beyond the Basics in the Management of Pancreatitis –Aliye Uc, M.D. (page 51)
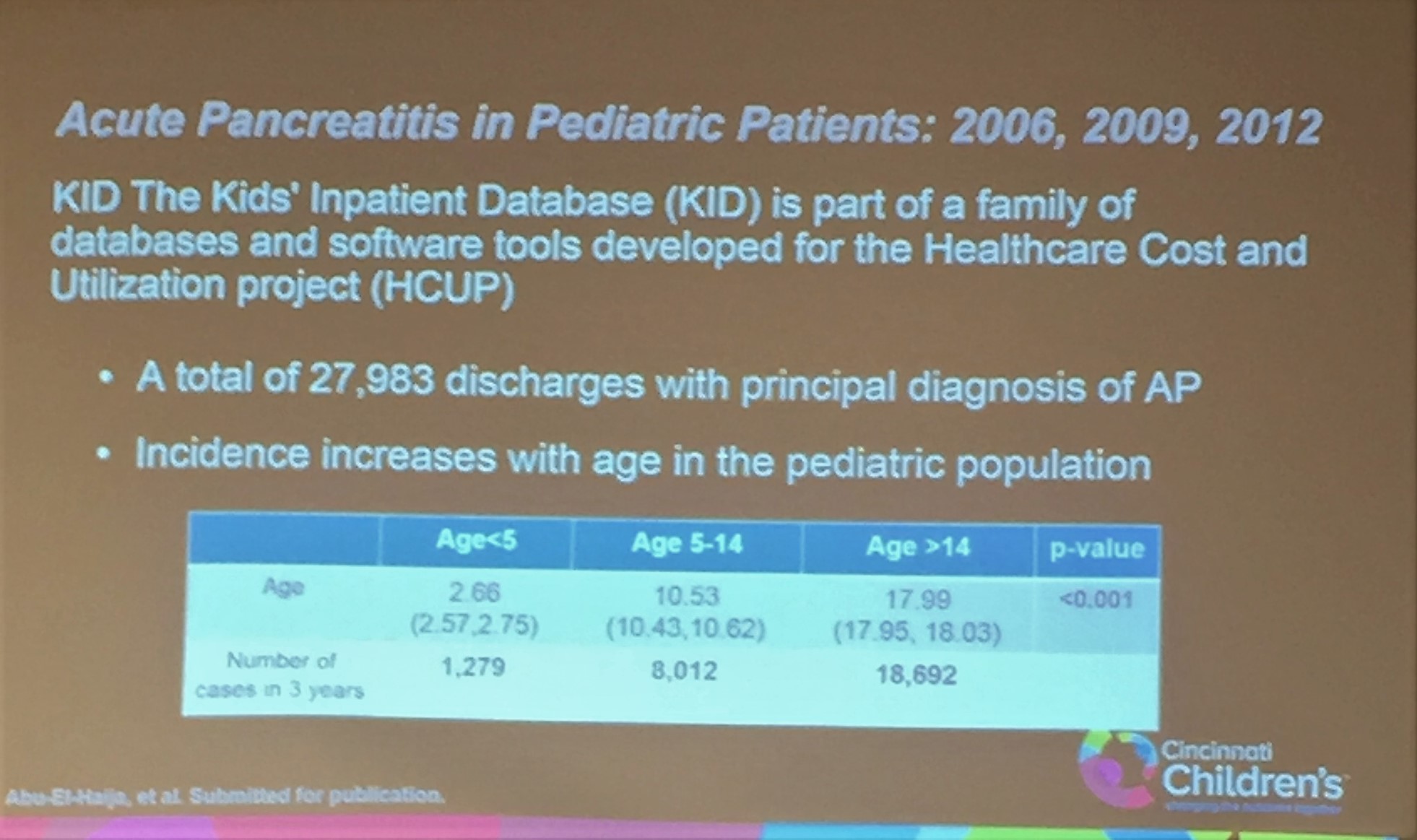
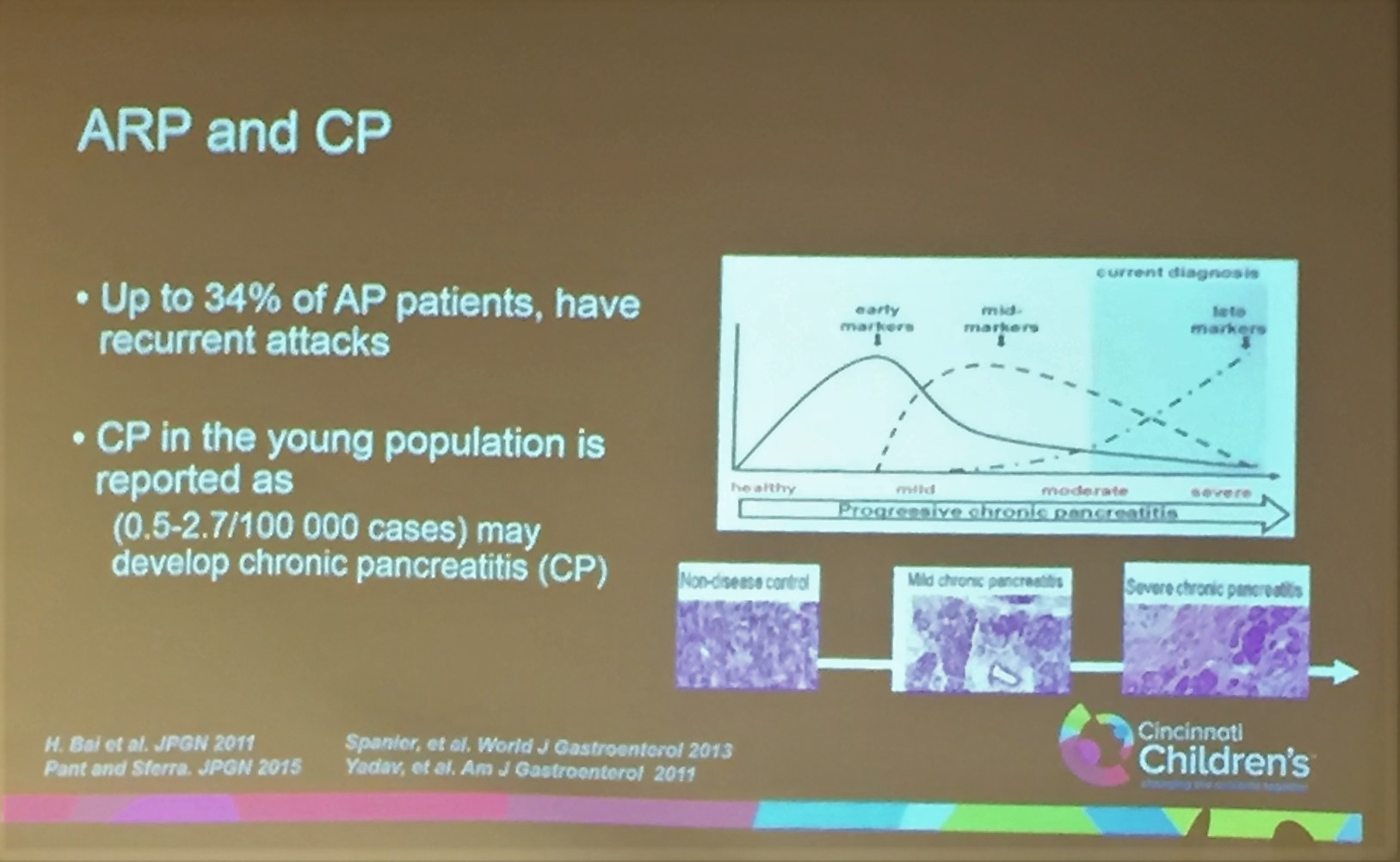
INSPPIRE To Study Acute Recurrent and Chronic Pancreatitis in Children-180 children from 14 centers enrolled to study the etiologies, epidemiology, natural history and outcome.
Pediatric Acute Recurrent and Chronic Pancreatitis-etiologies
- Genetic (49%) (61 of 91 tested)
- PRSS1-30%, CFTR-22%, SPINK1-14%, CTRC-3%
- Obstructive (34%)
- Idiopathic (20%)
- Toxic-Metabolic (17%)
- Autoimmune (3%)
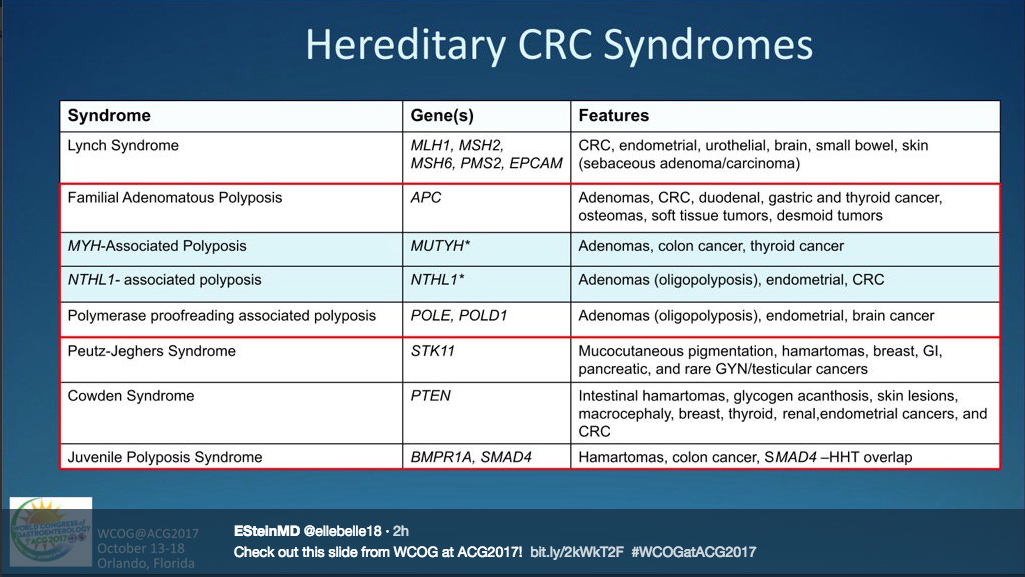
Genetics of Pancreatitis:
1. PRSS1 (cationic trypsinogen): Autosomal dominant, 80% penetrance, Mutations are due to increased activation or decreased inactivation of trypsin (i.e. R122H, N29I).
2. SPINK1 (trypsin inhibitor): Autosomal recessive/complex inheritance, 2% have mutation, <1% have pancreatitis (i.e. N34S), Pancreatitis is dose-related (homozygous>>>het), Associated with other mutations (CFTR)
3. CFTR (>1700 mutations):
- 2 Severe mutations = Cystic Fibrosis
- 1 severe, 1 mild mutation = mild or atypical CF, ARP, CP
- CF carriers = 3-4 fold increase risk in pancreatitis.
- 1 any +SPINK1 = CFTR-associated pancreatitis
- 1 any +divisum = CFTR-associated pancreatitis
4.New Modifier Genes in ARP and CP
- CTRC (trypsin degrading enzyme)
- CASR (a calcium-sensing receptor)
- CLDN2 (tight junction protein on X chromosome)
- CPA1 (Carboxypeptidase 1) increased riskf for CP in younger patients
Management:
- Unclear if antioxidants helpful for pain.
- The role of pancreatic enzymes in CP is equivocal.
Diet
- When to start feeds? depends on the severity of AP, OK to start early; correlate with clinical readiness, abd pain
- What mode of nutrition? prefer enteral over TPN, NG vs. NJ
- What to feed? recent studies in adults with mild AP support full diet
(Moraes JM et al. J Clin Gastroenterol 2010 44:517)
No evidence that low-fat diet is helpful
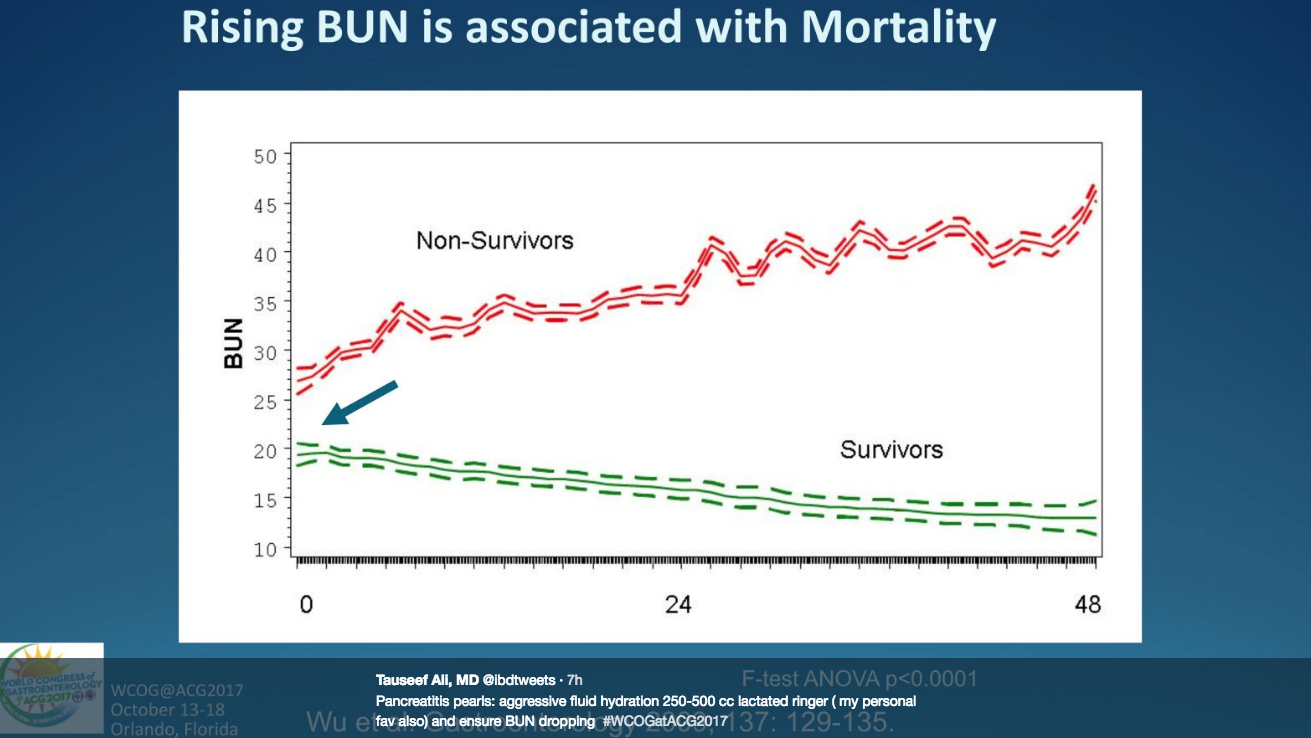
IV Fluids: With acute presentation, Lactated Ringer’s preferred over Normal saline.
NG Suction
- Not shown to decrease symptoms,mortality or hospital stay.
- May be useful if: severe gastric distention, refractory nausea and vomiting, or obstruction seen on abdominal x-ray