“According to the CDC, out of every 1,000 children who are infected with measles, one may develop encephalitis, which is a dangerous swelling of the brain. Up to 3 out of every 1,000 infected children will die.
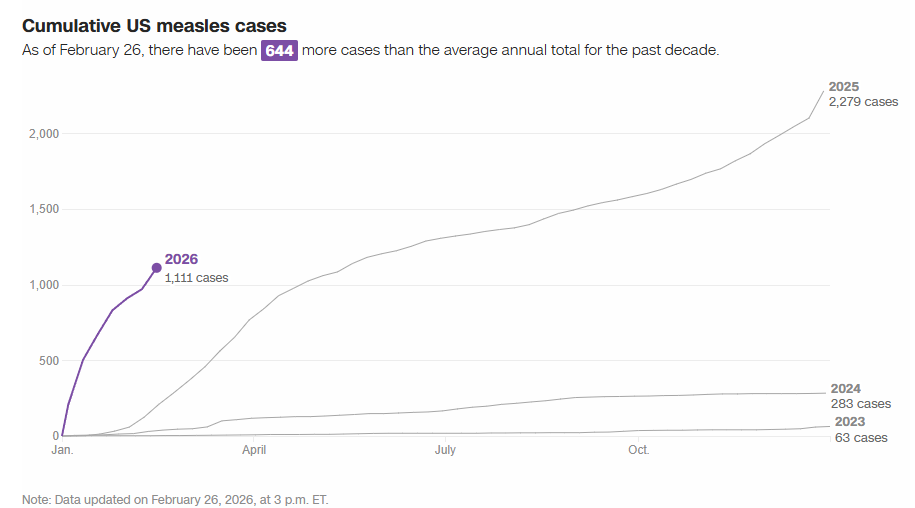
The US is on track for another record-breaking year for measles: The number of measles cases reported in the first eight weeks of the year — 1,136 as of February 26, according to CDC data — is already six times more than typical for an entire year. A tracker from the Johns Hopkins University Center for Outbreak Response Innovation has tallied an even higher the annual case total than the CDC…
New measles cases have started to slow in South Carolina in recent weeks…[due to] ublic health groundwork that has helped rapidly identify cases and potential exposures and drive quarantine guidance…Improving vaccination coverage has also helped, she said. The state health department administered nearly 17,000 MMR vaccines in January, which was one of the most successful months for vaccination that the state has had in years.
Background: “Measles is a highly contagious disease and, despite the availability of a safe and effective vaccine, remains still an important cause of childhood death worldwide [1,2]. The risk of severe illness in measles-naive individuals is particularly high in immunocompromised patients with inflammatory bowel disease (IBD) or after liver transplantation (LT) [3]…Ideally, vaccination with live attenuated vaccines (LAVVs) should be completed four weeks before organ transplantation or the initiation of immunosuppressive therapy (IST) to allow for the live vaccine’s incubation period and minimize the risk of vaccine-associated disease…LAVVs are considered contraindicated during IST due to safety concerns and limited experience.”
Methods: “In this prospective multicenter observational study (DRKS00014569) 22 children and adolescents with incomplete MMR vaccination status were identified… with stable immunosuppressive therapy in the last three months with no evidence of underlying disease activity…Sixteen patients were vaccinated against MMR, eleven after liver transplantation and five with inflammatory bowel disease. At the time of vaccination, four patients were receiving moderate (e.g., tacrolimus drug level below 5 ng/ml), eleven were receiving high-intensity immunosuppression (e.g. anti-tumor-necrosis factor agents, mycophenolate mofetil) and one child had previously discontinued immunosuppressive treatment.”
Immediately prior to the references, the authors provide a downloadable document detailing how they chose to categorize the degree of immunosuppression and their precise protocol, including immunologic pretesting and drug contraindications as noted below.
Key findings:
There were no serious adverse events or complications related to the vaccination
In children receiving immunosuppressive medications, the seroconversion rate for measles after the first MMR vaccination was 73.3 % (11/15) and after the second vaccination 80 % (12/15)
My take: In carefully-selected immunocompromised pediatric patients, the MMR vaccine may be safe. However, given the small numbers receiving vaccination in this study, the absolute safety is unclear. Even infrequent adverse effects would be problematic. This study’s protocol could be helpful for those considering vaccination in immunocompromised populations with a measles epidemic. For now, the most important approach is improving vaccination rates in those (especially family members) without contraindications.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
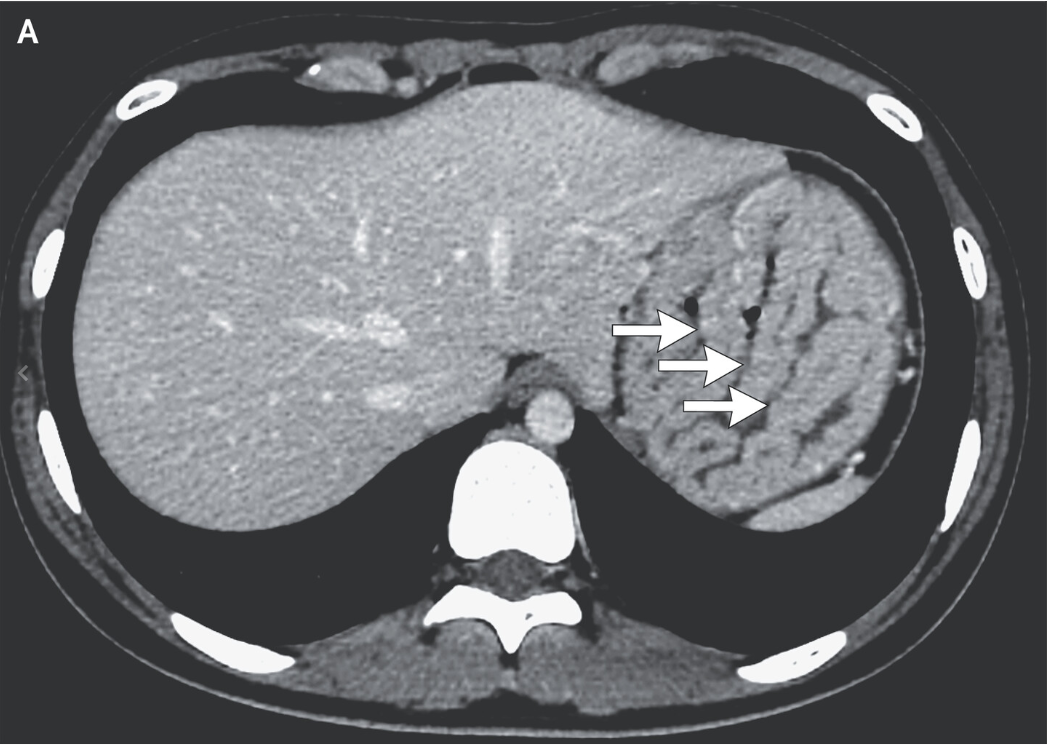
X Wang et al. N Engl J Med 2025;392:1334. Ménétrier’s Disease
History: 16-year-old girl was admitted to the hospital with a 2-month history of leg swelling and hypoalbuminemia. She had no gastrointestinal symptoms.
Treatment: She was placed on a high-protein diet and medications to eradicate a concurrent infection with Helicobacter pylori. At a 3-month follow-up visit, the patient’s edema and hypoalbuminemia had resolved.
Measles as of Friday May 2nd (per Caitlin Rivers): “According to CDC, a total of 935 confirmed measles cases have been reported by 30 jurisdictions. The previous high was 1,274 in 2019. So far this year, 121 cases (13%) have been hospitalized.”
“More U.S. children have died this flu season than at any time since the swine flu pandemic 15 years ago, according to a federal report released Friday…It’s a startlingly high number, given that the flu season is still going on. The final pediatric death tally for the 2023-2024 flu season wasn’t counted until autumn…There are likely several contributors to this season’s severity, but a big one is that fewer children are getting flu shots, added O’Leary, a University of Colorado pediatric infectious diseases specialist. The flu vaccination rate for U.S. children has plummeted from about 64% five years ago to 49% this season. Flu vaccinations may not prevent people from coming down with symptoms, but research shows they are highly effective at preventing hospitalizations and deaths, O’Leary said.”
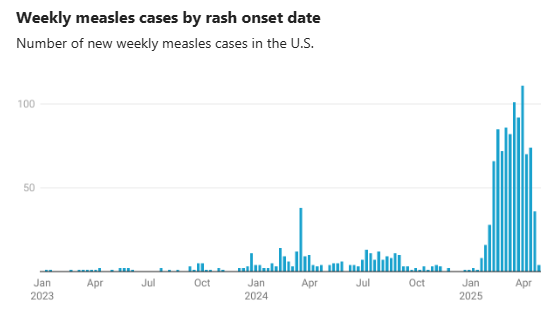
These charts show measles data through April 7th. Some additional data through Apirl 11th is listed below.
For those interested in a deeper dive into the measles numbers, you can follow Caitlin Rivers substack. From her notes on April 11:
“Since my last update on Tuesday, Arkansas and Hawaii reported cases for the first time this year. At least five states have reported ten or more cases, which is very unusual. Texas continues to register the most cases, with 541 to date.”
“According to the CDC, 712 cases have been reported so far this year. 1 in 3 (32%) are under the age of 5, and 1 in 10 (11%) have been hospitalized.”
“Vaccines are the first step toward health equity in many parts of the world…Around the globe the measles vaccine has saved nearly 94 million lives over the past 50 years. This and other vaccinations have revolutionized global health…”
“A May study in the Lancet estimated that vaccines against 14 common pathogens have saved 154 million lives over the past five decades—at a rate of six lives every minute. They have cut infant mortality by 40 percent globally and by more than 50 percent in Africa. Throughout history vaccines have saved more lives than almost any other intervention. And vaccines’ promotion of health equity goes far beyond preventing death. The Lancet study found that each life saved through immunization resulted in an average 66 years of full health, without the long-term problems that many diseases cause. Vaccines play a role in nearly every measurement of health equity, from improving access to care, to reducing disability and long-term morbidity, to preventing loss of labor and the death of caretakers…”
“If you have no money, then you want the best bang for the buck, and it’s going to be immunization,” says Seth Berkley, former CEO of Gavi. “For every dollar you invest in immunization, you get $54 of benefit.”
The reduction in mortality equates to 9·0 billion life-years saved.
“In late 2019, when a novel coronavirus detected in Wuhan, China, kicked off one of the largest, deadliest pandemics in a century, everyone looked to the same solution: a vaccine. COVID’s devastation hit poorer countries with less developed health-care systems particularly hard, and in wealthier countries people from underserved and low-income communities suffered higher rates of illness, death and economic hardship…”
“A 2022 study in the Lancet Infectious Diseases estimates that COVID vaccination worldwide prevented 19.8 million excess deaths.”
My take: This is a terrific article and particularly timely given the growing influence of anti-vax proponents. Not only have vaccines prevented millions of deaths, they have helped prevent chronic complications (eg. disability after meningitis). The reduction in mortality in the charts is likely UNDERESTIMATED. Many other vaccines were not included in this estimation: smallpox, human papillomavirus, (HPV), influenza, SARS-CoV-2, Ebola, mpox and other vaccines.
Why does Mississippi have the best childhood immunization rates (99%)? This is due to state policies. This article reviews the small but significant drops in childhood immunizations which is opening the door for highly contagious diseases like measles.
Some excerpts:
U.S. routine childhood vaccination rates have historically been among the world’s best. But within the first year of the pandemic, the nation’s children missed nine million vaccine doses for diseases like polio and measles. Rates for the three major childhood immunizations — for measles, mumps and rubella; chickenpox; and diphtheria, tetanus and pertussis — fell by an average of 1.3 percentage points, with the rates in seven states and many cities falling under 90 percent…
Measles should not be taken lightly. The virus is highly contagious; according to the C.D.C., if one person has it, up to 90 percent of the people close to that person who are not immune will also become infected. It can live up to two hours in the air. One to three of every 1,000 children who contract measles die of respiratory and neurological complications…
Covid vaccine acceptance and anti-vax attitudes do not fully explain differences among states. Neither do red-blue partisan affiliations or the strength of a state’s public health system. Instead, the decline is rooted in longstanding policies among some states that allow, for instance, for nonmedical exemptions, failures to rigorously enforce vaccination requirements and inadequate public health campaigns…
Vaccines are one of the few true cost savers in medicine. The routine immunizations of children born from 1994 to 2018 are projected to prevent nearly one million early deaths and save nearly $1.9 trillion in economic costs — more than $5,700 for each American, according to the C.D.C. For measles, a state might spend more than $2 million responding to a single outbreak, with each case costing nearly $50,000 on average, according to an analysis of a recent outbreak in Washington State.
To avoid dangerous and costly outbreaks, states should introduce enforceable solutions that give their children and communities the best protections against vaccine-preventable infectious diseases.
1st Advance: In 1796, Edward Jenner “found that an animal virus (cowpox) could protect against disease caused by a human virus (smallpox)… Jenner’s work ultimately led to the eradication of a disease that is estimated to have killed more than 300 million people in the 20th century”
2nd Advance: In 1885, Louis Pasteur developed an inactivated virus vaccine for rabies. This has led to the development of many other inactivated vaccines, including the influenza vaccine.
3rd Advance: In 1937, Max Theiler attenuated yellow fever virus by means of serial passage in mouse and chicken embryos. This has led to the development of numerous attenuated vaccines to prevent polio (Sabin, 1960s), measles (1963), mumps (1967), rubella (1969), varicella (1995), and rotavirus (2008).
4th Advance: In 1980, Stanford biochemists Richard Mulligan and Paul Berg developed recombinant DNA technology which led to vaccines containing purified surface proteins. This led to the hepatitis B virus (1986), human papillomavirus (2006), and influenza virus (2013) vaccines.
Some of the notable improvements related to vaccines:
In U.S., the incidence of polio dropped from 29,000 cases in 1955 to elimination
In U.S., during the “2019–2020 influenza season, the influenza vaccine prevented an estimated 7.52 million infections, 3.69 million medical visits, 105,000 hospitalizations, and 6300 deaths”
In U.S., the measles vaccine has nearly eliminated a virus that previously caused 2 million to 3 million infections, 50,000 hospitalizations, and 500 deaths every year
In U.S., “since the hepatitis B virus vaccine started being routinely recommended for newborns in the early 1990s, rates of hepatitis B virus infection among children younger than 10 years have fallen from about 18,000 per year to nearly zero”
Globally, “between 2000 and 2018, roughly 23 million measles deaths were prevented by vaccination…Live attenuated rotavirus vaccines are countering a virus that once killed more than 500,000 infants and young children each year”
5th Advance: In 2020 “with the recent authorization of mRNA vaccines, we have entered the fifth era of vaccinology. This class of vaccines doesn’t contain viral proteins; rather, these vaccines use mRNA, DNA, or viral vectors that provide instructions to cells on how to make such proteins. The SARS-CoV-2 pandemic will be an important test of whether these new platforms can fulfill their promise of creating safe, effective, and scalable vaccines more quickly than traditional methods.”
A recent report (JR Zucker et al. NEJM 2020; 382: 1009-17) highlights an outbreak of a vaccine-preventable disease, measles. Measles is much more contagious than the recent coronavirus; this is one reason why a vaccine is so crucial.
In total, there were 649 cases confirmed –most of the cases were in a close-knit community in Brooklyn, NY. 86% of the cases with a known vaccination history occurred in those who were unvaccinated. 49 required hospitalization. The cost to the Department of Health was $8.4 million.
My take: The health consequences and cost of not preventing measles is staggering -though being eclipsed by the coronavirus pandemic. The toll in Europe has been much higher. Worldwide more than 140,000 died from measles in 2018.
704 Measles cases for this year were reported on April 30th. It is likely to climb much higher. More than 40,000 cases were reported in Europe in the first 6 months of 2018.