C-H Lo et al. Gastroenterol 2022; 163: 852-861. Open Access! Association of Proton Pump Inhibitor Use With All-Cause and Cause-Specific Mortality
Background: “A major challenge that pharmacoepidemiologic studies often face is the susceptibility to protopathic bias. Protopathic bias occurs when a pharmaceutical agent is prescribed for an early manifestation of a disease and then appears to cause the disease when it is eventually diagnosed…Here, we used a modified lag-time approach to investigate the association between PPI use and all-cause and cause-specific mortality”
Methods: This was a prospective cohort study using data collected from the Nurses’ Health Study (2004–2018) and the Health Professionals Follow-up Study (2004–2018). Study participants: 50,156 women and 21,731 men followed for 831,407 person-years and a median of 13.8 years.
Key findings:
Upon applying lag times of up to 6 years, the mortality associations were attenuated and no longer statistically significant:
- All-cause mortality: HR, 1.04; 95% CI, 0.97–1.11
- Cancer: HR, 1.07; 95% CI, 0.89–1.28
- Cardiovascular diseases: HR, 0.94; 95% CI, 0.81–1.10
- Respiratory diseases: HR, 1.20; 95% CI, 0.95–1.50
- Digestive diseases: HR, 1.38; 95% CI, 0.88–2.18
Longer duration of PPI use did not confer higher risks for all-cause and cause-specific mortality.
My take: This study provides convincing evidence that PPI use does not increase the risk of mortality. Protopathic bias can make PPI use appear to increase the risk of mortality (HR, 1.19 in this study) compared to PPI non-users. It is still a good idea to use these agents for appropriate indications and at appropriate doses.
Related blog posts:
- Austin Bradford Hill, PPIs and IBD
- Why Observational Studies Are Misleading & PPI Association with Kidney Stones
- PPIs: Good News on Safety
- PPIs: Good News on Safety (Part 2) | gutsandgrowth
- More Good News for PPIs: NO Increased Risk of Dementia
- Deconstructing PPI-Associated Risks with Nearly 8 Billion Data Points and More on COVID-19 GI Symptoms (Video) | gutsandgrowth
- PPI Side Effects: “Dissecting the Evidence” | gutsandgrowth

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
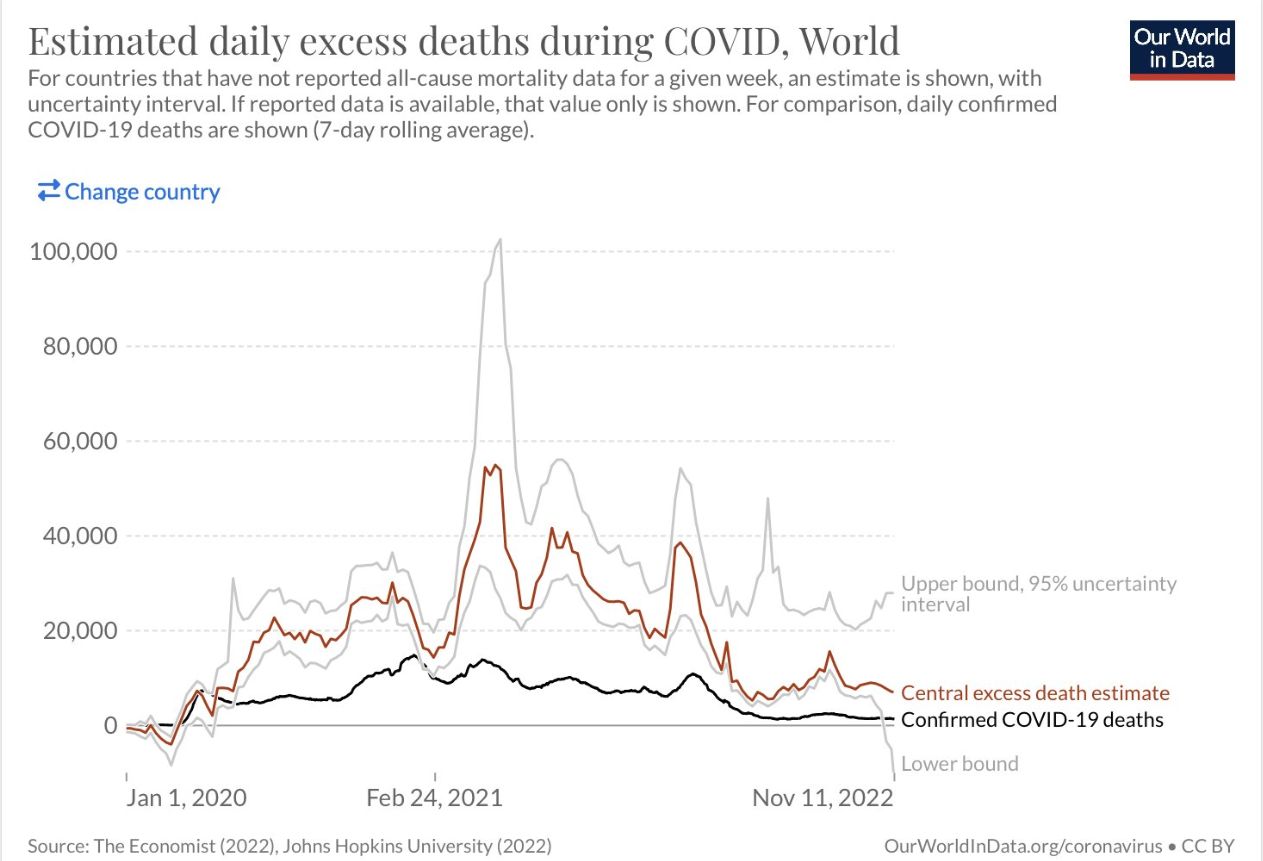
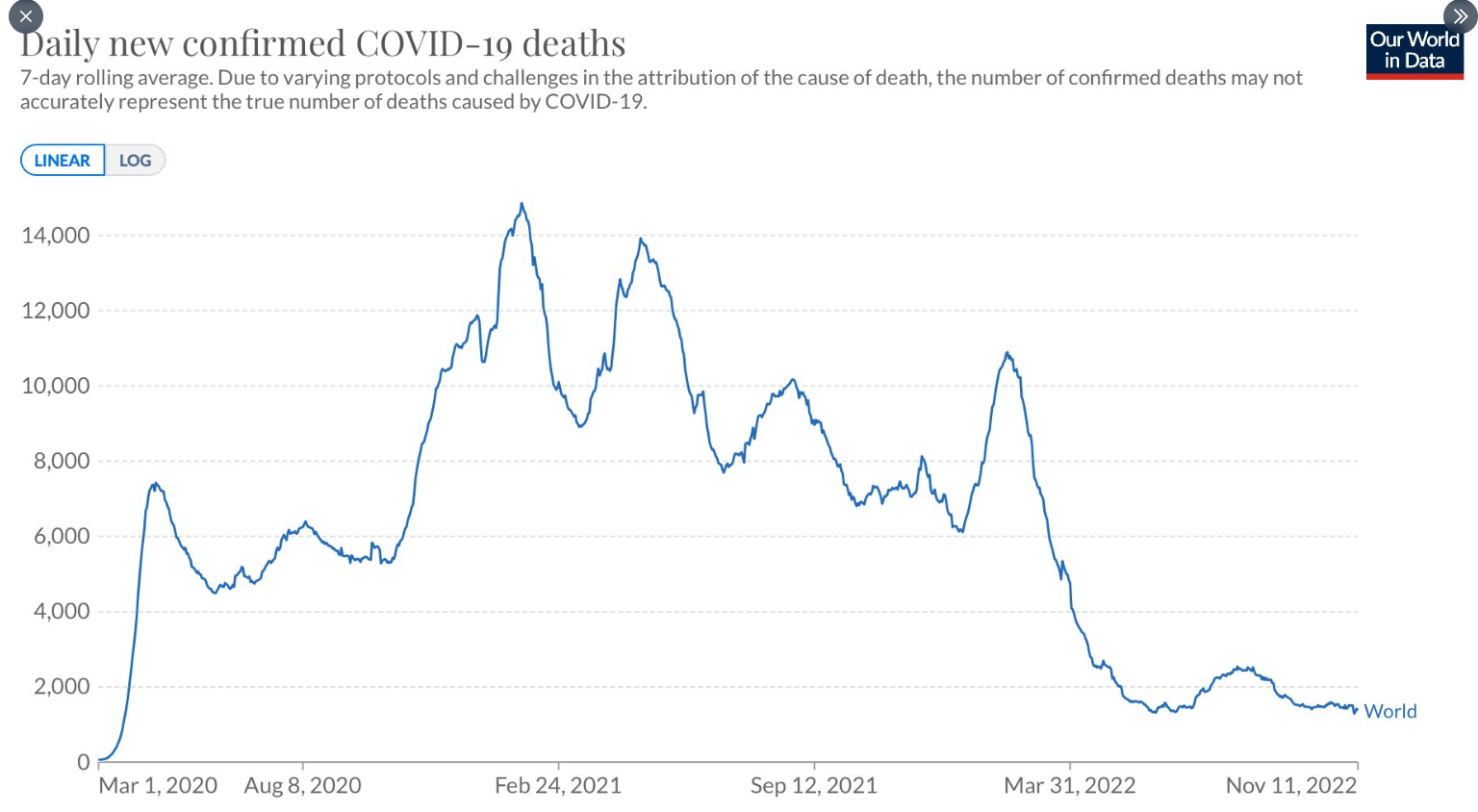
Also, worldwide COVID-19 deaths are at a low point since the beginning of the pandemic (both reported and estimated excess deaths).