This is the last of my blog posts on the topic of biotechnology and foods from Ronald Kleinman’s lecture: Biotechnology, Nutrition, and Agriculture: A Perspective and Implications for Child Health. The posts over the past 4 days describe in detail why the hysteria over genetically modified foods/genetically modified organisms (GMOs) is detrimental. Unfortunately, the lack of understanding has led to widespread adoption of “GMO-free” labeling by food manufacturers which perpetuates the misplaced idea that these foods may not be safe. The slides and lecture will be available at the Nutrition4Kids website.

This mother’s blog: “I don’t feed them organic food and I’m not a bad Mom.” It is a sad commentary that someone needs to write this.

Humans, unlike plants, do not have the enzyme that Roundup (glyposate) targets –so it is safe. By targeting this enzyme, genetic engineering can allow the crop to be herbicide resistant, making it fairly easy to kill off weeds without hurting crop. With biotechnology, we can kill weeds without killing plants. Thus, no till farming is needed. Current herbicides are much safer than prior agents. Roundup (glyphosate) is water-soluble; it is not stored in fat. There is a 30 yr hx/o safe use. There is no data indicating cancer risk in humans or fertility risk.


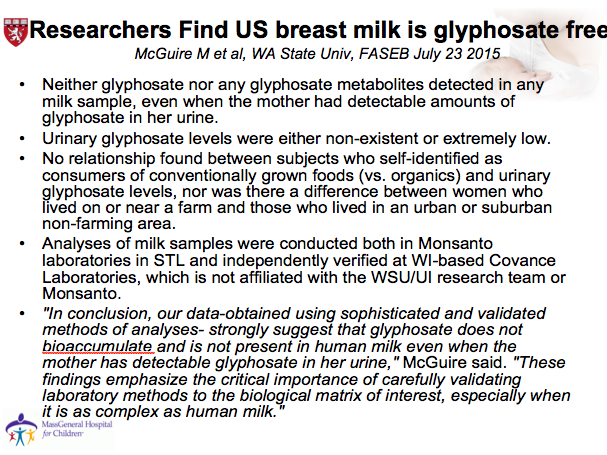
In the past, testing breastmilk for roundup used a flawed methodology. F/u study by McGuire M (sponsored by US govt) showed no Roundup (glyphosate) in breastmilk.
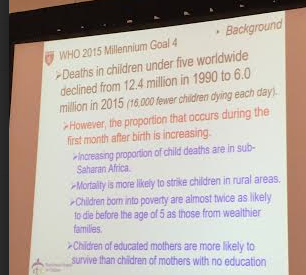
Drought-resistant crops are becoming increasingly important. Meeting global food production will require more ‘crop per drop’ due to increasing population and less lands available for farming. Not just 3rd World –look at California. There are low crop yields in areas without biotech (Subsaharan Africa) and higher mortality.
Key points:
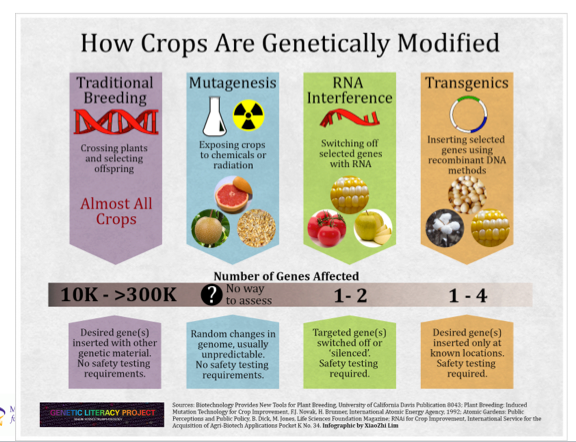
- Genetically Modified Foods/Genetically modified organisms (GMO). These foods are safer and better than foods that are not genetically modified.
- Roundup is not dangerous for humans.
- Attacks on GMOs are part of a larger “War on Science.” As with vaccinations, there is a great deal of misleading and exaggerated information.
- Biotechnology can help solve food crisis, improve the lives of small farmers, and reduce malnutrition. Genetically modified food reduces the needs for chemicals and can improve health.