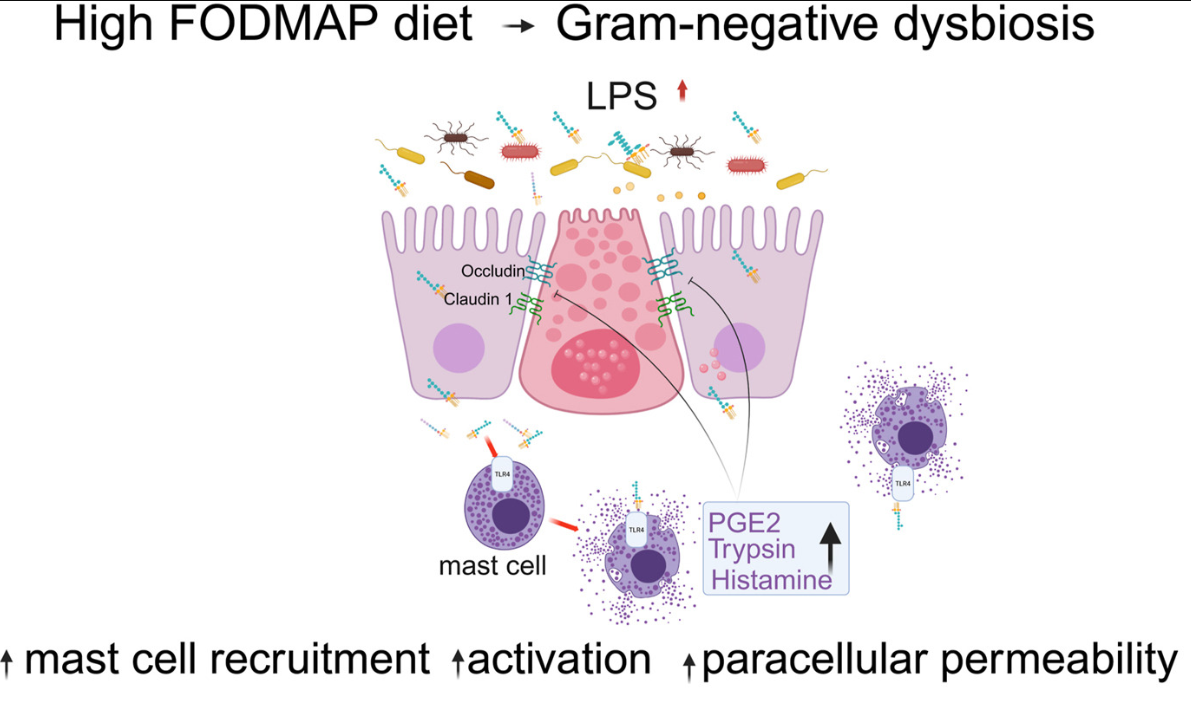
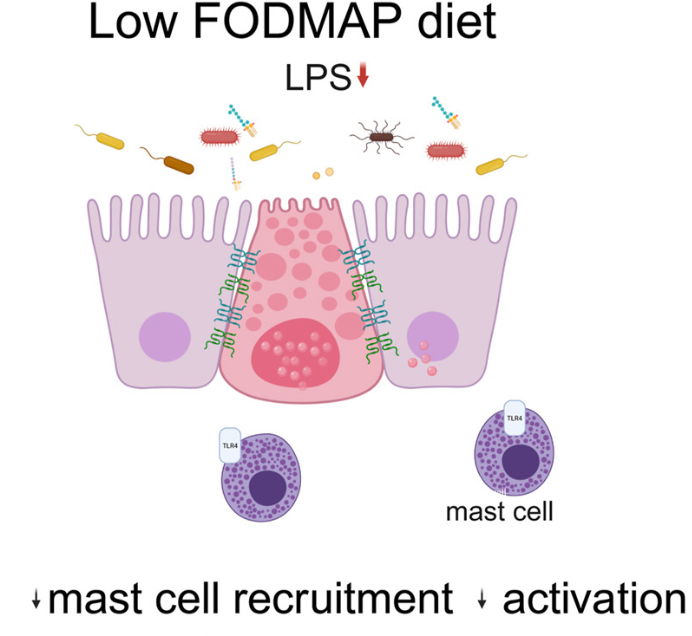
Background: “Mechanisms by which fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) drive pathophysiology of irritable bowel syndrome (IBS) are not well understood.”
Methods: 42 patients with “Rome IV diarrhea-predominant IBS (IBS-D) underwent barrier function evaluation pre- and post-LFD along with assessment of mast cell number and activation profile. Finally, fecal supernatants (FS) were administered intracolonically to wild-type mice with and without pharmacologic inhibition, toll-like receptor 4 (tlr4)–/– mice, and mast cell-deficient mice with/without mast cell reconstitution.”
Key findings:
This is a highly technical study and would recommend reviewing the findings directly (open access article).
To summarize:
“Patients with IBS-D had significant improvement in colonic barrier structure and function, mast cell number, and levels of mast cell mediators post-LFD (low FODMAP diet). The magnitude of physiological changes did not correlate with the magnitude of clinical response.”
“This study showed the complex interplay among food, microbiome, local immune activation, and epithelial physiology in IBS by demonstrating that FODMAPs increase fecal lipopolysaccharide levels, which activates colonic mast cells to causes barrier dysfunction in diarrhea-predominant IBS.”
My take: By understanding the GI effects of a low FODMAP diet in patients with IBS-D more precisely, it may improve dietary approaches as well as other treatments like mast cell stabilizers.
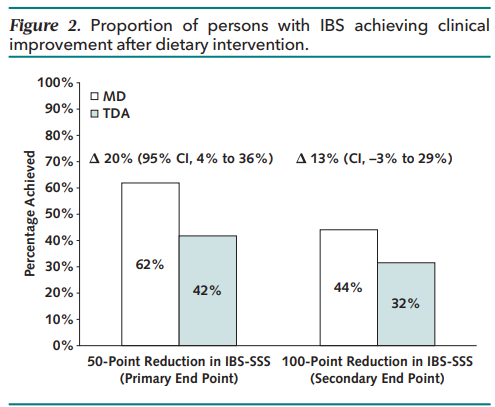
Methods: Randomized noninferiority clinical trial (n=139 Adults from UK) — 6 weeks of the MD (Mediterranean diet) (n = 68) versus TDA (traditional diet advice) (n = 71). Primary end point was the proportion achieving clinical response, defined as 50-point or greater reduction in IBS Symptom Severity Scale (IBS-SSS).
Traditional dietary advice’s main elements are to “adopt sensible eating habits and avoid excess fatty foods, spicy foods, processed foods, caffeine, fizzy drinks, and alcohol. The principal components of the MD are a diet rich in fruit, vegetables, pulses (aka legumes), whole grains, nuts, fish, and olive oil.”
Key findings:
The primary end point was met by 62% following a MD versus 42% following TDA (P = 0.017)
There was a greater reduction in the mean IBS-SSS after a MD than TDA (−101.2 vs. −64.5)
My take: I agree with the authors: The Mediterranean diet “represents a viable first-line dietary intervention for IBS.”
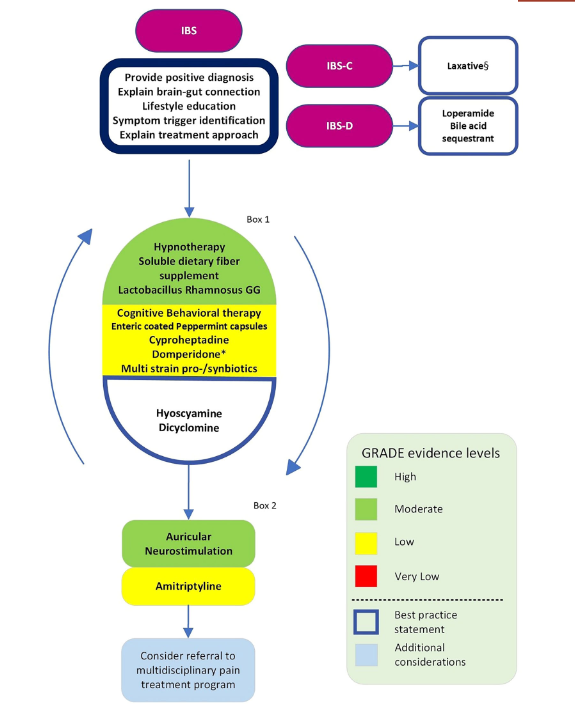
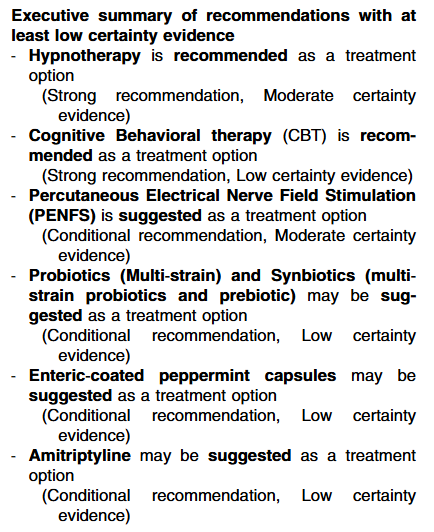
Overall, this article notes that the evidence based for most treatments for pediatric irritable bowel (IBS) is often lacking.
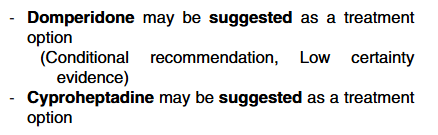
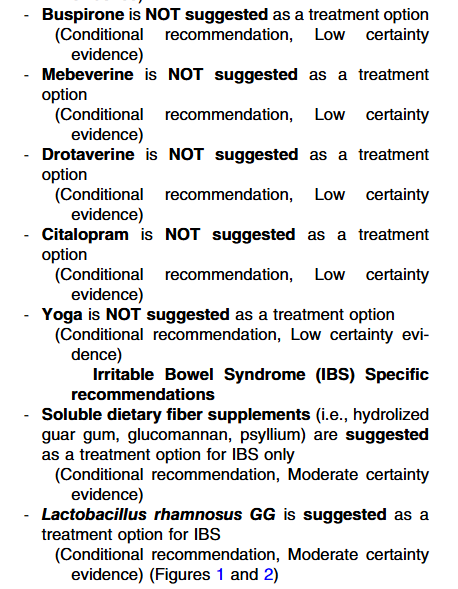
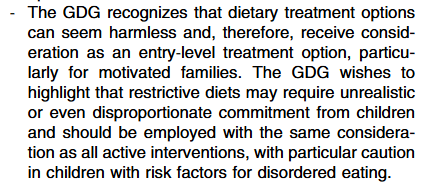
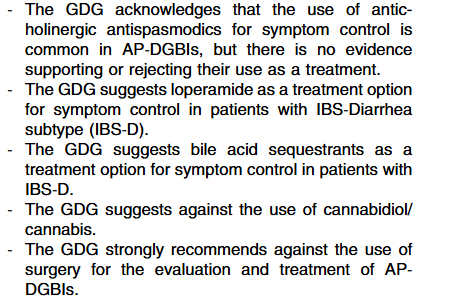
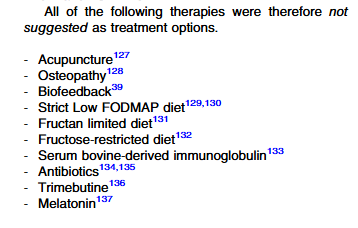
Specific recommendations:
Executive summary of Best Practice Statements‐ The Guideline Development Group (GDG) notes that a crucial emphasis should be placed on education regarding the abdominal pain‐related disorders of gut–brain interaction.
My take: This is a helpful guideline and likely to influence practice.
Methods: From May 2020 to May 2022, the authors performed a series of cross-sectional online surveys among a representative sample of adults ≥ 18 years old in the US (n=160,154). We administered Rome IV gastroduodenal and bowel DGBI questionnaires.
Key findings:
During the COVID-19 pandemic, the prevalence of irritable bowel syndrome (IBS) increased from 6.1% [May 2020] to 11.0% [May 2022]
In addition, the prevalence of chronic idiopathic constipation (CIC) increased mildly from 6.0% [May 2020] to 6.4% [May 2022]
No changes in prevalence were seen for the other examined gastroduodenal and bowel disorders of gut-brain interaction (DGBI)
My take: This study identified increases in the prevalence of IBS during COVID. Increases in IBS following other enteric infections (eg. norovirus, shigella, campylobacter) has been shown previously as well.
This study used transgenic, surgical, and pharmacological approaches to study the effects of intestinal epithelial serotonin reuptake transporter or serotonin on mood and gastrointestinal function, as well as relevant communication pathways.
Key findings:
Serotonin reuptake transporter ablation targeted to the intestinal epithelium promoted anxiolytic and antidepressive-like effects without causing adverse effects on the gastrointestinal tract or brain; conversely, epithelial serotonin synthesis inhibition increased anxiety and depression-like behaviors.
In utero SSRI exposure is a significant and specific risk factor for development of the DGBI, functional constipation, in the first year of life.
My take: While this lengthy article presents data mainly from mice studies, it further supports the likelihood that SSRI selective targeting of the gut epithelium may improve anxiety, depression and comorbid DGBI. Selective targeting of the GI tract would reduce adverse effects of these medications.
In the movie There’s Something About Mary, there is a scene (YouTube: 7-minute abs) where the main character picks up a hitchhiker. The hitchhiker reveals his brilliant idea for the 7-minute ab workout to replace the 8-minute ab workout. Of course, he becomes upset when the lead character suggests that someone else could invent the 6-minute ab workout.
This is what I was thinking of when I read a recent article describing a simplified, less restrictive low FODMAP diet.
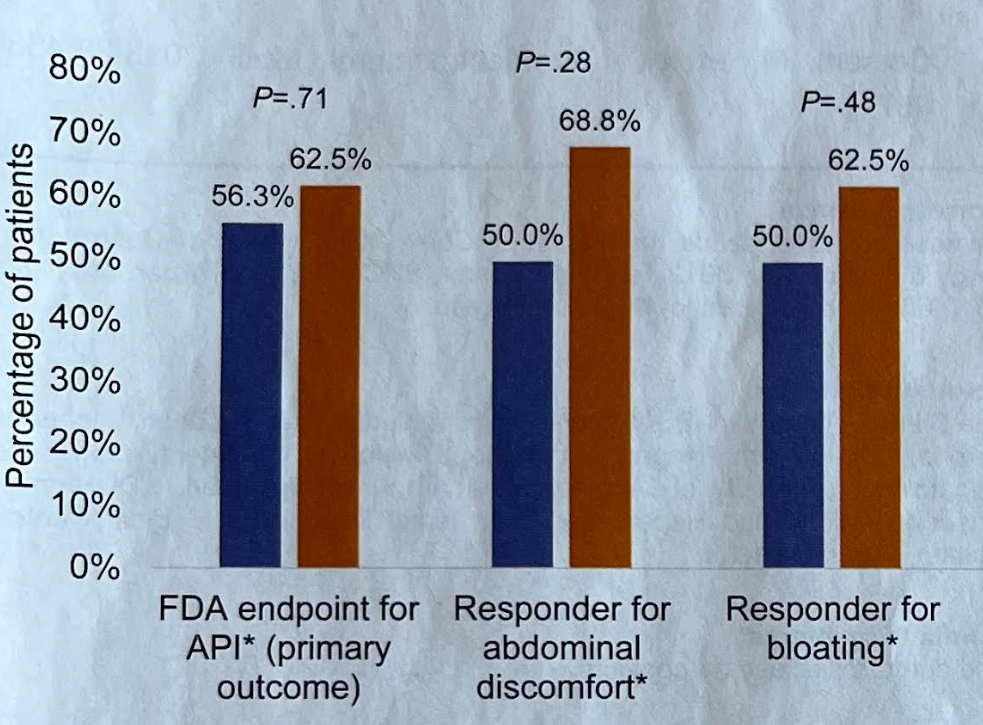
This pilot study with 35 subjects with IBS-D were randomized to a standard low FODMAP diet (LFD) or to a simplified FODMAP diet which eliminated solely fructans and galactooligosaccharides. The primary endpoint was the proportion of subjects meeting the FDA responder definition for abdominal pain intensity (ie. a >/= 30% reduction in weekly average of daily abdominal pain scores for 2 of the 4-week treatment period).
Key findings:
There was a similar reduction in key symptoms (see below)
Fewer individuals in the simplified diet dropped out due to side effects or difficulty with adherence (12.5% vs 26.3%)
Blue columns indicate response to traditional low FODMAP diet (n=19) and orange represents response to simplified low FODMAP diet (n=16)
My take: Larger trials are needed. This study suggests that a simplified version of a low FODMAP diet would improve symptoms in most patients with IBS-D.
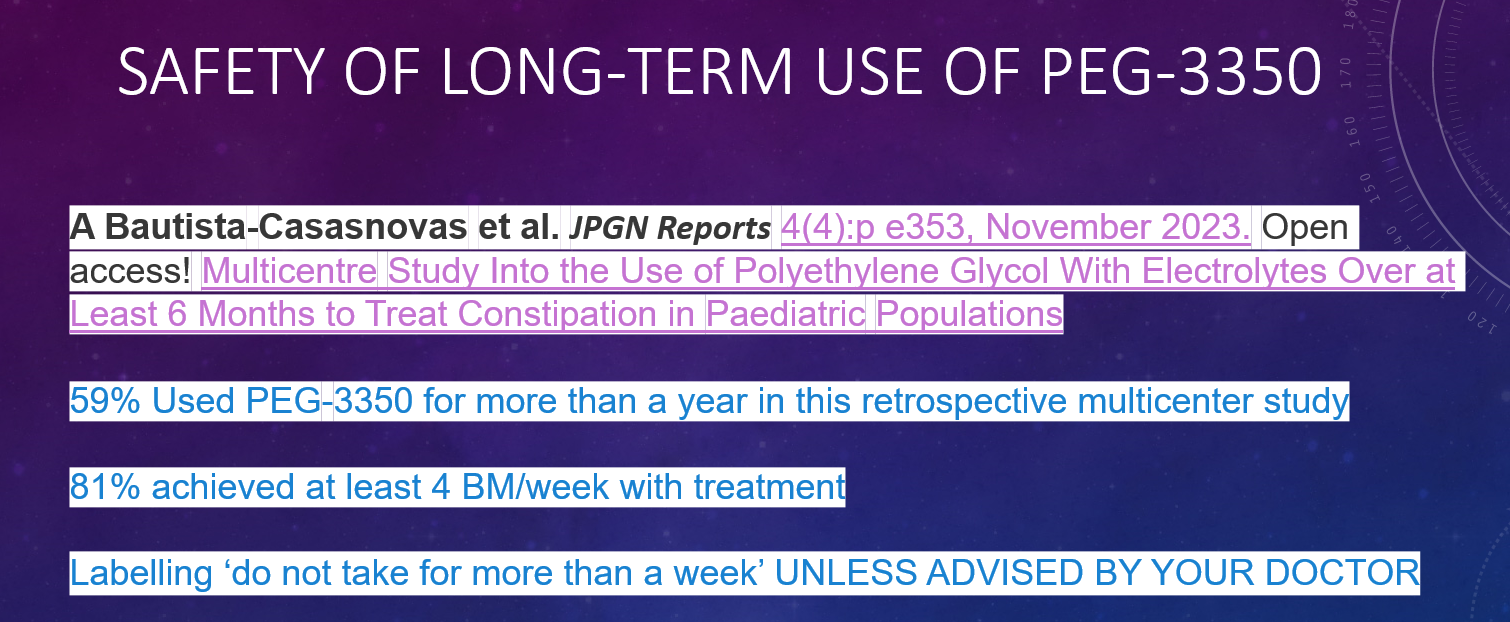
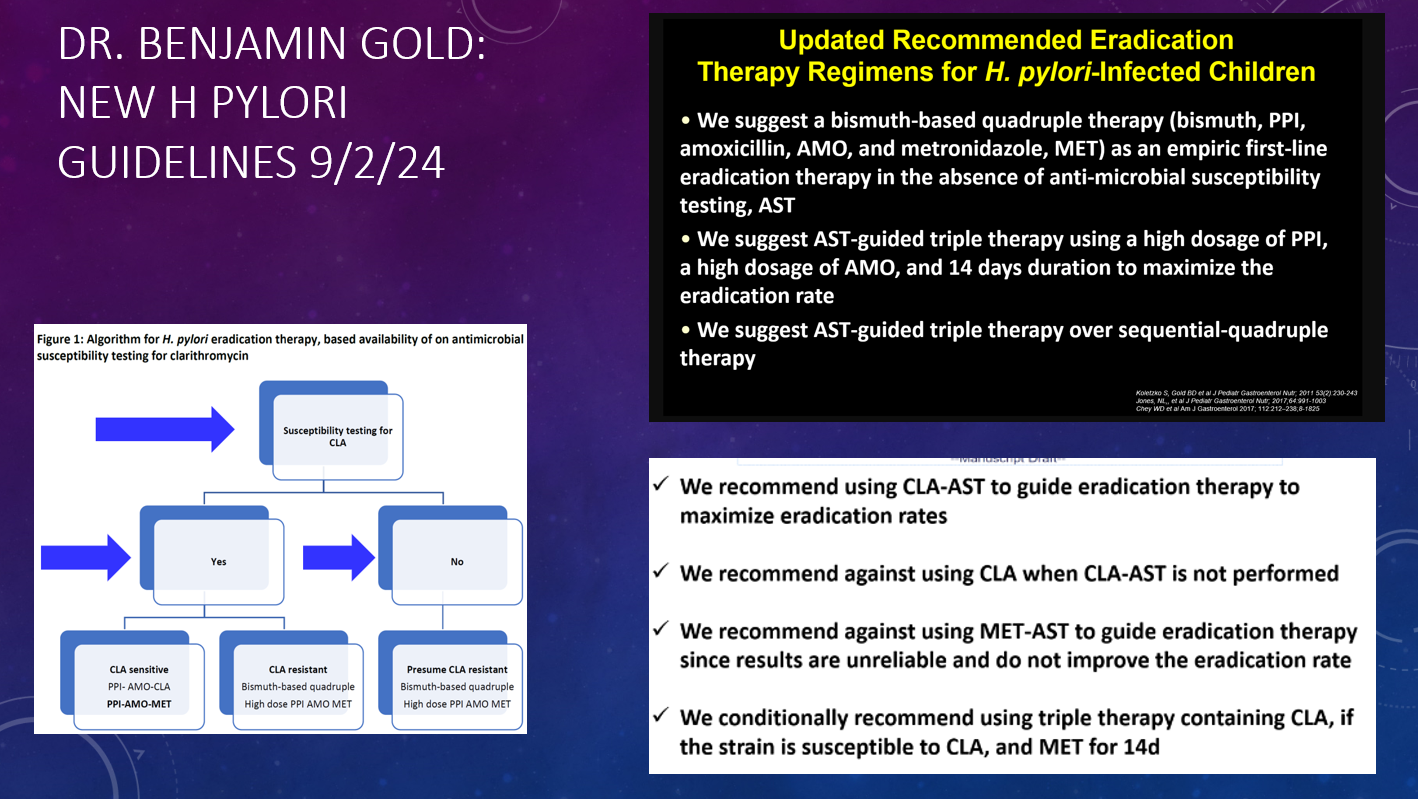
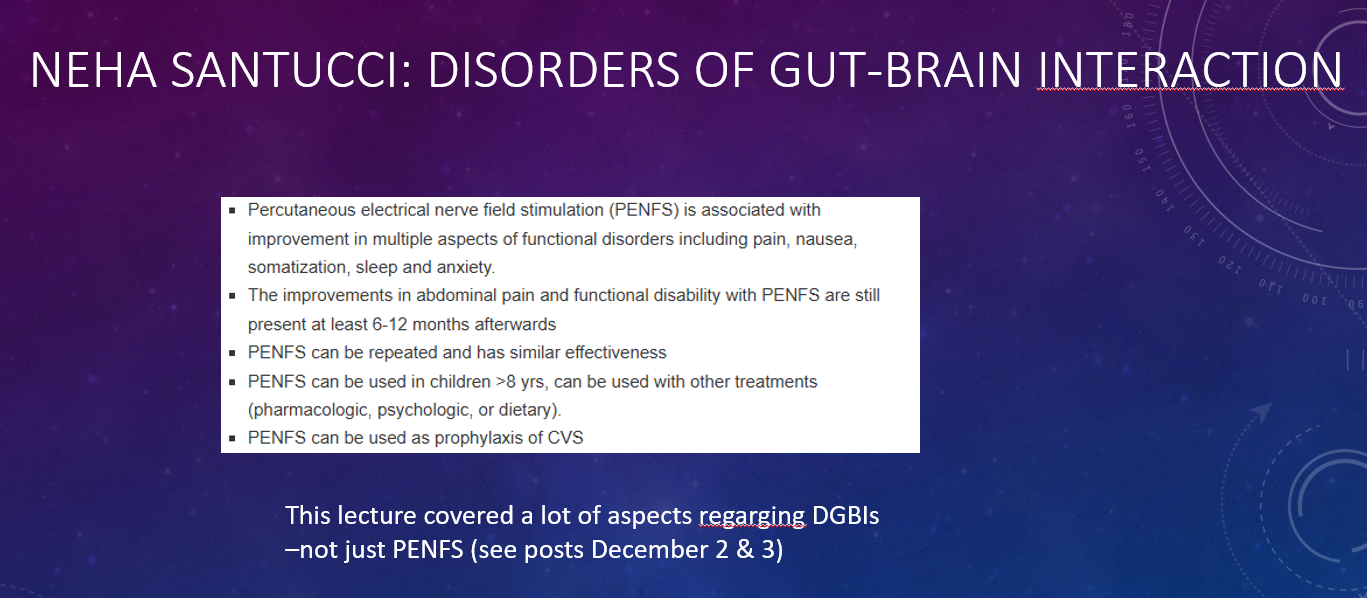
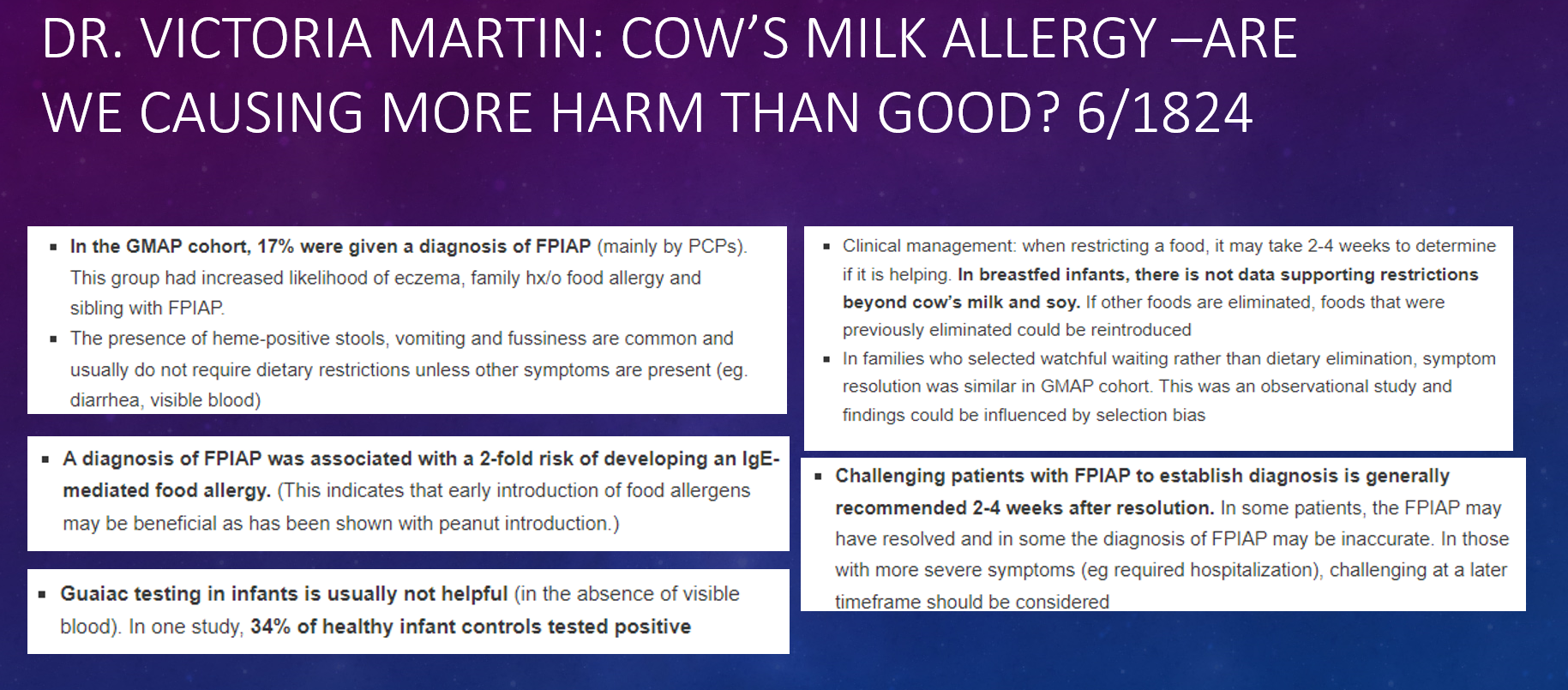
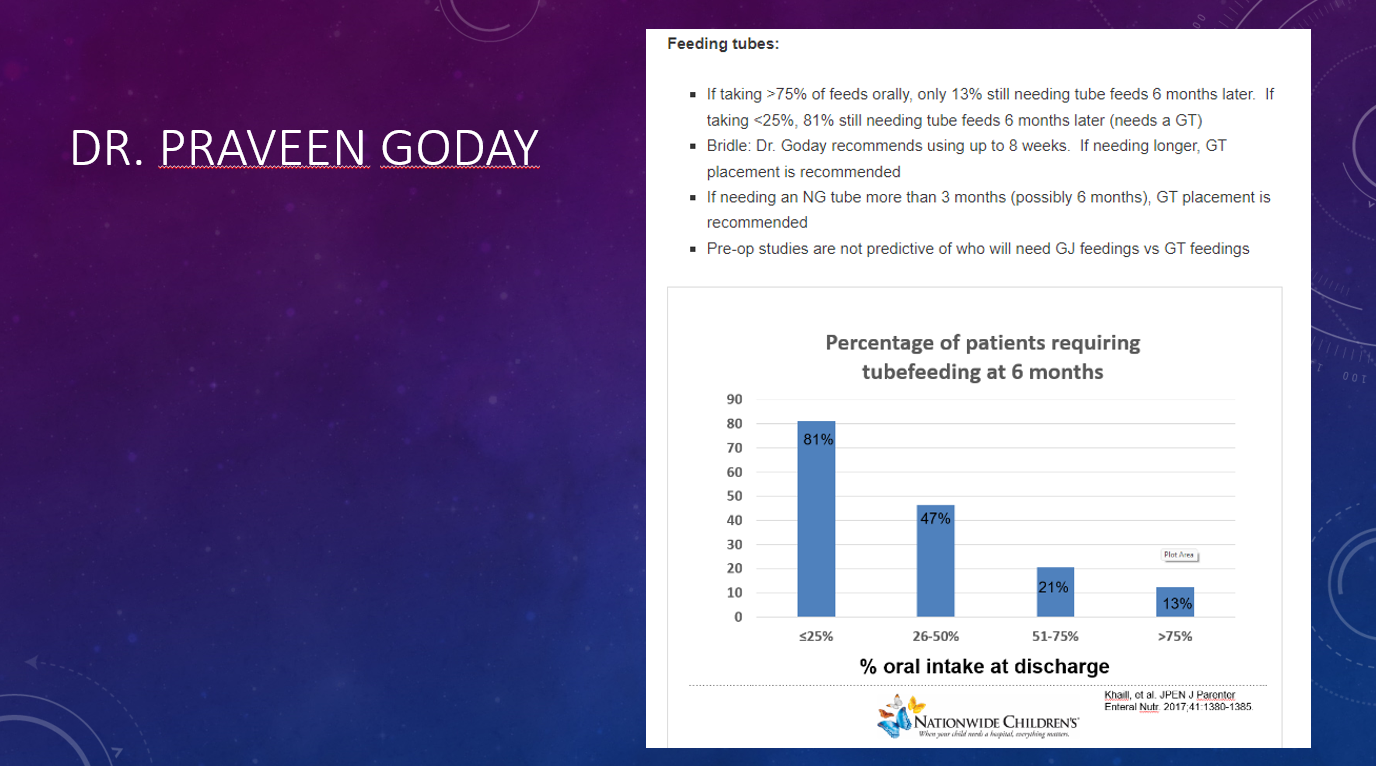
This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
This study examined markers of the epithelial and vascular barriers in 223 patients with irritable bowel syndrome in comparison to 78 healthy subjects. In actuality, this lengthy report was a composite of about 8 different experiments.
Key findings:
Figure 2 summarizes in vivo and in vitro epithelial permeability testing using orally-administered sugars and using Caco-2 cell incubation of control/IBS supernatants. In all of these experiments, there was a significant mean increase in IBS-D permeability compared to controls.
Figures 3 and 4 report on significant changes the gut vascular barrier and specific mediators, respectively, in IBS compared to controls
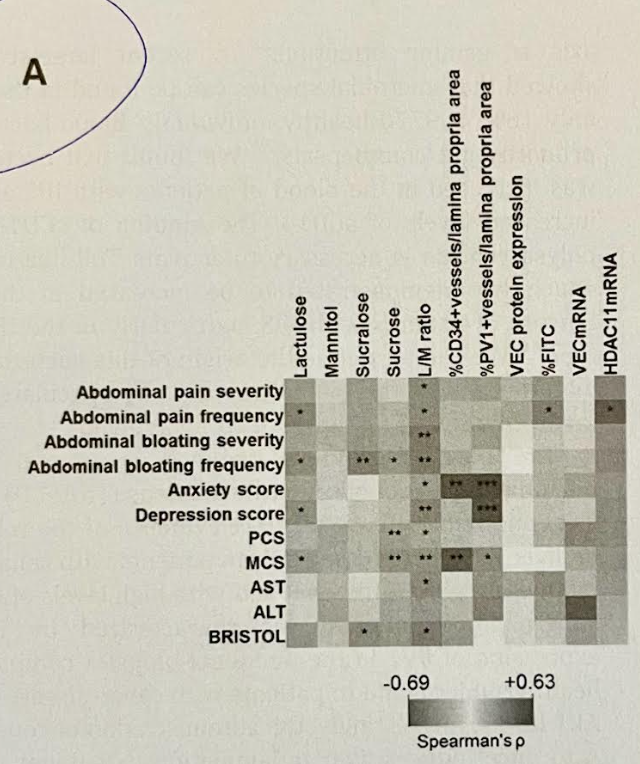
One novel finding was correlation of epithelial barrier markers with gastrointestinal symptoms and gut vascular dysfunction with systemic systems including anxiety and depression (see heat map below)
Relationships between epithelial and endothelial permeability markers and symptoms. The asterisks on the heatmap indicate significances in the Spearman’s correlation.
My take: The term ‘leaky gut’ has a negative connotation among many gastroenterologists as it has been associated with misleading diagnostic and therapeutic claims. However, this study shows a correlation between epithelial and vascular barrier disruptions and symptoms in irritable bowel. This is useful information; nevertheless, there are not simple tests to identify these findings and there are not therapeutics with demonstrated efficacy.
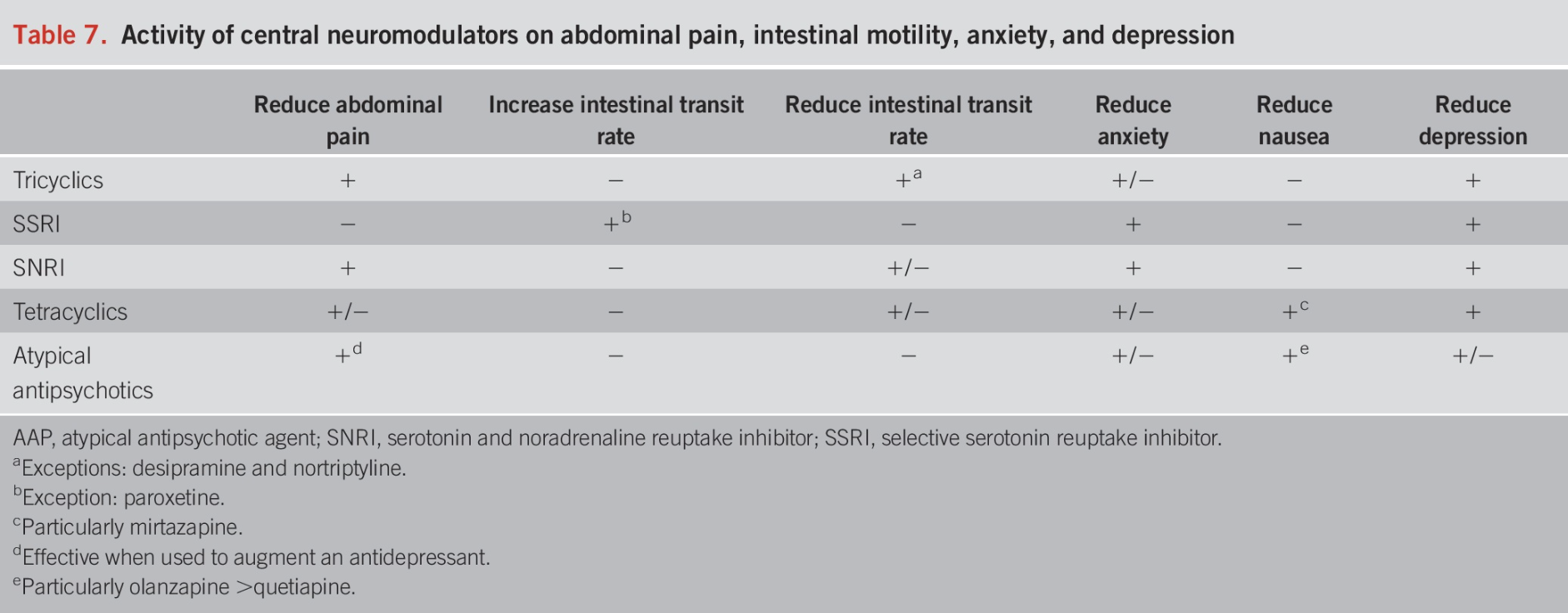
This is a terrific review article. The authors detail the rationale for neuromodulators, strategies for selecting among them, side effects, and dosing.
Background: “IBS is frequently associated with neuropsychiatric disorders such as depression and anxiety, which are considered triggers for the onset of symptoms or occur in response to having them (3). In the Rome Foundation global study that included 54,127 participants, subjects with psychological distress or clinically relevant somatic symptoms were 4.45 times more likely to have 1 or more DGBI than those without psychological distress. The same study reported that those who met specific criteria for bowel disorders presented clinically relevant psychological distress or somatic symptoms in 55.5% of cases (4). In addition, in a meta-analysis that included 7,095 subjects with IBS exclusively, the global prevalence of depression was 36%…Anxiety was present in 44% of patients with IBS….Central neuromodulators act on receptors along the brain-gut axis, so they are useful in treating psychiatric comorbidities, modifying gut motility, improving central downregulation of visceral signals, and enhancing neurogenesis in patients with IBS… Neuromodulator treatment is still considered off-label, many of the recommendations herein are based on expert consensus (6)”
Key points:
“The first-line treatment for pain management in IBS is using tricyclic antidepressants.” Nortriptyline and desipramine are less likely to cause constipation.
“Selective serotonin reuptake inhibitors (SSRIs) are useful when symptoms of anxiety and hypervigilance are dominant but are not helpful for treating abdominal pain….The SSRIs include fluoxetine, fluvoxamine, sertraline, paroxetine, citalopram, and escitalopram. …Sertraline, citalopram, and escitalopram tend to have the fewest pharmacokinetic drug interactions”
“SSRIs are first-line pharmacologic agents for treating anxiety disorders, but they have the potential to induce restlessness and exacerbate anxiety when the drug is initiated. They are typically initiated at half of the usual starting dose to minimize these potential anxiogenic adverse effects. The dose may gradually increase to the regular starting dose after about 1 week… SSRIs should be considered when a significant component of anxiety without pain is present.”
SNRIs: “In addition to showing benefits with depression and painful disorders, SNRIs have shown significant improvement in anxiety.” Thus, they may be useful as monotherapy for patients with pain and anxiety.
Tetracyclics: “The most representative agent of this class is nirtazapine (Table 5). However, their effects seem to be mainly on anxiety, early satiety, nausea, and other symptoms associated with esophageal and gastroduodenal disorders, so their use in IBS is limited.”
“It is important to explain to the patients, …neuromodulators are not necessarily used for the treatment of depression but are a therapeutic alternative in the management of DGBI. It helps to use the term “neuromodulator” instead of “antidepressant” (6,8) It also helps to clarify that these medications can treat pain and other GI symptoms independent of treating depression, and the dosages are often lower than those used for treating major depression. This will preclude any patient concerns that their symptoms are being underestimated or considered to be in their head (6,8).”
Using central neuromodulators for IBS requires long-term treatment. From our experience, 6–12 months of treatment or more are needed to increase the likelihood of remission.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
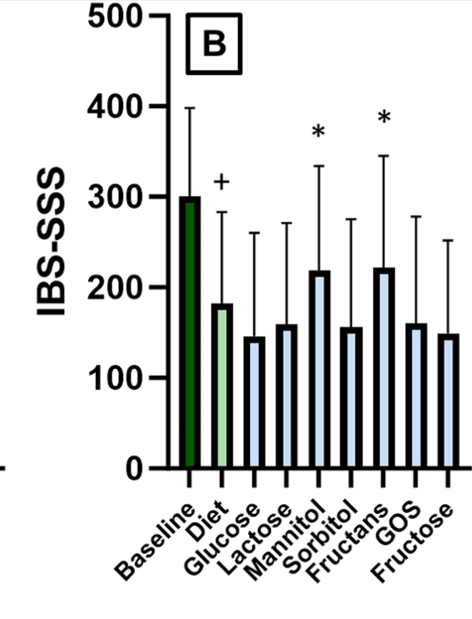
Methods: Responders (n=94 of 117) to a 6-week low FODMAP diet, defined by a drop in IBS symptom severity score (IBS-SSS) compared with baseline, entered a 9-week blinded randomized reintroduction phase with 6 FODMAP powders (fructans, fructose, galacto-oligosaccharides, lactose, mannitol, sorbitol) or control (glucose). A rise in IBS-SSS (≥50 points) defined a FODMAP trigger. Patients were challenged with 6 FODMAPs or glucose as a control (3/day x 7 days) while continuing with the low FODMAP diet. At the end of the seventh day, patients entered 2 days of washout before starting with the next blinded FODMAP or control powder.
Key findings:
IBS-SSS improved significantly after the elimination period compared with baseline (150 vs. 301, P < .0001, 80% responders)
Symptom recurrence was triggered in 85% of the FODMAP powders, by an average of 2.5 FODMAPs/patient
The most prevalent triggers were fructans (56%) and mannitol (54%), followed by galacto-oligosaccharides, lactose, fructose, sorbitol, and glucose (respectively 35%, 28%, 27%, 23%, and 26%) with a significant increase in abdominal pain at day 1 for sorbitol/mannitol, day 2 for fructans/galacto-oligosaccharides, and day 3 for lactose.
One limitation of the study was selecting the dose for the challenge/reintroduction. “In comparison to clinical practice, our selected dose was higher, intended to maximize the potential of inducing symptoms. On the other hand, if that information was available, we aimed to stay below a dose for an individual FODMAP that was shown to elicit symptoms in healthy controls.”
My take:
Fructans and Mannitol had the highest prevalence rate as trigger foods upon reintroduction. However, the other groups all had at least a 23% chance of being a food trigger as well.
Having available powders of the FODMAP grouping could potential expedite and standardize reintroduction in clinical practice. If a patient did well with the specific FODMAP powder, there is a good likelihood that the related foods would be tolerated as well.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.