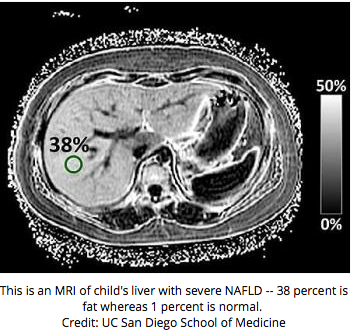
A recent study (JB Schwimmer et al. Hepatology 2015; 1887-95, editorial Vos MB, pages 1779-80) examines the accuracy of magnetic resonance imaging (MRI) compared with liver histology in children with nonalcoholic fatty liver disease.
This prospective validation study enrolled 174 children with a mean age of 14 years. The MRI estimated the liver proton density fat fraction (PDFF).
Key findings:
- Liver MRI-PDFF correlated with steatosis grade; the correlation was particularly strong at high and low end values. Thus, a very low MRI-PDFF was highly likely to predict a steatosis grade 0 or 1 while a very high value corresponded to high steatosis levels.
- Liver MRI-PDFF was weaker in children with stage 2-4 fibrosis than in children with no fibrosis
The editorial notes that this study “is one of hundreds now published in the literature on MRI and NAFLD…The superiority of MR-based methods…over ultrasound is clear. The question is why are we still ordering abdominal ultrasounds to diagnose NAFLD in children?” The barriers for usage of MRI include cost, potential sedation, and nonuniform methods for MRI usage.
The paper conclude that “MRI is not yet sufficient to replace liver biopsy in children.” The editorial also indicates that the MRI era is fast approaching but not viable today.
Take-home point: Due to the huge numbers of patients with pediatric NAFLD, MRI remains a terrific area for research but remains problematic in clinical practice. Given the expense of MRI, until its use can reduce liver biopsies or improve management, its role is likely to remain limited.
- Imaging in NAFLD -Don’t Rely on Ultrasound | gutsandgrowth
- Increasing prevalence of pediatric NAFLD | gutsandgrowth
- NAFLD -Analogous to a Dog Chasing A Bus? | gutsandgrowth
- Screening for NAFLD | gutsandgrowth
- NAFLD Guidelines 2012 | gutsandgrowth
- Pediatric NAFLD Position Paper | gutsandgrowth

Turner Field