TE and MRE did not have high correlation with liver biopsy in the detection of high-grade fibrosis
Fibrosis was identified in 90% of liver biopsies with bridging fibrosis in 15 (19%) and cirrhosis in 1 (1%)
AUROC curves of MRE and TE for detection of high-grade fibrosis were 0.817 and 0.750, respectively, and not significantly different.
The authors note that previous adults studies suggest that MRE is more accurate in the identification of liver fibrosis than TE (MRE detected ≥ F1 fibrosis with an AUROC of 0.82, while TE detected fibrosis with an AUROC of 0.67).20
My take: Trying to identify accurate non-invasive testing is crucial to help identify patients most in need of treatment and for limiting costs.
SJ Martinez-Dominguez et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1274–1283, https://doi.org/10.1093/ibd/izad175 Open Acess! Inflammatory Bowel Disease Is an Independent Risk Factor for Metabolic Dysfunction–Associated Steatotic Liver Disease in Lean Individuals
Methods: This was a cross-sectional, case-control study including 300 lean cases with IBD and 80 lean controls without IBD, matched by sex and age (median age ~45 yrs). All participants underwent a liver ultrasound, transient elastography, and laboratory tests. All patients with current or previous use of systemic steroid in the last 2 years were excluded from the analysis
Key Findings:
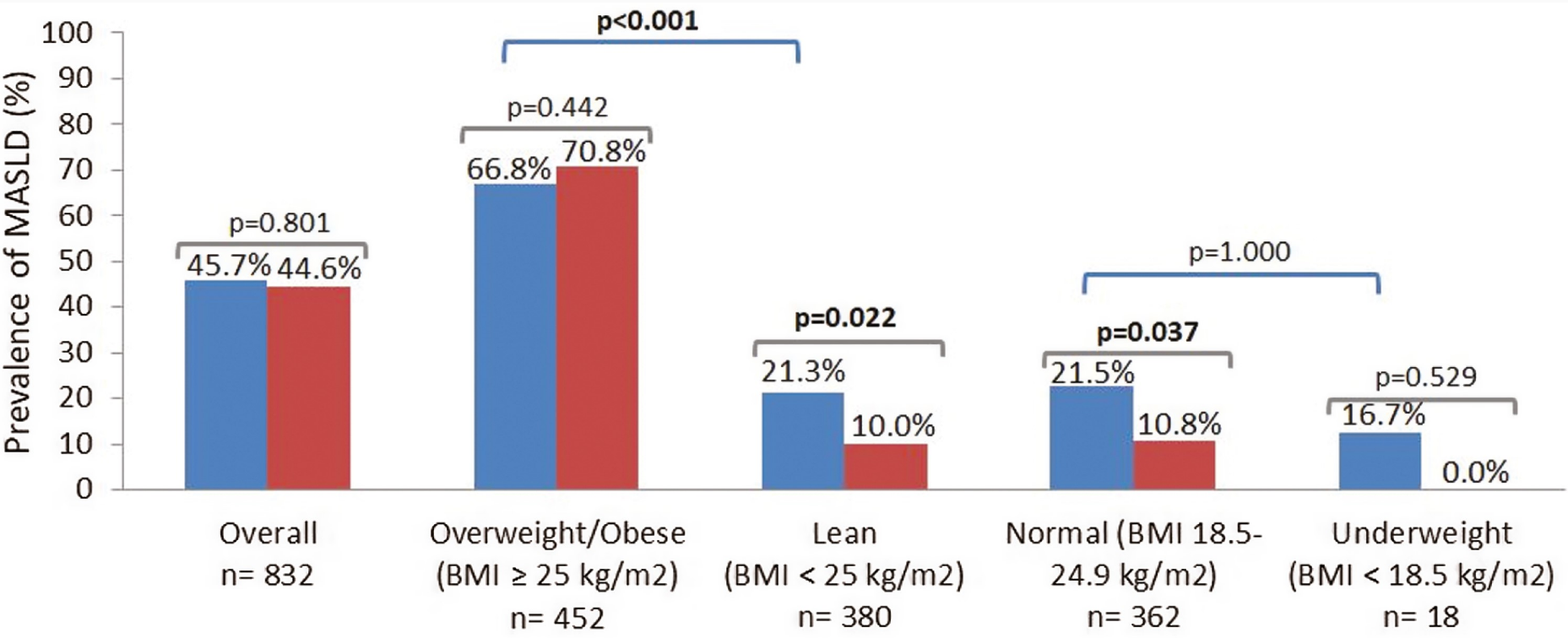
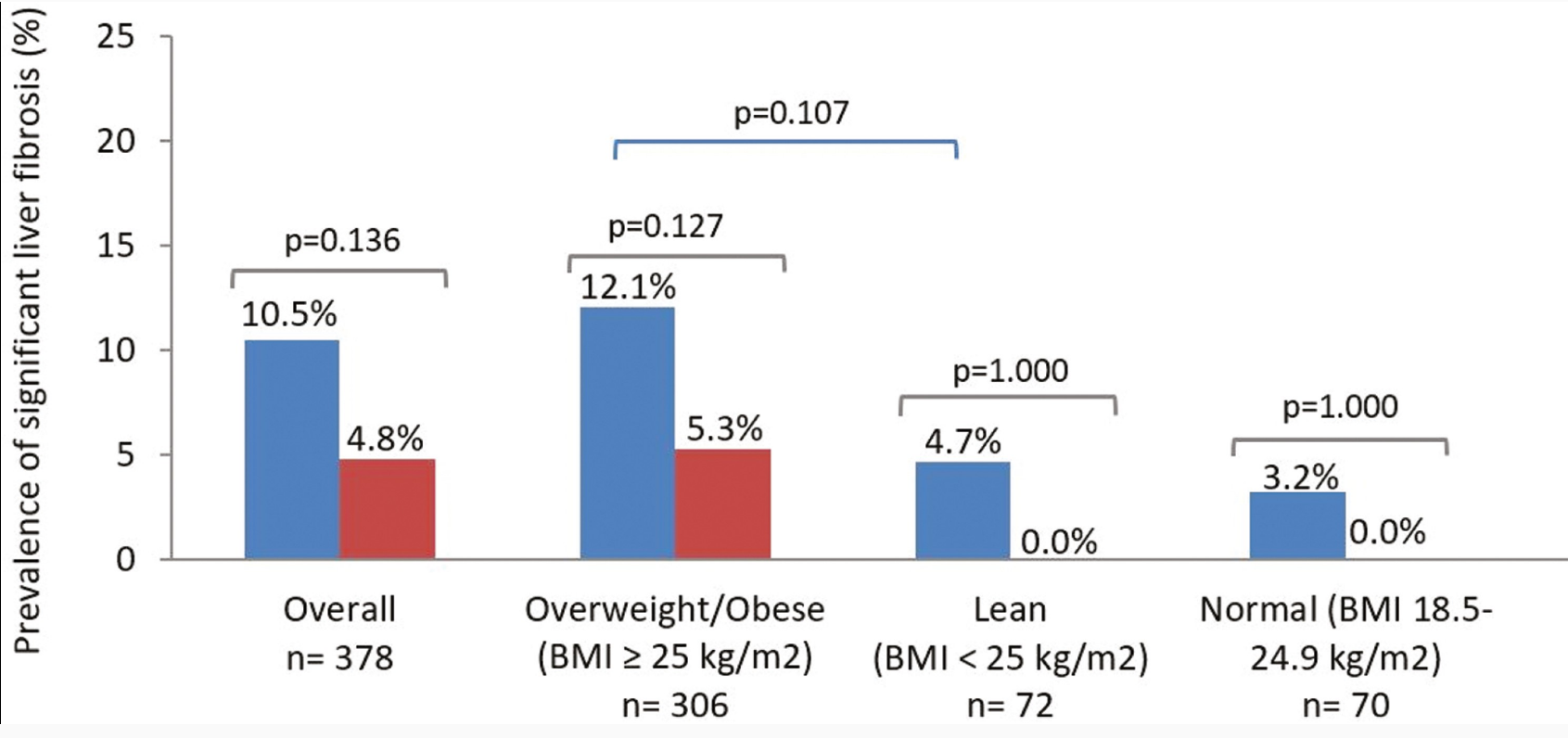
The lean IBD group showed a significantly higher prevalence of MASLD compared with lean non-IBD group (21.3% vs 10%; P = .022), but no differences were observed in the prevalence of significant liver fibrosis (4.7% vs 0.0%; P = 1.000)
No differences were found between the prevalence of MASLD in IBD and non-IBD participants who were overweight/obese (66.8% vs 70.8%; P = .442)
IBD was an independent risk factor for MASLD in lean participants (odds ratio [OR], 2.71) after adjusting for classic metabolic risk factors and prior history of systemic steroid use
Prevalence of metabolic dysfunction–associated steatotic liver disease (MASLD) in cases and controls according to body mass index (BMI) status. Blue bars: cases (inflammatory bowel disease). Red bars: controls (non–inflammatory bowel disease). P values in bold indicate statistical significance (P < .05).
My take: This study suggests that “chronic inflammation could play a role in MASLD development.” Also, this indicates that MASLD could be a reason for elevated LFTs in patients with IBD, even in lean patients.
Methods: Among 1410 adolescents (12–19 years) in NHANES (2017-March, 2020), the controlled attenuation parameter (CAP) of transient elastography (TE) was used to define steatosis and fibrosis (TE ≥ 7.4 kPa). Obesity and alanine aminotransferase (ALT) ≥ 80 U/L were used to identify adolescents qualifying for hepatology referral according to practice guidelines.
Key findings:
At the supplier (EchoSens)-recommended CAP threshold of 240 dB/m, 30.5% of adolescents had steatotic liver disease (SLD) and about 85% of adolescents with NAFLD met criteria for MASLD. At a CAP threshold of 270 dB/m, SLD prevalence was about 16% in adolescents. The other 15% of NAFLD patients do not meet diagnostic criteria MASLD and would receive a diagnosis of cryptogenic SLD or possible MASLD
At higher CAP thresholds, MASLD/NAFLD concordance increased and approached 100%.
Among adolescents with MASLD-fibrosis, only 8.8% had overweight/obese and ALT ≥ 80 U/L. Thus, more than 90% of adolescents in this group would not merit hepatology evaluation based on current guidelines.
My take: This study identifies potential problems with current thresholds for which patients need to be seen by pediatric hepatologists. This will be even more important as effective pharmaceuticals become available.
9698 participants in NHANES during the 2017-2020 cycle completed a transient elastography examination. After excluding patients less than 18 years, these were the key findings:
37.87% had steatotic liver disease
32.45% had MASLD
2.56% had MetALD
1.17% and ALD
Limitations: database study, lack of liver biopsy, reliance on self-reports of alcohol consumption
Methods: 336,866 adults aged ≥30 years were prospectively enrolled in a health screening program between 1997–2013
Key findings:
122,669 (36.4%) had MASLD. Over a mean follow-up of 15 years, 5562 new cases of cirrhosis and 2273 new cases of HCC were diagnosed.
Hazard ratios for HCC were 8.86 for MASLD with HBV or HCV, compared with non-SLD without HBV or HCV
Hazard ratios for HCC were 8.81 for HBV or HCV with non-SLD (SLD), and 1.52 for MASLD without HBV or HCV
My take: MASLD significantly increased cirrhosis and HCC risks; however the risk of HBV or HCV was much greater. The high prevalence rates of MASLD guarantees a huge need for liver disease management for the foreseeable future.
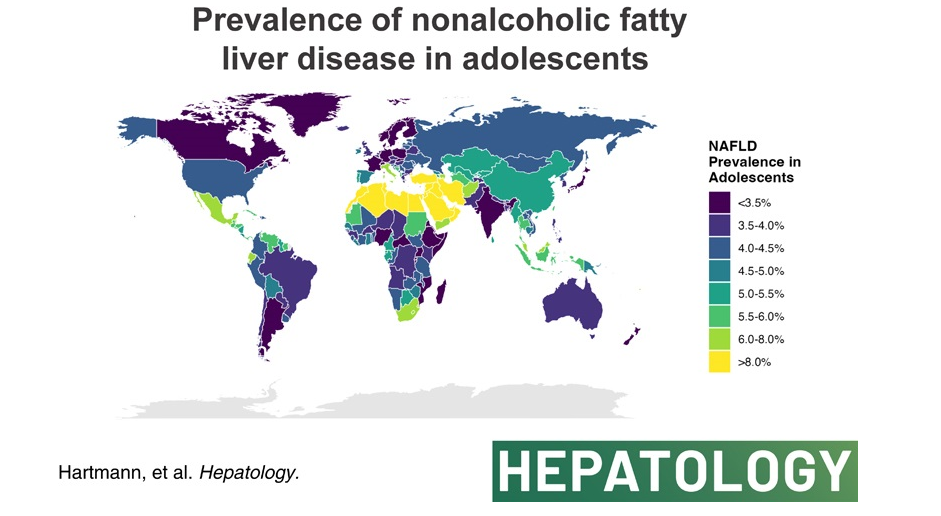
The authors analyzed data from the Global Burden of Disease Study 2019 to compare global, continental, and national prevalence rates of adolescent (15-19 yrs of age) NAFLD.
Key finding:
The global NAFLD prevalence in adolescents increased from 3.73% in 1990 to 4.71% in 2019 (a relative increase of 26.27%). NAFLD is now termed metabolic dysfunction-associated steatotic liver disease (MASLD).
High body mass index and not type 2 diabetes mellitus correlated with NAFLD prevalence in adolescents globally.
In the associated editorial (S Xanthakos, Hepatology78(4):p 1017-1019, October 2023, Rising tide of NAFLD in youth: A warning bell and call to action), some of the key points:
“The Global Burden of Disease (GBD) Study is the most comprehensive and long-standing effort to systematically and scientifically collate data on hundreds of diseases and injuries across the globe, including related clinical outcomes. Beginning in 1990, the GBD Study initially collected data on 106 conditions and 10 risk factors, across 5 age groups.1 Over time, the GBD Study has expanded through serial iterations to involve >9000 international researchers collecting data on 369 diseases and injuries across 204 countries and territories in the most recent 2019 report.1“
” From the GBD Study, we learned that NAFLD is the most rapidly rising cause of chronic liver disease in adolescents and adults,2 and the fastest-growing contributor to cirrhosis, liver cancer, and liver-related deaths globally.”
“The global prevalence of NAFLD in adolescents shows no sign of abating, rather has continued to increase steadily from 3.7% in 1990 to 4.7% in 2019.”
“As with all epidemiological research, the GBD study faces the primary limitation of relying on data sources that employ varying and less accurate measures of NAFLD prevalence (alanine aminotransferase and/or ultrasound primarily). However, the rigorous methodological approach employed by the GBD including frequent assessment of face validity, and the tremendous input of data sources (>80,000 in 2019) nonetheless results in the most comprehensive global data set available.”
My take (borrowed from editorial): Without intervention, “the increase in adolescent NAFLD certainly portends a future increase in NAFLD-related cirrhosis and liver-related deaths in young adults in the coming decades, and a likely escalation in cardiovascular and diabetes-related morbidity.
This article offers best practice advice -here are two of them:
#2: A Fibrosis 4 Index score <1.3 is associated with strong negative predictive value for advanced hepatic fibrosis and may be useful for exclusion of advanced hepatic fibrosis in patients with NAFLD.
#8 Patients with NAFLD and NITs (noninvasive tests) results suggestive of advanced fibrosis (F3) or cirrhosis (F4) should be considered for surveillance of liver complications (eg, hepatocellular carcinoma screening and variceal screening per Baveno criteria). Patients with NAFLD and NITs suggestive of advanced hepatic fibrosis (F3) or (F4), should be monitored with serial liver stiffness measurement; vibration controlled transient elastography; or magnetic resonance elastography, given its correlation with clinically significant portal hypertension and clinical decompensation.
In this study from U.S., patients (n=2523) were divided into three categories based on FIB-4 scores: (A) Fibrosis-4 (FIB-4) <1.3 and/or liver-stiffness measurement (LSM) measured by Fibroscan <8 kp, (B) FIB-4 1.31‒2.6 and/or LSM 8.1-12.5 kp, and (C) FIB-4 >2.6 and/or LSM >12.5 kp. However, those in class A with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3, or class B with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3 were upstaged by one class. The data were reviewed retrospectively from a prospective longitudinal cohort (TARGET-NASH)
Key findings: All adverse outcomes including liver and cardiovascular (see below) were correlated with FIB-4 staging.
Key findings: The prevalence of steatosis, severe steatosis, advanced fibrosis, and cirrhosis was 44.39%, 10.57%, 2.85%, and 0.87%, respectively in Chinese adults
Limitation: This data was derived from a health checkup cohort which could give different results than a random population sampling. Patients at health checkups may be more health conscious and/or be aware of underlying health concerns.
Prevalence of different grades of liver fibrosis in different age groups.
My take: Steatotic liver disease is a huge worldwide problem. The growing prevalence is going to result in extensive health issues.
—————
This year’s pumpkin 910/31/23):
It does not look like I will become a professional pumpkin artist anytime soon!
Ten males [mean 15.1 years, standard deviation (SD) 2.2] with NASH were randomized to once daily treatment with Elafibranor: 80 mg (n = 5) or 120 mg (n = 5). Elafibranor, a dual peroxisome proliferator-activated receptor α/δ agonist, has been proposed as a treatment for nonalcoholic steatohepatitis (NASH, aka Metabolic dysfunction-associated steatohepatitis (MASH)). Key findings:
End of treatment mean ALT was 52 U/L (SD 20) for the 120 mg group, with a relative mean ALT change from baseline of −37.4% (SD 23.8%) at 12 weeks.
Elafibranor was rapidly absorbed and well tolerated.
My take: I think we are on the verge of identifying medications which will be able to improve outcomes for those with steatotic liver disease.
Using NHANES data for 12-19 year olds, the authors examined rates of elevated ALT. Elevated ALT was defined as >22 U/L (females) and >26 U/L (males) Key findings:
Prevalence of elevated ALT in adolescents was 16.5% overall and 39.5% among those with obesity
For White (W), Hispanic (H), and Asian (A) adolescents, prevalence of elevated ALT was 15.8%, 21.8%, and 16.5% overall. In overweight adolescents, 12.8% (W), 17.7% (H), and 27.0% (A), and in those with obesity, 43.0% (W), 43.5% (H), and 43.1% (A) in those with obesity, respectively
Prevalence was much lower in Black adolescents (10.7% overall, 8.4% for overweight, 20.7% for obesity)
Prevalence ofALT at 2X-ULN was 6.6% in adolescents with obesity
Hispanic ethnicity, age, male sex, and higher BMI were independent predictors of elevated ALT
My take: It is hard to get very excited about a mildly elevated ALT value when 1 in 6 adolescents has this as well as ~40% of adolescents with obesity.