At bottom of post, more information on COVID-19.
——————————————————-
At a recent Pharmacy, Nutrition, and Therapeutics (PNT) meeting, one of the topics that we reviewed was injectable iron agents, primarily iron sucrose (Venofer ®) and ferric carboxymaltose (Injectafer®). Iron dextran is mainly used as a supplement in parenteral nutrition in our patient population.
Also, this topic is reviewed in Practical Gastroenterology Jan 2020 (M Auerbach et al. January 2020 • Volume XLIV, Issue 1: Treatment of Iron Deficiency in Gastroenterology: A New Paradigm
Key points:
- Venofer® is much less expensive and currently has an FDA indication for children. To provide 1500 mg, Venofer®, 5 doses of 300 mg (~$75/dose)~$375. Injectafer®, 2 doses of 750 mg (~$600/dose) ~1200. This does not include potential travel and other ancillary costs.
- Dosing: Injectafer® can give large amounts of iron; in adults, typical dose is 750 mg given 7 days apart (in children 15 mg/kg/dose with 750 mg max). FDA approved method is to administer over 15 minutes. Venofer® in children is 5-7 mg/kg/dose with 300 mg max per dose.
- Injectafer® has been associated with hypophosphatemia (in 27%, <2 mg/dL); Hypophosphatemia has also been reported with iron sucrose. The reported incidence of hypophosphatemia is higher with ferric carboxymaltose vs iron sucrose.
- Other Adverse Effects:
| Iron Sucrose (Venofer®) | Ferric Carboxy (Injectafer®) | |
| Nausea | 8.6% | 7.2% |
| Vomiting | 5% | 1.7% |
| Diarrhea | 7.2% | <1% |
| Dizziness | 6.5% | 2% |
| Hypertension | 6.5% | 3.8% |
Oral vs IV Iron for IBD: Auerbach et al recommends that “iron should only be given orally to IBD patients with inactive disease, mild anemia, and good tolerance of oral iron; in patients with active IBD oral iron should be avoided.” They state that “oral iron has been shown to exacerbate intestinal inflammation of IBD independent of anemia, and cause luminal changes in microbiota and bacterial metabolism, which may negatively alter the microbiome.” (Has IV iron’s effect on the microbiome been studied/compared to oral iron?)
Safety of intravenous iron: “In a recent meta-analysis, the results of more than 10,000 patients who were treated with intravenous iron were reported. Compared to oral iron, placebo, and even intramuscular iron (which should never be given), while minor infusion reactions were observed with IV iron, there was no increase in serious adverse events compared to any comparator including placebo.”
My take: Injectafer® is likely preferable to Venofer® in the outpatient setting as adequate dosing can be given in 1 or 2 infusions.
Related blog posts:
- CHOP QI: Anemia in IBD Pathway Link: CHOP Algorithm
- Is It Right? Anti-TNF Therapy Does Not Fix IBD-Related Anemia
- Be Aggressive! Treating Anemia Associated with Inflammatory Bowel Disease | gutsandgrowth
- Microcytic Anemia Review | gutsandgrowth
- IBD Update January 2015 (Part 2) | gutsandgrowth
- Help with hepcidin | gutsandgrowth
- Inadequate treatment of anemia in IBD | gutsandgrowth

Trail on Blood Mountain
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
————————————
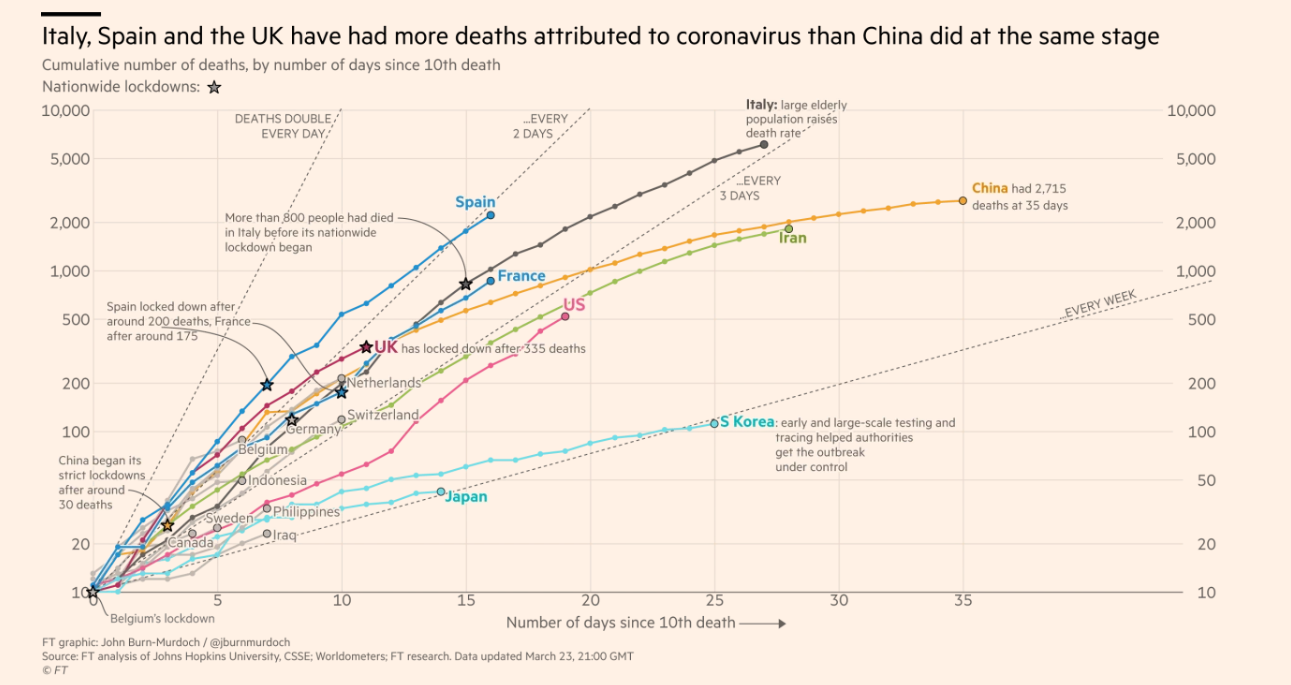
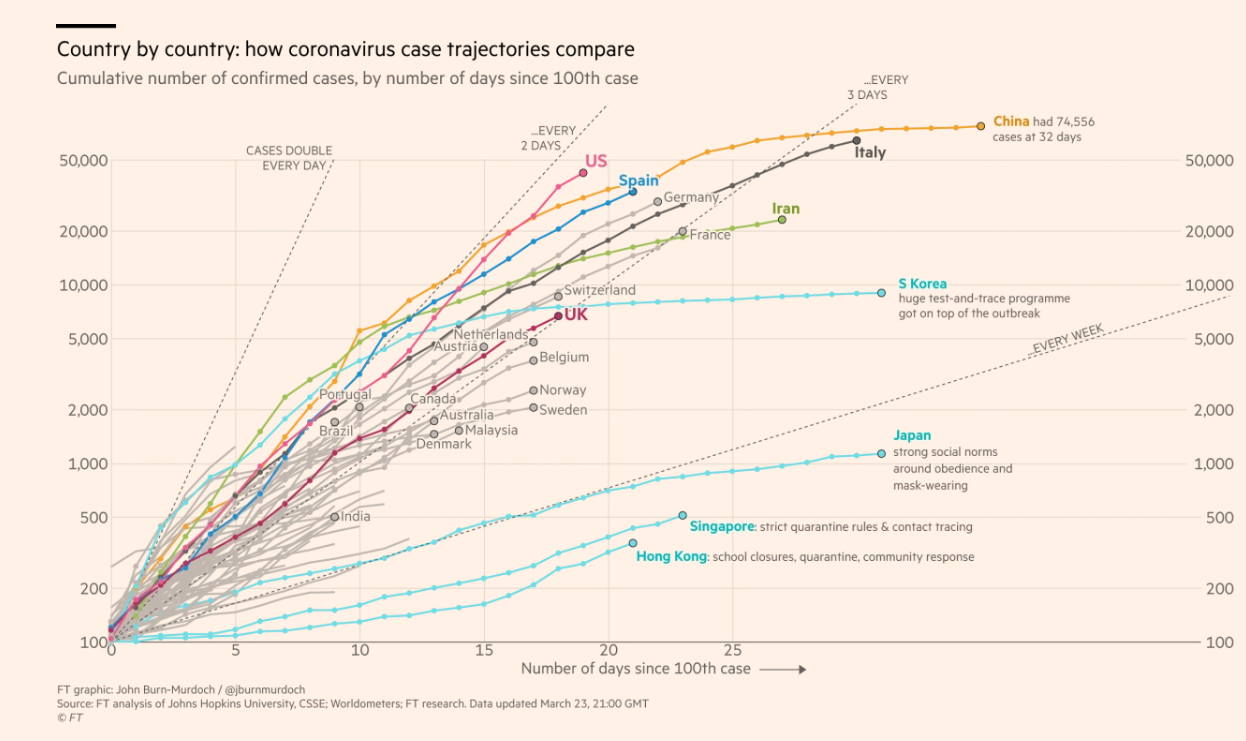
Here’s a link to Financial Times COVID-19 Tracker –includes logrithmic charts plotting the rates of reported infection and deaths and allows quick comparison between countries and high-volume locations (eg. Madrid, Lombardia, NY City). Some figures from March 23, 2100 GMT noted below; unfortunately, the U.S is likely to the world leader in number of reported cases quite soon.
- Financial Times: Coronavirus tracked: the latest figures as the pandemic spreads | Free to read
- From Johns Hopkins: COVID19 Caseload & Outcomes Worldwide
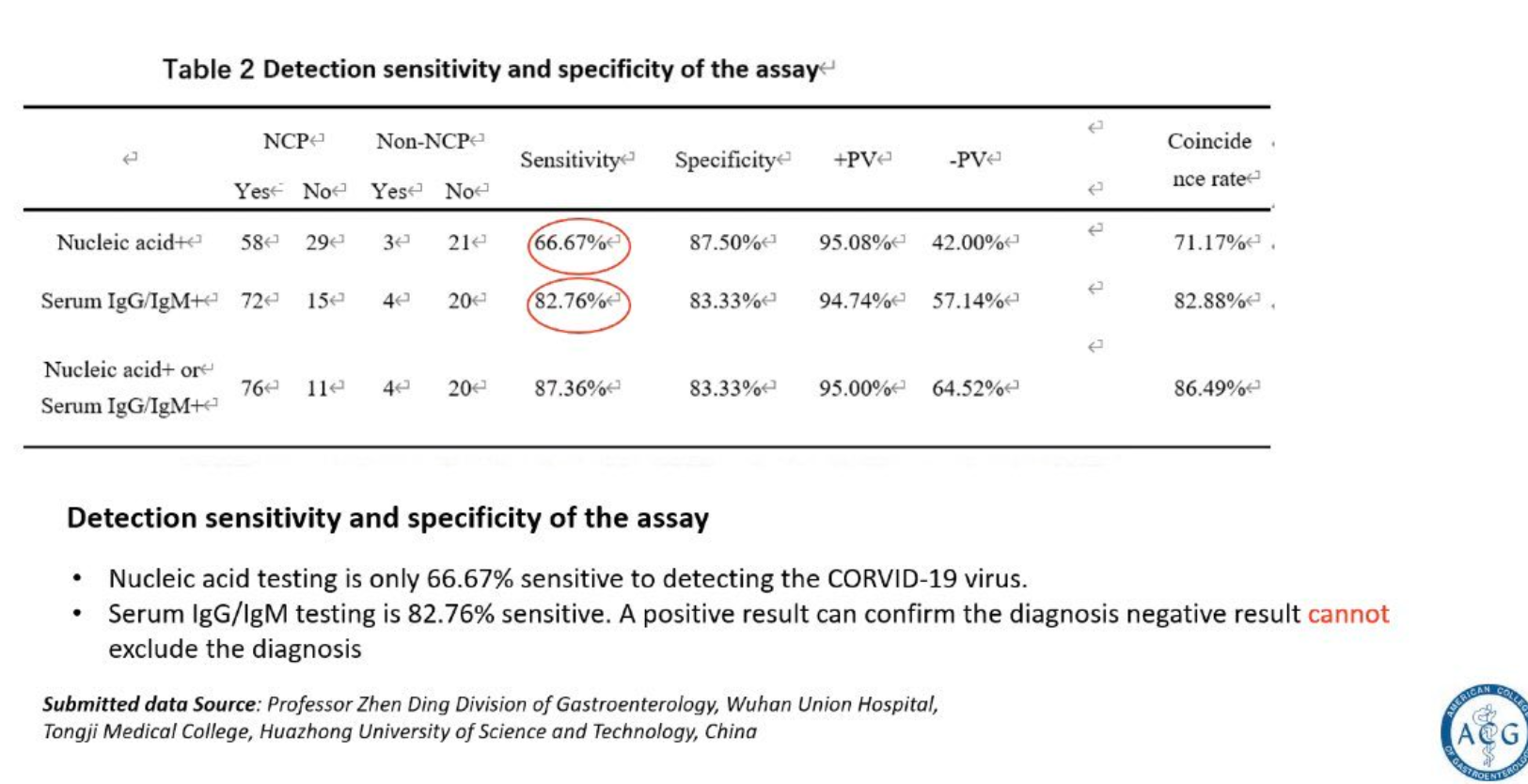
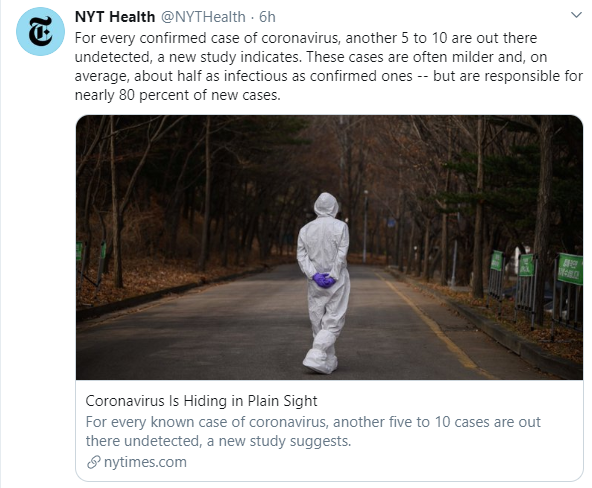
Other relevant tweets: