A total of 46 studies fulfilled the eligibility criteria, comprising approximately 8 million participants from 21 countries.
Key findings:
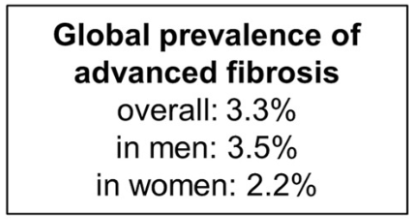
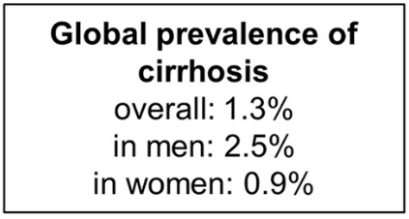
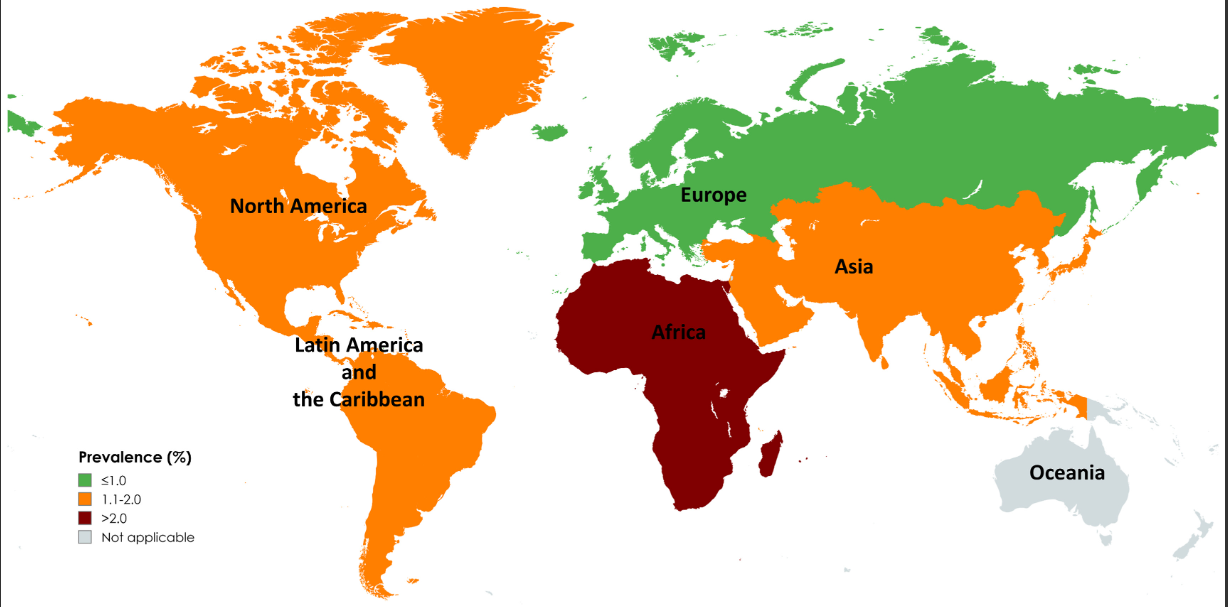
The pooled prevalence rates of advanced liver fibrosis and cirrhosis in the general population were 3.3% (95% CI, 2.4%–4.2%) and 1.3% (95% CI, 0.9%–1.7%) worldwide, respectively
Risk factors for cirrhosis were viral hepatitis, diabetes, excessive alcohol intake, obesity, and male sex
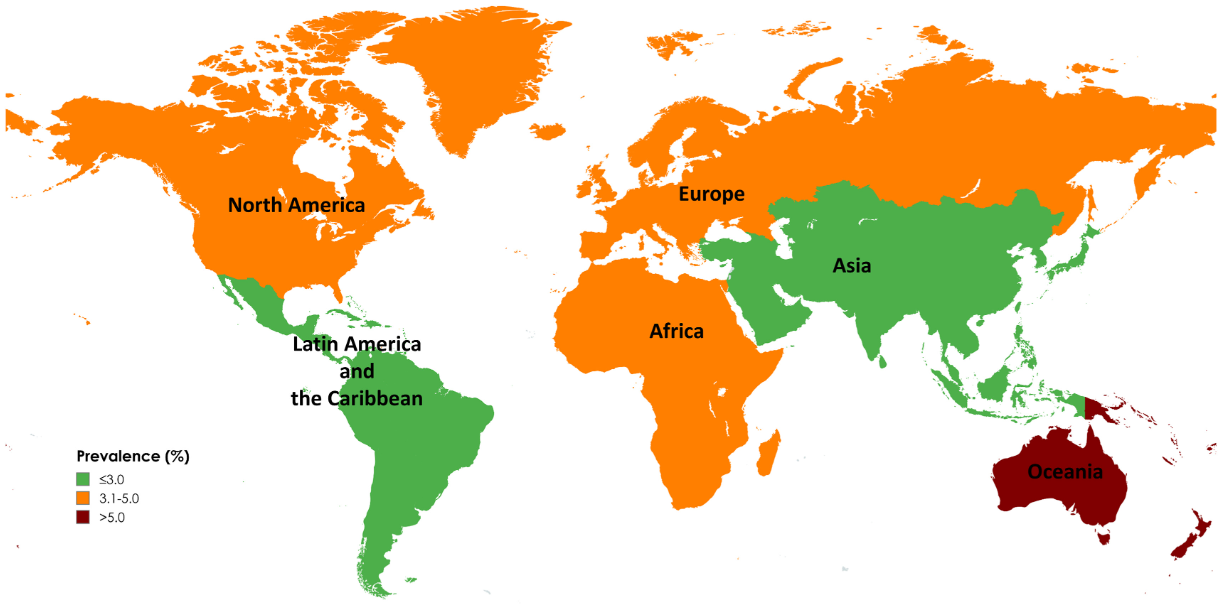
Limitations: 1. All included studies used noninvasive tests to diagnose advanced fibrosis and cirrhosis, which might overestimate prevalence in general populations. The diagnostic performance of these tests is influenced by baseline prevalence, leading to a higher rate of false positives in low-prevalence populations 2. Significant differences in prevalence by geographic region and time period. However, these differences could be influenced by variations in health care infrastructure, access to health care, and disease awareness, which may only partially reflect the true prevalence of advanced liver fibrosis and cirrhosis. In addition, the data is influenced by the number of studies (eg. Oceania had only 1 individual study).
Map of Global Prevalence of Advanced FibrossiMap of Global Prevalence of Cirrhosis
My take: This study provides estimates of the high and increasing prevalence of advanced liver fibrosis and cirrhosis. This data is essential in determining if we are making progress and how to mitigate the disorders leading to advanced liver disease.
From the commentary: “In 2019, the EAT-Lancet Commission on Food, Plant, and Health proposed a planetary health diet, known as the EAT-Lancet reference diet, that promotes human health and sustainable food production globally…and recommends fruits, vegetables, whole grains, plant-based proteins (eg. legumes, nuts) and unsaturated plant oils, with limited or moderate amounts of animal-based proteins such as meat and dairy….[it] has been associated with multiple health benefits, including reducing the risks of type 2 diabetes, cardiovascular disease, certain cancers, and all-cause mortality.”
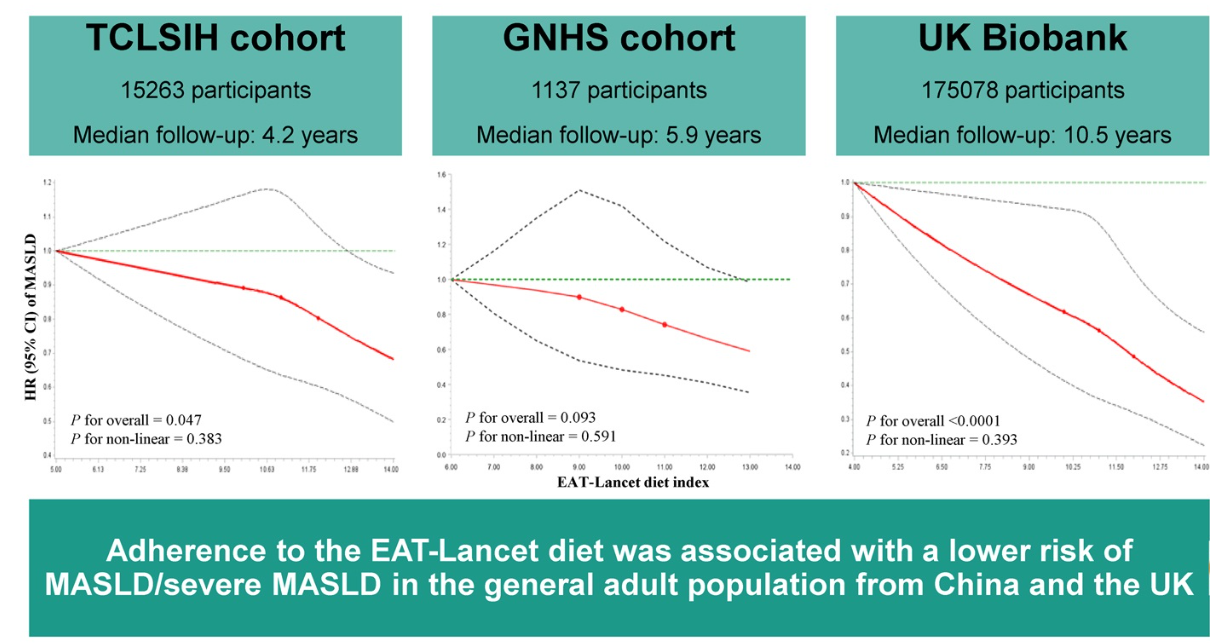
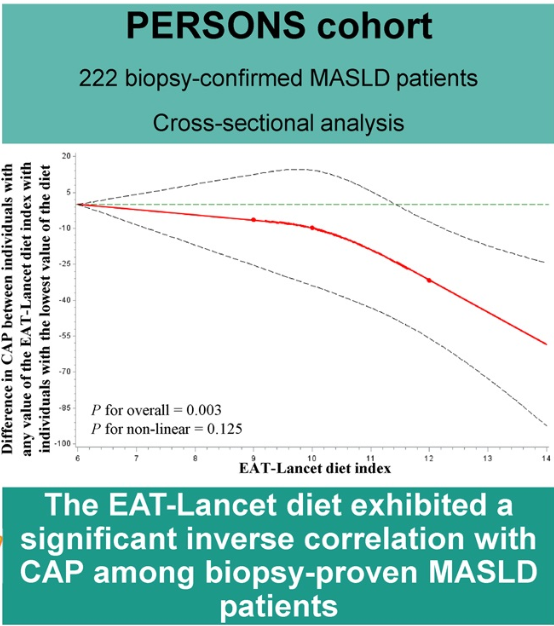
Methods: This prospective multicohort study comprised more than 191,000 adults from several cohorts. In addition, 228 Chinese adults from the Prospective Epidemic Research Specifically of Non-alcoholic Steatohepatitis (PERSONS) with biopsy-proven MASLD were included.
Key findings:
Participants in the highest tertiles of the EAT-Lancet diet index had a lower risk of MASLD compared with those in the lowest tertiles with HR ranging in different cohorts from 0.73 to 0.87
Liver-controlled attenuation parameter decreased with increasing the diet index in individuals with biopsy-proven MASLD (β = −5.895
My take (borrowed from the authors): Adherence to the EAT-Lancet reference diet was inversely associated with the risk of MASLD as well as its severity.
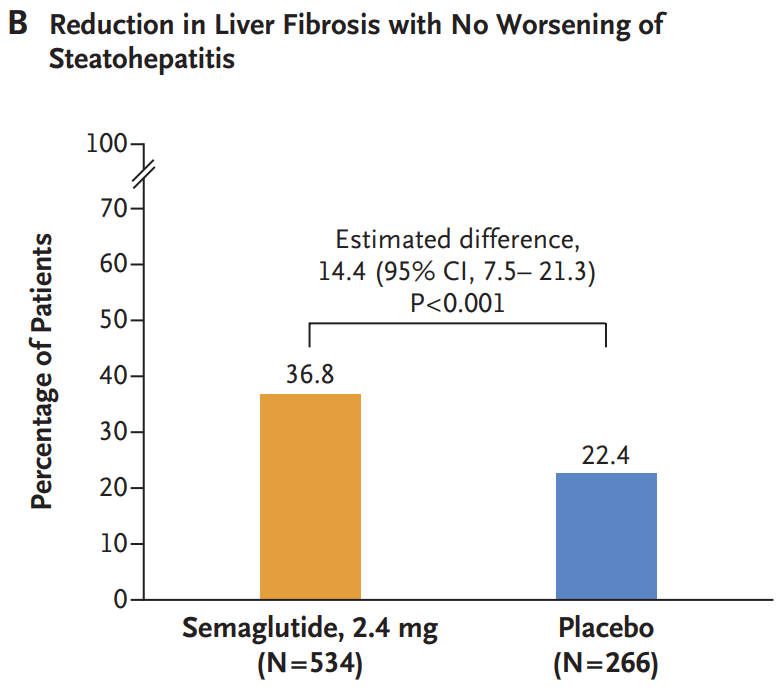
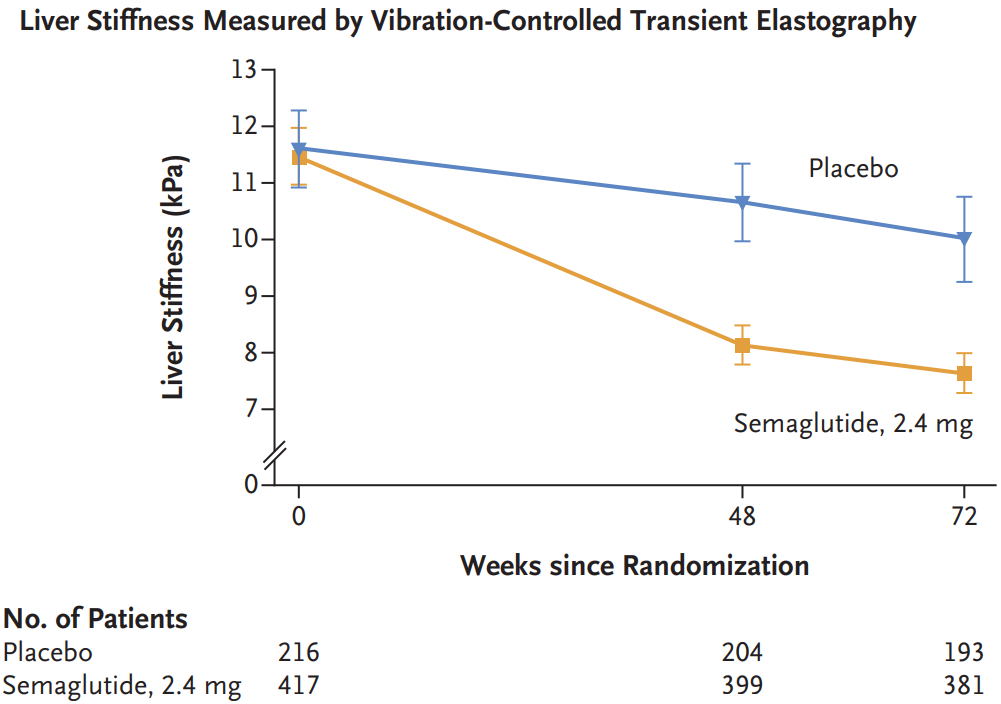
Methods: In this phase 3, multicenter, randomized, double-blind, placebo-controlled trial, the authors assigned 1197 patients with biopsy-defined MASH and fibrosis stage 2 or 3 in a 2:1 ratio to receive once-weekly subcutaneous semaglutide at a dose of 2.4 mg or placebo for 240 weeks
Key findings:
Resolution of steatohepatitis without worsening of fibrosis occurred in 62.9% of the 534 patients in the semaglutide group and in 34.3% of the 266 patients in the placebo group (P<0.001)
A reduction in liver fibrosis without worsening of steatohepatitis was reported in 36.8% of the patients in the semaglutide group and in 22.4% of those in the placebo group (P<0.001).
The mean change in body weight was −10.5% with semaglutide and −2.0% with placebo (P<0.001)
Gastrointestinal adverse events were more common in the semaglutide group. The incidence of acute pancreatitis was similar in the two groups: Nausea 290/800 (36.2%) vs. 52/395 (13.2%), Diarrhea 215/800 (26.9%) vs. 48/395 (12.2%), Constipation 178/800 (22.2%) vs. 33/395 (8.4%) and Vomiting 149/800 (18.6%) vs. 22/395 (5.6%)
Semaglutide improved multiple cardiometabolic features, including glycemic control and insulin resistance. “These findings are important because metabolic dysfunction is an upstream event driving hepatic lipotoxicity and, subsequently, steatohepatitis and fibrogenesis. Thus, semaglutide treatment addressed the primary pathogenic driver of MASH”
Side effects leading to people dropping out of the trial were 2.6% for the semaglutide group and 3.3% for the placebo group
Discussion notes that “although semaglutide can be safely used in patients with cirrhosis, its efficacy in this population has not been established.”
My take: Semaglutide appears to be effective in patients with MASH.with stage 2 or 3 fibrosis.
This guideline reviews and recommends blood-based tests as a tool to help determine the likelihood/severity of liver fibrosis in the presence of chronic liver disease. Most of the guideline focuses on adult liver disease. For pediatrics, the guideline makes the following recommendation:
In the pediatric patients with chronic liver disease, AASLD suggests the use of simple, cost-effective, and readily available blood-based NILDA [Non-invasive Liver Disease Assessment], such as APRI or FIB-4, for the detection of advanced fibrosis (F3-4) (ungraded statement).
Technical Remarks:
Some blood-based NILDA in children have good accuracy in detecting advanced fibrosis but have difficulty discriminating earlier stages of fibrosis.
FIB-4 does not perform as well in children as it does in adults, particularly very young children, due to the inclusion of age in the index.
Rapid growth in children and attendant fluctuations in alkaline phosphatase can confound interpretation of blood or collagen-based NILDA tests in pediatric liver disease.
There are insufficient biopsy validated data to recommend biomarkers for evaluating fibrosis in pediatric NASH and α1AT at this time.
In the pediatric population with CLD, there is growing but insufficient evidence to recommend blood-based NILDA as endpoints to monitor changes in fibrosis over time.
Despite the guidance recommendation, reading the text makes one leery about relying on these tests:
For example with biliary atresia: “The utility of APRI to assess or predict liver fibrosis in BA is mixed in the current literature.”
“In conclusion, blood-based NILDA tests in children vary widely in their accuracy, even in detecting F3-4 fibrosis, and have difficulty discriminating earlier stages of fibrosis. These tests also have different disease-specific thresholds that correlate with histopathologic fibrosis and differ from adults. APRI and FIB-4 have been the most studied NILDA tests in children, but there is still insufficient evidence to recommend blood biomarkers as endpoints to monitor changes in fibrosis over time. Any blood-based NILDA that includes age (Table 5) should be used cautiously in children.“
My take: This practice guideline, while recommending use of blood-based tests for fibrosis even in the pediatric age group, makes a fairly compelling argument that they are unreliable in children. Elastrography is likely to be more useful, though also imperfect, in the pediatric population.
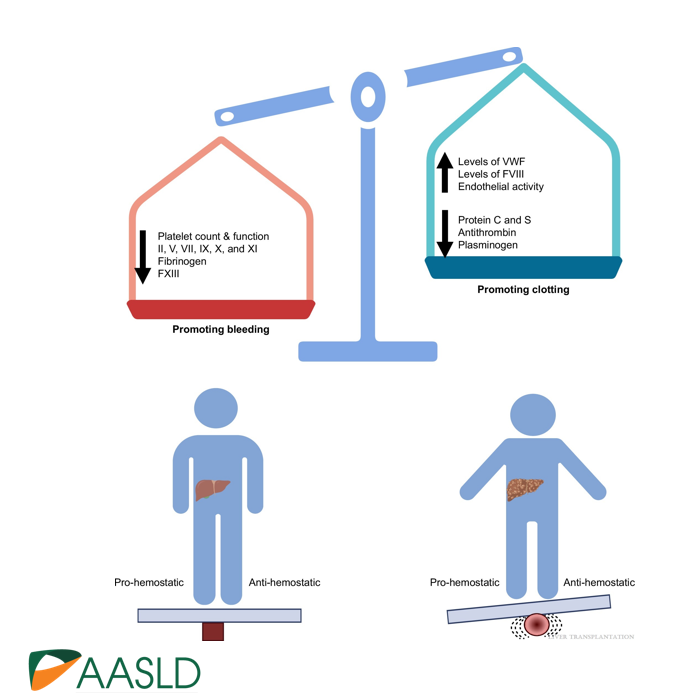
Background: “The most important factor contributing to bleeding risk in patients with liver disease is related to the presence of portal hypertension rather than coagulation abnormalities.1 The changes in the coagulation system in patients with cirrhosis create a re-balanced state, which is prothrombotic. Despite this well-known pathophysiology and recommendation against routine transfusion of blood products (especially fresh frozen plasma) by major guidelines, platelet and fresh frozen plasma transfusion remain a common practice before percutaneous liver procedures.2,3“
Methods: In this retrospective study from three centers in Spain, the researchers enrolled 1797 adults including 316 with cirrhosis (97% had compensated disease). They established a protocol that allowed, at the discretion of the radiologist, to transfuse patients with FFP or platelets if INR was 1.5 or greater or if platelets were 50,000 or below. The primary outcome of the study was major bleeding, which was defined as a drop in hemoglobin (2 or more units) or a need for transfusion of 2 or more units of blood within 1 week after the procedure. This study enrolled patients who underwent percutaneous liver biopsy (86% of cohort) and percutaneous ablation of liver tumors (14% of cohort). Only 6/25 (24%) with INR >1.5 received FFP. 16/22 (72%) with platelet counts below 50,000 received a platelet transfusion. Overall, 7 patients received FFP (1 with cirrhosis, 6 without) and 35 patients received platelets (16 with cirrhosis, 19 without).
Key findings:
Only 14 patients (0.8%) experienced major bleeding after the procedure, and there was no difference between those who had a diagnosis of cirrhosis versus those without cirrhosis. Bleeding occurred in 0.6% of patients with cirrhosis compared to 0.8% of those without.
Only 1 patient with an ablation procedure had major bleeding
Patients with a diagnosis of cirrhosis were more likely to receive a transfusion of any kind
Among those with major bleeding, none met the criteria for transfusion. That is, “no variable was identified to predict the risk of major bleeding.”
My take (borrowed from editorial): This study reinforces the recommendation that “correction of coagulation markers before procedures is unnecessary.”
The editorial notes that “the changes in the coagulation system in patients with cirrhosis create a re-balanced state, which is prothrombotic.
Related blog posts:
Time to Adjust the Knowledge Doubling Curve in Hepatology This post summarizes the following reference: PG Northup et al. Hepatology 2021; 73: 366-413 (346 references) Full text: Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients With Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases PDF version: Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients With Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases. Specific recommendations from this practice guidance: –For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50. –For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
Researchers have corrected a disease-causing gene mutation with a single infusion carrying a treatment that precisely targeted the errant gene.This was the first time a mutated gene has been restored to normal….
The study involved patients who have alpha-1 antitrypsin deficiency, or AATD, a genetic disease that affects an estimated 100,000 Americans…
When the nanoparticles reached the liver, the lipid layer peeled off, releasing the editor — a disabled CRISPR molecule that acted like a GPS for the genome and an enzyme to fix the mutation. The CRISPR molecule crawled along the patient’s DNA until it found the one incorrect letter that needed to be repaired among the three billion DNA letters in the genome. Then the editing enzyme replaced that letter with the correct one… Those who got the highest dose made enough normal alpha-1 antitrypsin to be in a range where no more damage should occur.
My take: This is exciting news, though, long-term data is needed to determine if this will be a durable cure. Cost/availability will be an important consideration if effective.
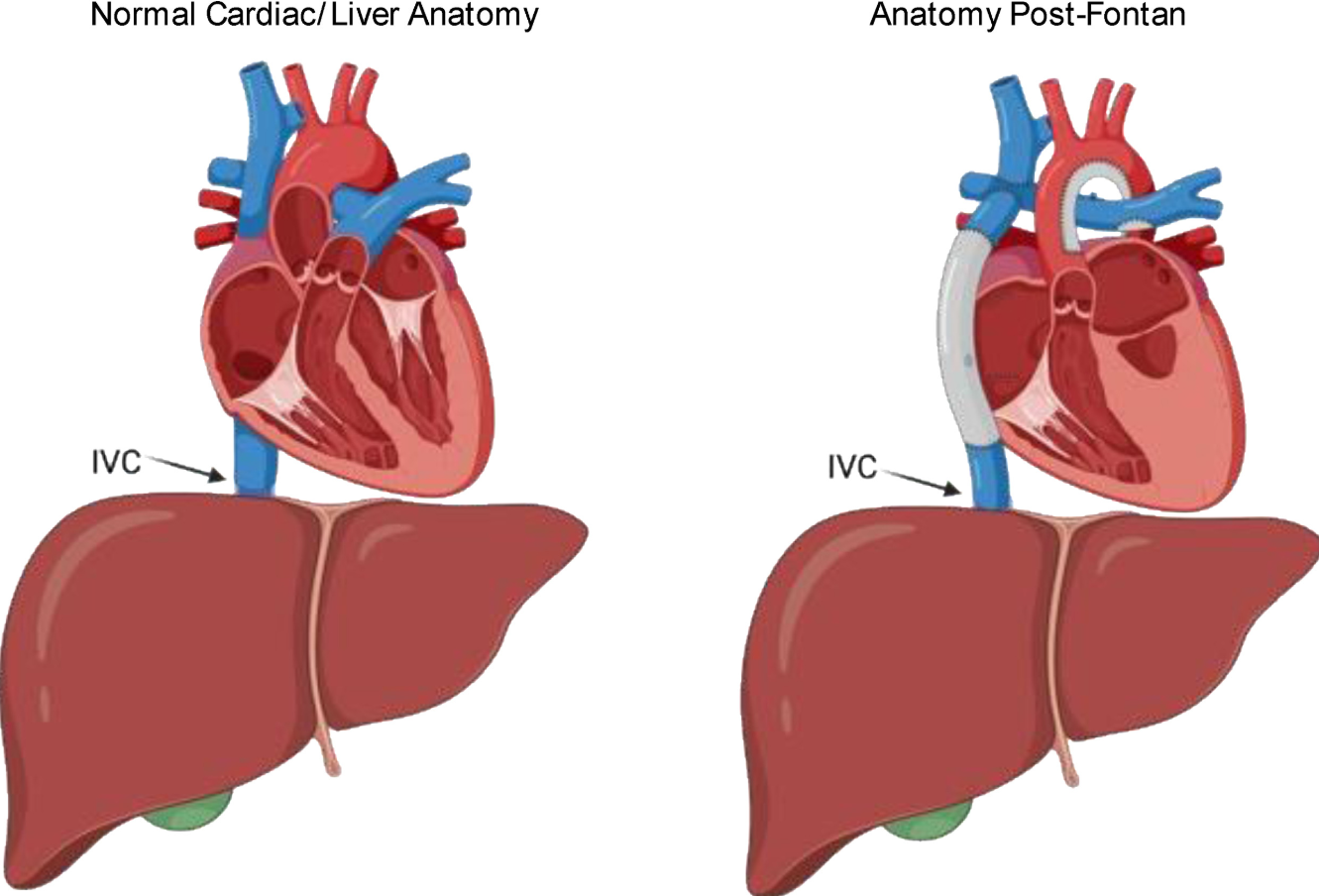
This review article provides a lot of useful advice regarding Fontan-Associated Liver Disease (FALD).
Key points:
FALD prevalence: “will be 70,000 by 2025, with the mean age of 23 years”
Early common manifestations are modest increases in AST and ALT. Elevation of bilirubin is a late finding. Mild elevation of INR is common in range of 1.4 to 1.8.
Ascites occurs in 2-17% of patients with FALD but can be due to other etiologies like PLE
Annual labs (HFP, GGT, CBC/d, PT/INR, AFP) recommended after 7 years post-Fontan
No special diet is recommended but it is worthwhile to avoid fatty liver disease
For varices, a TIPS procedure “may precipitate pulmonary hypertension resulting in cardiac failure.” ‘The safety of a nonselective beta-blocker to prevent a variceal bleed has not been established.” It is important to determine if there are cardiac options that could improve portal hypertension.
In patients with advanced liver disease, multidisciplinary teams are needed to determine if an isolated liver transplantation versus combined heart and liver transplantation (CHLT) is needed.
“If a patient requires a heart transplant, the presence of liver fibrosis or even cirrhosis alone is not an indication for liver transplantation, because cirrhosis has been reported to reverse after isolated heart transplantation in a single provocative case. However, if there is evidence of cirrhosis and liver decompensation, then a CHLT should be considered.”
Many hepatologists recommend trending elastography. Many recommend liver biopsy starting after 10 years status post Fontan
When to refer to hepatology:
Concerning labs: high transaminases, GGT or bilirubin; low albumin (if liver-related), high INR (not due to warfarin), and high AFP
Signs of portal hypertension (eg. splenomegaly, varies, reversal of flow on ultrasound)
Liver masses
More than 10 years post-Fontan. “100% of patients with Fontan circulation will develop liver disease in their lifetime”
My take: There is a lot that we do not know about FALD and management is complex due to coexistent abnormal cardiac physiology.
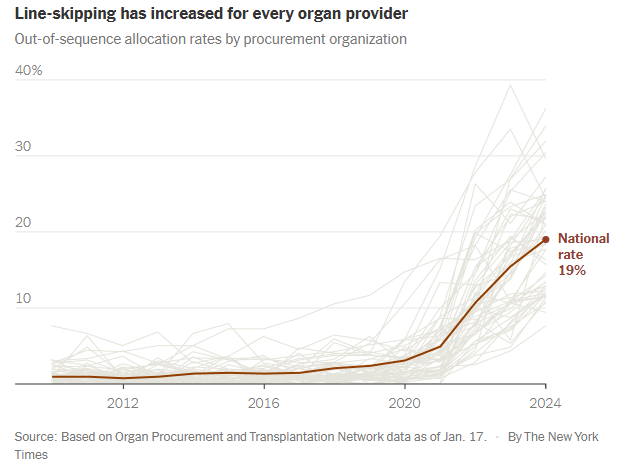
The sickest patients are supposed to get priority for lifesaving transplants. But more and more, they are being skipped over…For decades, fairness has been the guiding principle of the American organ transplant system…today, officials regularly ignore the rankings, leapfrogging over hundreds or even thousands of people when they give out kidneys, livers, lungs and hearts…
Last year, officials skipped patients on the waiting lists for nearly 20 percent of transplants from deceased donors, six times as often as a few years earlier. It is a profound shift in the transplant system, whose promise of equality has become increasingly warped by expediency and favoritism…
Under government pressure to place more organs, the nonprofit organizations that manage donations are routinely prioritizing ease over fairness. They use shortcuts to steer organs to selected hospitals, which jockey to get better access than their competitors.
These hospitals have extraordinary freedom to decide which of their patients receive transplants, regardless of where they rank on the waiting lists. Some have quietly created separate “hot lists” of preferred candidates...
More than 100,000 people are waiting for an organ in the United States, and their fates rest largely on nonprofits called organ procurement organizations…
The procurement organization is supposed to offer the organ to the doctor for the first patient on the list. But the algorithms can’t necessarily identify exact matches, only possible ones. So doctors often say no, citing reasons like the donor’s age or the size of the organ…
Until recently, organizations nearly always followed the list. On the rare occasion when they went out of order and gave the organ to someone else, the decision was examined by the United Network for Organ Sharing — the federal contractor that oversees the transplant system — and a peer review committee. Ignoring the list was allowed only as a last resort to avoid wasting an organ...
Procurement organizations regularly ignore waiting lists even when distributing higher-quality organs. Last year, 37 percent of the kidneys allocated outside the normal process were scored as above-average…
Skipping patients is exacerbating disparities in health care. When lists are ignored, transplants disproportionately go to white and Asian patients and college graduates…
How a rare shortcut became routine
In 2020, procurement organizations felt under attack. Congress was criticizing them for letting too many organs go to waste. Regulators moved to give each organization a grade and, starting in 2026, fire the lowest performers... the organizations increasingly used a shortcut known as an open offer. Open offers are remarkably efficient — officials choose a hospital and allow it to put the organ into any patient...
Open offers are a boon for favored hospitals, increasing transplants and revenues and shortening waiting times. When hospitals get open offers, they often give organs to patients who are healthier than others needing transplants…Healthier patients are likelier to help transplant centers perform well on one of their most important benchmarks: the percentage of patients who survive a year after surgery...
It is impossible to gauge whether line-skipping prevents wasted organs. But data suggests it does not. As use of the practice has soared, the rate of organs being discarded is also increasing.
My take: This article was eye-opening for me as I am not actively involved in listing patients for transplantation. I was unaware of this increasing tendency of line-skipping and open source allocation. It is disturbing to see the distribution process undermined in this manner –better oversight is needed to assure fairness for those whose lives are at stake.
“Let food be thy medicine” is a well-known phrase usually attributed to Hippocrates (though it is unclear if he said this). Regardless, this study indicates that added curcumin in the diet could be beneficial for steatotic liver disease.
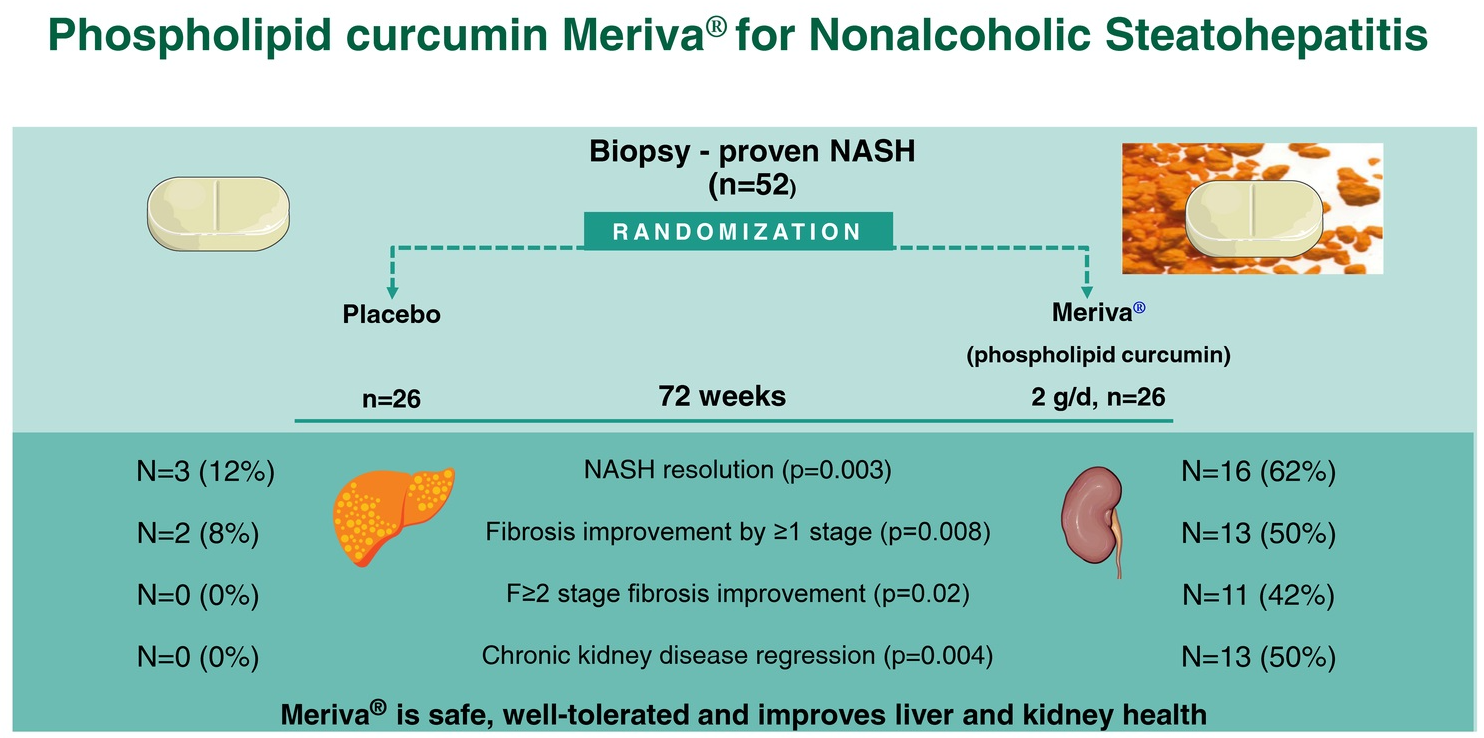
Methods: In this double-blind trial, 52 patients with biopsy-proven NASH (71% with stage ≥F2 fibrosis, 58% with stage A2-G2/A2-G3a chronic kidney disease) were randomized 1:1 to receive Meriva 2 g/d (1 g BID) or placebo for 72 weeks. Meriva is a formulation of curcumin extract with phospholipids that has improved oral bioavailability of curcumin metabolites.
Key findings:
Sixteen (62%) patients on Meriva (curcumin) versus 3 (12%) patients on placebo had NASH resolution (RR = 5.33)
hirteen (50%) patients on Meriva versus 2 (8%) patients on placebo had ≥1 stage fibrosis improvement (RR = 6.50)
Eleven (42%) patients on Meriva versus 0 (0%) on placebo had regression of significant liver fibrosis (RR = 18.01)
Thirteen (50%) patients on Meriva versus 0 (0%) on placebo had chronic kidney disease regression (RR = 10.71)
Compared with placebo, Meriva improved eGFR (difference in adjusted eGFR change: +3.59 [2.96–4.11] mL/min/1.73 m2/y, p = 0.009), fasting glucose(−17 mg/dL; 95% CI = −22, −12), HbA1c (−0.62%; 95% CI = −0.87%, −0.37%), LDL-C (−39 mg/dL; 95% CI = −45, −33), triglycerides (−36 mg/dL, 95% CI = −46, −26), HDL-C (+10 mg/dL; 95% CI = +8, +11), and inflammatory markers
The observed benefits were associated with downregulation of hepatic NF-kB which is a proinflammatory transcription factor and a known curcumin target
My take: A larger multicenter study is needed to confirm these promising results. This study shows that dietary changes and lifestyle modification remain important tools in treating MASH (aka NASH).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
GI and Hepatology News, Open Access: Watershed Moment’: Semaglutide Shown to Be Effective in MASH (November 2024): “At 72 weeks, a 2.4-mg once-weekly subcutaneous dose of semaglutide demonstrated superiority, compared with placebo, for the two primary endpoints: Resolution of steatohepatitis with no worsening of fibrosis and improvement in liver fibrosis with no worsening of steatohepatitis.”
“ESSENCE (NCT04822181) is an ongoing multicenter, phase 3 randomized, double-blind, placebo-controlled outcome trial studying semaglutide for the potential treatment of MASH.” Cohort: N=1200, biopsy-defined MASH and fibrosis, stages F2 and F3…”After initiation, the semaglutide dosage was increased every 4 weeks up to 16 weeks when the full dose (2.4 mg) was reached.”
Key findings:
62.9% of those in the semaglutide group and 34.1% of those in the placebo group reached resolution of steatohepatitis with no worsening of fibrosis.
37% of those in the semaglutide group and 22.5% of those in the placebo group had improvement in liver fibrosis with no worsening of steatohepatitis
Weight loss was also significant, with a 10.5% reduction in the semaglutide group compared with a 2% reduction in the placebo group
No new safety signals were identified
Cardiometabolic risk factors improved as well, with changes in blood pressure measurements, hemoglobin A1c scores, and cholesterol values.
20%-40% improvements in liver enzymes and noninvasive fibrosis markers, such as ELF and vibration-controlled transient elastography liver stiffness.
My take: This expected finding indicates that more GLP-1 agents are likely to be approved for MASH treatment. Survodutide received “U.S. FDA Breakthrough Therapy” in October 2024.