


Tag Archives: Ulcerative colitis
Active Colitis More Likely in Children in Clinical Remission Who Have PSC and IBD
A recent study (A Ricciuto et al. Clin Gastroenterol Hepatol 2018; 16: 1098-1105) provides more data regarding the lack of symptom correlation and inflammatory bowel disease (IBD) activity in children with primary sclerosing cholangitis (PSC).
In a prospective study of children with colonic IBD with and without PSC, the authors followed clinical features (eg. PUCAI), fecal calprotectin and endoscopy severity.
Key findings:
- Patients with PSC-IBD (n=37) in clinical remission had higher endoscopic scores and greater odd of active endoscopic disease than IBD-only controls (n=50) (odds ratio 5.9, with CI 1.6-21.5)
- Fecal calprotectin level <93 mcg/g were identified mucosal healing with 100% sensitivity and 92% specificity when compared with UC Endoscopic Index of Severity (UCEIS)
Overall, this study is in agreement with a prior adult study showing higher levels of active disease in those with PSC-IBD compared to those with IBD alone, despite clinical remission (Why does PSC increase the risk of colorectal cancer in UC?).
My take: Particularly in individuals with the combination of IBD-PSC, objective biomarkers (eg. Calprotectin) are needed to identify the accuracy of clinical remission; though, even in patients with IBD without PSC, objective biomarkers are needed as well due to the limitations of clinical symptom indices.
Related blog posts:
- Big Study of PSC in Children
- PSC -Natural History Study (pediatric)
- Primary Sclerosing Cholangitis (PSC) –Natural History Study
- Why does PSC increase the risk of colorectal cancer in UC?
- Remission in Crohn’s Disease

Moraine Lake, Banff
Management of Pediatric Ulcerative Colitis -ESGHAN/ECCO Recommendations
Two complementary articles provide extensive guidance on the management of ulcerative colitis and acute severe colitis:
- D Turner et al. JPGN 2018; 67: 257-91
- D Turner et al. JPGN 2018; 67: 292-310
Between the two articles there are more than 60 practice recommendations, more than 120 practice points, and more than 700 references. As such, these articles are probably better for a journal review meeting rather than a brief blog post.
Figure 1 (2nd article, page 299) provides a handy algorithm for management of acute severe colitis:
- On day 1-2, the algorithm recommends stool studies, starting methylprednisolone, and withholding 5-ASA.
- On day 3, if PUCAI <45, suggests continuing steroid and transitioning to oral therapy when PUCAI <35. On day 3, if PUCAI ≥45, the authors suggest screening for second line therapy, involve surgery (to discuss colectomy if there is nonresponse to medical treatment), and looking for CMV infection (eg. sigmoidoscopy).
- On day 5, if PUCAI >65, recommendation is to start 2nd line Rx (eg. infliximab, tacrolimus, or cyclosporine). If PUCAI 35-65, continue corticosteroids for additional 2-5 days. The authors note that infliximab is preferred 2nd line Rx unless planning to transition to vedolizumab.
- The authors recommend weaning corticosteroids when 2nd line Rx is started
- The authors recommend addition of an immunomodulator for at least 6 months in responders to infliximab in effort to lower the risk of colectomy.
- The authors state “urgent colectomy is recommended following failure of 1 second-line therapy.”
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Related blog posts:
- An overlooked finding in a recent acute severe ulcerative colitis study
- UC SUCCESS
- Infliximab for children with Ulcerative Colitis
- Accelerated Infliximab Dosing in Acute … – gutsandgrowth
- Predictors of colectomy in pediatric UC | gutsandgrowth
- Predicting Remission in Pediatric Ulcerative Colitis …
Is it really necessary to check for Cytomegalovirus in Children with Inflammatory Bowel Disease?
A recent retrospective study (W El-Matary et al. JPGN 2018; 67: 221-24) examined the practice of looking for Cytomegalovirus (CMV) in children with a flareup of their inflammatory bowel disease (IBD) which is currently recommended by expert consensus (JPGN 2018; 67: 292-310 –recommendation #3).
Key findings:
- “Four of 61 patients encounters (6.6%) with UC/IBD-U, two with corticosteroid refractory disease, had positive biopsies for CMV by PCR but negative H&E and IHC. They responded to escalated medical therapy, without needing anti-viral therapy.”
- All children who had colectomy during the study did not have CMV detected in colonic mucosa.
The authors note that the rationale for looking for CMV is derived mainly from adult populations. Since age is a known risk factor for CMV reactivation, the risk of CMV causing refractory IBD in children is less.
My take (borrowed in part from authors): “The low frequency of CMV in our study challenges current guidelines that recommend assessment for CMV in all pediatric patients with acute severe UC refractory to corticosteroids.” This issue would be another that would benefit by collecting the experience of a large cohort (eg. ICN).
Related blog posts:
- Will infliximab worsen flare-ups associated with CMV? (Not in this study)
- CMV in IBD: Tissue Matters | gutsandgrowth
- IBD Updates -January 2017 | gutsandgrowth
- Utility of Antiviral Therapy for Cytomegalovirus in the … – gutsandgrowth
Patient T-shirt
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Serology Titers Associated with Clinical Expression of Ulcerative Colitis in Children
Briefly noted: A recent study (EA Spencer et al.Inflamm Bowel Dis 2018; 24: 1335-42) examined phenotype and serology in 399 children with newly diagnosed ulcerative colitis (PROTECT study).
Key findings:
- 65% had positive serology for pANCA; 62% in those <12 and 66% in those ≥12 years
- 19% had positive serology for anti-CBir1; 32% in those <12 and 14% in those ≥12 years
- High titer (≥ 100)) pANCA positivity was associated with more extensive disease but not with PUCAI values or Mayo endoscopic subscores.
My take: The serology titers for IBD, in my view, have academic interest but do not routinely enhance patient care.
Related blog post:
- Low-Value Care: IBD Serologies for Diagnosis of IBD
- How helpful are serologies in pediatric inflammatory bowel disease?

Amelia Island
VICTORY Consortium Showing Good Results for Vedolizumab
A presentation at the 13th Congress of the European Crohn’s and Colitis Organization (ECCO, Feb 2018) indicated that Vedolizumab had similar effectiveness as anti-TNF agents for both ulcerative colitis and Crohn’s disease. This data has been presented at a recent meeting in our office, some of the GI news magazines, and also ImproveCareNow listserv.
These analyses observed that patients with UC treated with Entyvio compared to TNFα-antagonist therapy had statistically significant higher 12-month cumulative rates of mucosal healing (50% vs 42%, hazard ratio [HR] 1.73, 95% confidence interval [CI] 1.10‑2.73) and clinical remission (54% vs 37%; HR 1.54, 95% CI 1.08‑2.18), and numerically higher steroid-free clinical remission rates (49% vs 38%; HR 1.43, 95% CI 0.79‑2.60). In CD, results reported statistically significant higher 12-month cumulative rates of mucosal healing (50% vs 41%; HR 1.67, 95% CI 1.13‑2.47), and numerically higher rates of clinical remission (38% vs 34%; HR 1.27, 95% CI 0.91‑1.78) and steroid-free clinical remission (26% vs 18%; HR 1.75, 95% CI 0.90‑3.43) compared to TNFα-antagonist therapy. These analyses were conducted by the VICTORY (Vedolizumab Health OuTComes in InflammatORY Bowel Diseases) Consortium.
My take: While the data compare anti-TNFs to vedolizumab in a “real-world setting,” the reported outcomes for anti-TNFs are lower than in other studies. Vedolizumab had the best results in those with colonic disease. Patients with Crohn’s disease with isolated small bowel disease had lower response rates.
Related study: AK Waljee et al Inflamm Bowel Dis 2018; 24: 1185-95. Using phase 3 clinical trial data with 594 subjects, the authors note that the majority of patients who will respond to vedolizumab can be identified by week 6 using a laboratory algorithm based on hemoglobin, albumin, vedolizumab level and CRP. Fformula: Hgb*Albumin*VDZ level/CRP*Weight. A cutoff of 185.96 predicted success with an AuROC of 0.75. Higher hemoglobin, higher albumin, and higher vedolizumab level, and lower CRP are associate with higher response rates.
Related blog posts:
- Summary of latest information on Vedolizumab
- GI Care for Kids Data on Vedolizumab 2017
- Latest on Vedolizumab
- Pediatric Experience with Vedolizumab | gutsandgrowth
- Vedolizumab -another new IBD treatment | gutsandgrowth

Red Top Mountain, Homestead Trail
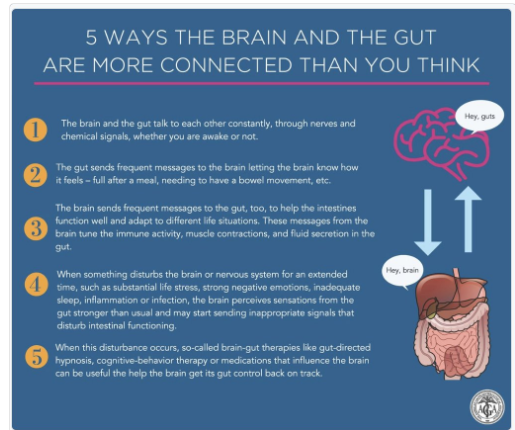
Three Tweets: Colon Cancer Screen at 45 per ACS, Tofacitinib Approved for UC, Brain Gut Connection Infographic


Opiates, Inflammatory Bowel Disease and Mortality
A recent retrospective study (NE Burr et al. Clin Gastroenterol Hepatol 2018; 16: 534-41) with 3517 patient’s with Crohn’s disease (CD) and 5349 with ulcerative colitis (UC) examined the frequency of opioid prescriptions and the relationship to fatal outcomes.
Key findings:
- Compared to 1990-93, the period of 2010-13 saw a sharp rise in the use of opiods in England: 10% compared to 30%.
- Prescription of strong opioids (>3 prescriptions per calendar year) was associated with premature mortality: Hazard ratio 2.18 for CD and 3.3 for UC.
This study is in agreement with other data showing increasing use of opiate prescriptions worldwide for chronic noncancer pain (although there has been a drop in the past year). As with other studies of patients with inflammatory bowel disease, this study shows an association between opioid use and mortality.
My take: Needing an opioid may be a marker for more severe disease. Whether the opioid use directly contributes to mortality remains unclear.

Time Will Tell: Granulomatous Upper GI Inflammation
A recent retrospective study (K Queliza et al. JPGN 2018; 66: 620-23) describes seven patients with granulomatous disease in the upper GI tract who were diagnosed with ulcerative colitis.
This study examined patients at a single center between 2007-2016 with ages ranging from 2 years to 17 years. Median time of followup is not provided. Two patients required colectomy. All patients had non-casseating granulomas identified in either the stomach or duodenum (or both) along with moderate to severe pancolitis. All of the patients had extensive investigations, generally cross-sectional imaging (MRE or CT) or capsule endoscopy
Key point::
- “The final classification of IBD was based on expert opinion from gastroenterologists, radiologists, and pathologists upon thorough review of the medical records.”
My take: This study highlights the confusion of the essentially binary classification of IBD into either Crohn’s disease or ulcerative colitis, when in fact there are hundreds of genetic mutations which give rise to inflammatory bowel disease. Given that granulomas are a hallmark of Crohn’s disease and there are no pathognomic features of ulcerative colitis, only time will tell if these patients have an ulcerative colitis phenotype. I wonder how many centers would take exception to this classification and describe these patients as ‘indeterminate’ colitis/IBDU (IBD unclassified).
Related blog posts:
- ESPGHAN IBD Diagnostic Practice … – gutsandgrowth
- Serology in IBD | gutsandgrowth
- Paris Classification of Pediatric Crohn’s Disease | gutsandgrowth
- How helpful are serologies in IBD

Pediatric Home and Office Biologic Infusions -What is Needed
A recent clinical report (E Barfield et al. JPGN 2018; 66: 680-86) will be influential. This guideline is from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Congratulations to my partner, Chelly Dykes, who is one of the coauthors.
For many years, our office has had an office-based infusion center which has provided infusions in a safe and cost-effective manner. Recently, there have been some situations in which home-based infusions have been proposed either to lower costs and/or for convenience. This report succinctly describes the hurdles that need to be addressed before recommending this treatment pathway. As noted below, patient safety encompasses a great deal more than infusion reactions. Delays in infusions (which can increase risk of loss of response) due to reactions and lapses in communication are additional issues.
Recommendation 1: Home- or office-based infusions should ensure safe administration of the biologic infusion, provide reliable execution of infusion-related orders (eg, laboratories for therapeutic drug monitoring, dose optimization protocols, etc), and be equipped to recognize and respond to potential complications.
- Infusion reactions: ” Infusion reactions associated with infliximab and vedolizumab can range from mild reactions such as fever and chills, dyspnea, pruritus, or urticaria (in approximately 5%–10%), to severe reactions including anaphylaxis, convulsions, and hypotension (<1%)”
- Emergencies: “In the event of an urgent or emergent reaction during home- or office-based infusions, the in-home services agency (IHSA) nurse needs to be able to contact the appropriate ordering medical team member expeditiously by phone or pager to review/clarify specific concerns or needs to have an established clear policy on how to proceed with managing the reaction.”
- Communication: “We identified the lack or inconsistency of on-call coverage by the primary medical team when home- or office-based infusions occur as a significant barrier to safely initiating or continuing home- or office-based infusion programs. Difficulty in reaching a knowledgeable team member is a breach in reliable care and represents serious patient risk.”
- Related work: “In addition to administering the biologic infusion, executing all other infusion-related orders is an important safety consideration. Implementing unique home infusion protocols is linked to treatment efficacy.”
Recommendation 2: Pediatric home- or office-based infusions, particularly for patients 12 years and younger, should be staffed by a pediatric nurse professional with Pediatric Advanced Life Support (PALS) certification and clinical experience with pediatric patients.
Recommendation 3: Evidence-based standard of care for biologic therapy maximizing effectiveness and treatment sustainability should be established before initiating home or office-based infusions.
Recommendation 4: Home- or office-based infusion pathways that decrease opportunity loss for patients and families and deliver high-quality, patient-centered care should be supported and reproduced.
Recommendation 5: Pediatric gastroenterologists should ensure appropriate shared liability with IHSAs to deliver high-quality care in home-based infusions for children by executing pragmatic steps as outlined below:
- “Document discussion with the patient and family about the indication, risks, and adverse event management …
- Refer the patient to an accredited, licensed IHSA based on patient’s insurance coverage. If no accredited, licensed IHSA for the pediatric patient exists, this is grounds for not initiating home- or office-based infusions…
- & 4. Use an infusion protocol… with clear directives on recognition of signs/symptoms of reactions and administration of reaction medications and use of EMS or parent transport to an emergency room.
- Maintain accurate documentation and communication of therapy type, dose, and frequency.
- Provide a reliable communication mechanism for the IHSA to notify provider of changes or infusion-related events
- Regularly reviewing ongoing IHSA performance with regard to delivery of services, accurate laboratory ordering and turnaround time, safety and quality concerns and timely redressal of these issues.
- Switch to another IHSA if the performance reliability is unsatisfactory. …we acknowledge that changing IHSAs may be difficult.”
Recommendation 6: A more equitable division of labor should be established to offset increased administrative burden placed on the pediatric gastroenterologist and medical team to effectively facilitate and maintain home- or office-based infusions, especially when driven by payer-mandated policies.
Recommendation 7: …Among patients receiving home- or office-based infusions, unreliable follow-up care with the provider as scheduled is grounds for discontinuation of home- or office-based biologic therapy.
Recommendation 8: A proper appeals process should be in place to prevent cost transference from payer to patient in payer-mandated decisions for home- or office-based infusions.
Our office practice:
- Emergencies: In our office, there is always one physician dedicated to being available to assess patients who are receiving infusions. This helps insure safety and in addition, helps to make sure that minor medical problems do not needlessly postpone important treatment.
- Documentation: With our office-based infusions, each infusion is documented by the administering nurse. This documentation along with labs are embedded in the medical record (EPIC) to help modify treatment.
- Communication: In our office, prior to each infusion, each patient’s chart is reviewed and specific orders are given. This assures that needed blood tests/imaging, additional treatments (eg. iron infusion), insurance authorizations, necessary followup, and personalized adjustments are made. This type of communication needs to be replicated for home-based infusions; hence, the use of home-based infusions could result in a huge increase in uncompensated work for the treating physician.
My take: In my experience, office-based infusions can be provided safely and in a cost-effective manner. While the convenience of home-based infusion is desirable, before implementing broadly, issues regarding communication, safety protocols, and documentation to allow modifications in therapy need to be proactively addressed. Families may not realize some of the complexities involved in managing infusions and how these issues could affect their child’s long-term response to biologic therapy.
Related blog posts:
- Infliximab infusions without premedication
- My first take: It is hard to save money at a Rolls Royce Dealership
- Orphan Drugs –Very Profitable (Humira is labelled an orphan drug!)
- NY Times: Humira’s Best-Selling Drug Formula: Start at a High Price. Go Higher.
The following image relates to another convenience-related health trend:

Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
