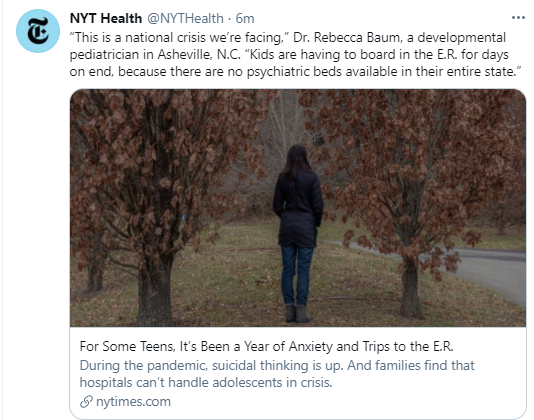
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
Methods: Sixteen callers, aged 17 to 23 years, were briefly trained in empathetic conversational techniques. Each called 6 to 9 participants over 4 weeks daily for the first 5 days, after which clients could choose to drop down to fewer calls but no less than 2 calls a week.
Key finding: A layperson-delivered, empathy-oriented telephone call program reduced loneliness, depression, and anxiety compared with the control group and improved the general mental health of participants within 4 weeks.
Among 9469 included participants, 1516 (16%) were regular users of acid suppressants, and 7953 (84%) were not…propensity score matching (PSM) was applied to match users of acid suppressants and nonusers.
Key findings:
The odds ratio (OR) of testing positive for COVID-19 associated with PPI or H2RA therapy in the PSM cohort was 1.083 (95% confidence interval [CI], 0.892–1.315) and 0.949 (95% CI, 0.650–1.387), respectively.
Omeprazole use alone was significantly related to an increased risk of SARS-CoV-2 infection from the subgroup analysis in patients with upper gastrointestinal diseases (OR, 1.353; 95% CI, 1.011–1.825)
My take: This study provides reassurance that acid blockers are unlikely to contribute to the risk of SARS-CoV-2 or to related complications.
During the past week (as I write this), I came across two articles which focused on the subject of “attention.”
In the first, Toward a Medical “Ecology of Attention” (MJ Kissler et al. NEJM 2021; 384: 299-301), the authors assert that “in the clinical environment, the most important –and most limited–resource is attention.” They note that distraction contributes “to lapses in judgement, insensitivity to changing clinical conditions, and medication errors.” The article delves into modifications that can improve attention in clinical settings:
Prioritizing communications using triaging and batching
Designing physical spaces to improve concentration
Optimizing electronic health record to minimize attention spent maintaining the record outside vital patient care activities
“Most of this came to him in the mid-1980s, when Mr. Goldhaber, a former theoretical physicist, had a revelation. He was obsessed at the time with what he felt was an information glut — that there was simply more access to news, opinion and forms of entertainment than one could handle. His epiphany was this: One of the most finite resources in the world is human attention. To describe its scarcity, he latched onto what was then an obscure term, coined by a psychologist, Herbert A. Simon: “the attention economy“…
“Rational discussion of what people stand to gain or lose from policies will be drowned out by the loudest and most ridiculous.”
His biggest worry, though, is that we still mostly fail to acknowledge that we live in a roaring attention economy. In other words, we tend to ignore his favorite maxim, from the writer Howard Rheingold: “Attention is a limited resource, so pay attention to where you pay attention.”
Perhaps, just by acknowledging its presence [the attention economy], we can begin to direct it toward people, ideas and causes that are worthy of our precious resource.”
My take: I frequently relate a quote from Jim Gaffigan. He stated that his wife is great at multi-tasking but that he is trying just to task. I try to focus on what’s in front of me.
Steven Liu for Epic functionality (in the ~first 20 minutes)
John Pohl for Cerner functionality (in the ~second 20 minutes)
Jennifer Lee discussed patient portal, improving provider-patient communication, & protecting adolescent confidentiality-21st Century Cures Act
Jeannie Huang discussed the role of EHRs in value-based health care and clinical data collection.
Since our group mainly uses Epic, I will summarize some of the tips from Steven Liu, who also is our group’s Epic Physician Champion. Anyone who listened to the webinar will realize how there are so many tricks available. Some of the material from the talk is at the bottom in the form of screenshots; however, much of the information in the webinar is proprietary to EPIC and cannot be shared without permission.
Here are some of the key points:
Customize your templates for progress notes/H&Ps/other notes.
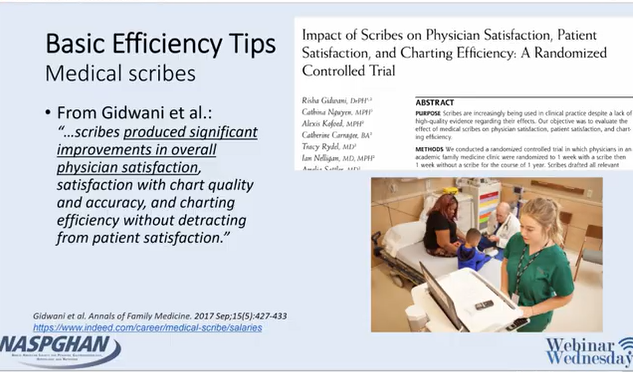
Scribes may relieve frustration and be a good investment
Use Smartphrases and Smartlinks
Smartphrases can be taken (or customized) from other users -can browse your superusers phrases by looking under Smartphrase manager
Smartforms can be very useful (eg. ImproveCareNow)
Using Dictionary, users can change autocorrect: example: if you type EoE, you could have it modified to Eosinophilic Esophagitis
Utilize customized filters (wrench icon) under the chart review tabs
Take advantage of the Chart Search function
can search “PPI” or “calprotectin” and this will identify if patient has used a PPI or had a calprotectin
can access this feature quickly with CTRL-spacebar
Shortcuts can save time -examples ALT-A and ALT-S
Take the time to build customized order panels, like “Celiac Annual Labs”
Health Maintenance Checklists can be incorporated but users may need their system to activate this feature
There is an Inbox Reminder function (to remind patient to get an appointment or test) or you can send a inbox message to yourself with a future date
For more sophisticated users: generating reports with Workbench
Epic has free classes (User Web -see slide below) available to help practitioners become more proficient (eg. Power User Course)
My take: Steven has helped everyone in our practice & listening to his talk makes me realize that I need to learn a good bit more and take some of his stuff. This EHR webinar provides a lot of tips to help good EHR users become better users. For those interested in research, understanding EHRs will be crucial going forward.
“Due to their mechanism of action, both mRNA COVID-19 vaccines are recommended for all patients with CLD (compensated or decompensated) and immunosuppressed SOT recipients.”
“The AASLD recommends that providers advocate for prioritizing patients with compensated or decompensated cirrhosis or liver cancer, patients receiving immunosuppression such as SOT recipients, and living liver donors for COVID-19 vaccination based upon local health policies, protocols, and vaccine availability.”