

Category Archives: General Health
Do Gun Law Restrictions Work?
Those opposed to gun safety provisions (a.k.a. gun control legislation) argue that laws will not prevent criminals from obtaining firearms illegally. A recent commentary in NY Times provides some data that shows that states with more gun safety provisions have lower levels of gun-related deaths (especially suicides).
NY Times: A Gun Killed My Son. So Why Do I Want to Own One?
Related blog posts:
- Firearm Mortality –Tragic Inertia
- No Exaggeration: Too Many Children are Dying in the US
- Another Day in the US: School Deaths Related to Firearms
- Is There an Unlocked Gun Where Your Child Plays?
- Firearm Mortality in U.S.
- Is It OK for Pediatricians to try to Prevent Firearm Injuries? Focus on Child Safety –Not on Gun Safety
- Physician narrative on gun control | gutsandgrowth
- NY Times: End the Gun Epidemic in America | gutsandgrowth
- A Call to Arms for Health Care Professionals
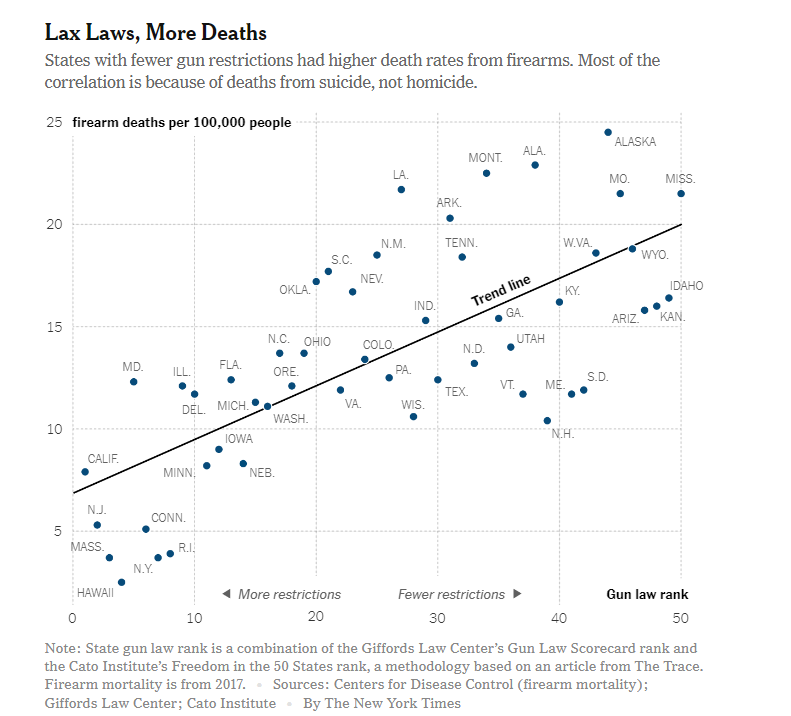
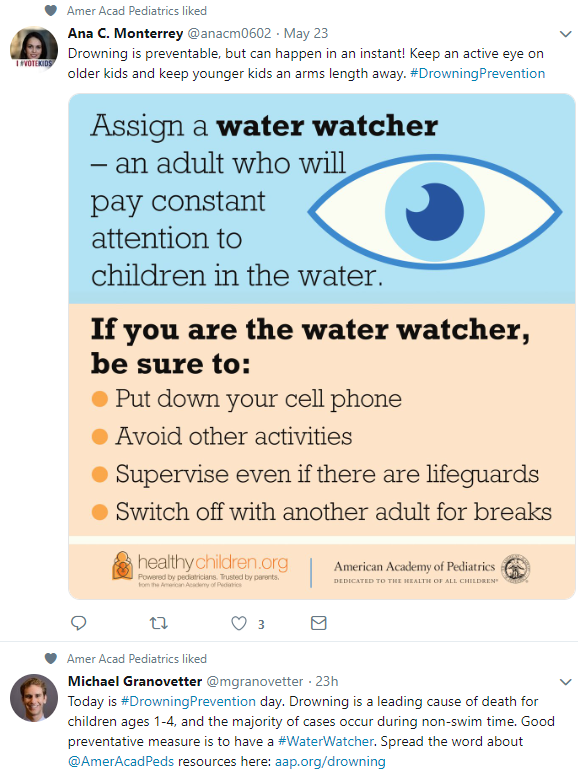
Image Only: Water Safety
Image
NY Times: “Millions Take Gabapentin for Pain. But There’s Scant Evidence It Works.”
NY Times: “Millions Take Gabapentin for Pain. But There’s Scant Evidence It Works.”
Thanks to Stan Cohen for pointing out this reference.
An excerpt:
The drug was initially approved 25 years ago to treat seizure disorders, but it is now commonly prescribed off-label to treat all kinds of pain, acute and chronic…
Two doctors recently reviewed published evidence for the benefits and risks of off-label use of gabapentin (originally sold under the trade name Neurontin) and its brand-name cousin Lyrica (pregabalin) for treating all kinds of pain…
Gabapentin and Lyrica, both sold by Pfizer, have been approved by the Food and Drug Administration to treat only four debilitating pain problems: postherpetic neuralgia, diabetic neuropathy, fibromyalgia and spinal cord injury. Even for these approved uses, the evidence for relief offered by the drugs is hardly dramatic…
In many well-controlled studies they found there was less than a one-point difference on the 10-point pain scale between patients taking the drug versus a placebo, a difference often clinically meaningless….
the number of people taking gabapentinoids more than tripled from 2002 to 2015…
Related blog post: Brave New World: Psychotropic Manipulation and Pediatric Functional GI Disorders
Near Cathedral of Barcelona
Self-Service Health Care??
A provocative commentary (DA Asch et al. NEJM 2019; 380: 1891-3) notes that the current approach to improving health care costs needs to be reconsidered.
“The physician-patient encounter is health care’s choke point.” Instead of pushing for more primary care visits, the authors recommend greater use of automation. Examples in other industries have included:
- TurboTax -helped reduce need for tax preparer’s
- Automated tellers at banks -reduce costs at banks
- Self-checkout at grocery stores -reduce costs at grocery stores
- Websites to directly arrange travel rather than travel agents
Much of medical care can be algorithmic, including hypertension (which affects one-third of U.S. adults), hyperlipidemia, anticoagulation, diabetes, and “might be far more efficiently managed by a bot.”
“An efficient industry wouldn’t lead with primary care, but would reserve it for cases for which lower levels of support haven’t been enough.”
The authors note that efforts to promote this will require removal of state-based regulation. “There is not legitimate interest that benefits from making it hard for a patient in Kansas to get automated care with third-level support from a physician in Ohio.”
My take: The authors are right in their assertion: “Transformative change in any industry requires breakthroughs in productivity.” Some of these changes are likely to be implemented given the cost escalations facing health care.

Magic Fountain, Barcelona
“Physician-Patient Relationship is Not Necessary to Sue Docs for Malpractice”
A recent ruling from the Minnesota Supreme Court:
Thanks to Jeffrey Blumenthal for pointing out this reference. An excerpt:
The Minnesota Supreme Court issued a ruling on April 17 in the case of Warren v. Dinter holding that the existence of a physician-patient relationship is not a prerequisite for a medical malpractice action. Rather, a person may sue a physician for malpractice – even if that person was not a patient of the physician – if the harm suffered by the person was a “reasonably foreseeable consequence” of the physician’s actions….
The Warren v. Dinter case arises out of the care provided to a woman (Susan Warren), who complained of abdominal pain, fever, chills, and other symptoms to a nurse practitioner at Essentia Health Clinic in Hibbing. After testing showed that Warren had an elevated white blood cell count, the nurse practitioner suspected infection and sought hospitalization for her at Fairview Range Medical Center. The nurse practitioner’s call was randomly assigned to a hospitalist at Fairview to discuss admission.
After a brief conversation, during which the physician was unable to view the patient’s medical record, …the physician did not recommend hospitalization during the conversation and the nurse practitioner did not seek hospitalization for the patient following the conversation. The patient subsequently died from sepsis caused by an untreated staph infection. Warren’s family sued both the nurse practitioner and the physician for medical malpractice…
Before its ruling April 17, Minnesota law has generally required the existence of a physician-patient relationship to sustain a malpractice action against a physician. The Court’s decision to rely on a broader legal theory of “foreseeability” represents a troubling change that puts Minnesota in the minority of states that do not require the existence of a physician-patient relationship for a malpractice action.
My take: While “foreseeability” was used as a determinant in this case, observers may foresee that the court’s ruling could erode informal advice (aka. curbside consults) that generally improves patient outcomes. If physicians’ liability is significant, many may choose to not offer advice on patients that they have not fully evaluated.

Barcelona Esplanade/Adjacent to beach
Annual Costs: Generics vs. Brand-Name Medications
MDEdge: Cost gap widens between brand-name, generic drugs
An excerpt:
- The average cost of a brand-name drug was 18.6 times higher than its generic equivalent in 2017, and the size of that gap has more than tripled since 2013, according to a report from the AARP Public Policy Institute…
- In 2017, the average retail cost of 260 generic drugs widely used by older adults for chronic conditions was $365 for a year of therapy, compared with $6,798 for brand-name drugs. In 2013, that same year of therapy with an average brand-name drug ($4,308) was only 5.7 times more expensive than the generic ($751)…
- “Generics account for nearly 9 out of every 10 prescriptions filled in the U.S. but represent less than a quarter of the country’s drug spending,” Debra Whitman, executive vice president and chief public policy officer at AARP
My take (borrowed in part from Debra Whitman):
- “These results highlight the importance of eliminating anticompetitive behavior by brand-name drug companies so that we get more lower-priced generic drugs on the market”
- This data shows the alarming increase in cost of brand-name medications.
Related blog posts:
- Another Shady Pharmaceutical Business Practice: Citizen’s Pathway to Delay Competition | gutsandgrowth
- “This Is A Stick Up — Your Money or Your Life” | gutsandgrowth
- Exorbitant Medicine Costs -Even with Long-established Generics
- Turning Liquid into Gold: A Pharmaceutical Rumpelstiltskin Story | gutsandgrowth
- Orphan Drugs –Very Profitable | gutsandgrowth
- Public Shaming is Not an Effective Drug Pricing Policy | gutsandgrowth
- Drug Waste Costing Billions. Who benefits? Pharmaceutical Companies | gutsandgrowth
- Tackling High Drug Costs -Lessons from Australia and Brazil
- 5000% Increase for Well-Established Drug
- Drug Waste Costing Billions. Who benefits? Pharmaceutical Companies
- How to Undermine Value Care: Lessons from Pharmaceuticals
- The Solution to Drug Prices” | gutsandgrowth
- Cornering the Generic Markup | gutsandgrowth
- Upside Down Incentives in Pharmaceutical Development -Profit …
- “New Math on Drug Cost-Effectiveness”

AAP Recommends Isotonic Maintenance IV Fluids
Full text: Feld LG et al. Pediatrics 2018; 142: pii:e20183083: Clinical Practice Guideline: Maintenance Intravenous Fluids in Children
Key Recommendation:
The American Academy of Pediatrics recommends that patients 28 days to 18 years of age requiring maintenance IVFs should receive isotonic solutions with appropriate potassium chloride and dextrose because they significantly decrease the risk of developing hyponatremia (evidence quality: A; recommendation strength: strong)
Isotonic and Hypotonic Fluids:
- Examples of isotonic/near isotonic fluids listed in Table 1 include D5 Normal Saline (0.9%), D5 Lactated Ringer’s which have osmolarities of 308 mOsm/L (same as human plasma) and 273 mOsm/L respectively.
- Examples of hypotonic fluids include D5 1/2 Normal Saline (0.45%) and D5 1/4 Normal Saline (0.2%) which have osmolarities of 154 mOsm/L and 78 mOsm/L respectively
“The administration of hypotonic IVFs has been the standard in pediatrics. Concerns have been raised that this approach results in a high incidence of hyponatremia and that isotonic IVFs could prevent the development of hyponatremia… in most patients from 28 days to 18 years of age who require maintenance IVFs. This guideline applies to children in surgical (postoperative) and medical acute-care settings, including critical care and the general inpatient ward.”
Excluded from these recommendations: “Patients with neurosurgical disorders, congenital or acquired cardiac disease, hepatic disease, cancer, renal dysfunction, diabetes insipidus, voluminous watery diarrhea, or severe burns; neonates who are younger than 28 days old or in the NICU; and adolescents older than 18 years old”
My take: It remains commonplace for patients to receive hypotonic fluids which place them at unnecessary risk for iatrogenic hyponatremia.
Related blog posts:
- Why D51/2 NS was the Right Choice for IVFs in the 1950s!
- What’s critical to you | gutsandgrowth
- We Still Have More to Learn” | gutsandgrowth
- Has Your Hospital Restricted Quarter-Normal Saline …

Magic Fountain, Barcelona
What’s the Chance You Will Be Taking an Antibiotic in the Next Year?
A recent letter (SW Olesen et al. NEJM 2019; 380: 1872-3) showed the frequency of filling antibiotic prescriptions in the U.S. from 2011-2014 using the Truven Health MarketScan Research Databases (62 million enrollees).
Key findings:
“The probability of filling an antibiotic prescription at an outpatient pharmacy was 33% … over 1 year, 47% …over 2 years, 55% …over 3 years, and 62%…over 4 years.”
My take: One-third of the population is filling an antibiotic prescription each year. That is way too much –antibiotic stewardship program personnel should have a lot of job security.

White Coat Contamination
A recent NYT story: Why Your Doctor’s White Coat Can Be a Threat to Your Health
An excerpt:
A recent study of patients at 10 academic hospitals in the United States found that just over half care about what their doctors wear, most of them preferring the traditional white coat…
What many might not realize, though, is that health care workers’ attire — including that seemingly “clean” white coat that many prefer — can harbor dangerous bacteria and pathogens.
A systematic review of studies found that white coats are frequently contaminated with strains of harmful and sometimes drug-resistant bacteria associated with hospital-acquired infections. As many as 16 percent of white coats tested positive for MRSA, and up to 42 percent for the bacterial class Gram-negative rods…
The review also found that stethoscopes, phones and tablets can be contaminated with harmful bacteria. One study of orthopedic surgeons showed a 45 percent match between the species of bacteria found on their ties and in the wounds of patients they had treated. Nurses’ uniforms have also been found to be contaminated.
My take: Your white coat should probably be washed as often as you wash your underwear (if you decide to wear it).

