N Du, C Torres. JPGN 2024;78:1149–1154. Prevalence of eosinophilic gastrointestinal diseases in children with short bowel syndrome: A single center study
Methods: EoEdefined as ≥15 eosinophils per high powered field (HPF), eosinophilic gastritis (EoG) as ≥30 eosinophils per HPF, eosinophilic enteritis (EoGN) as >50 eosinophils per HPF, and eosinophilic colitis (EoC) as>80–100 eosinophils per HPF.
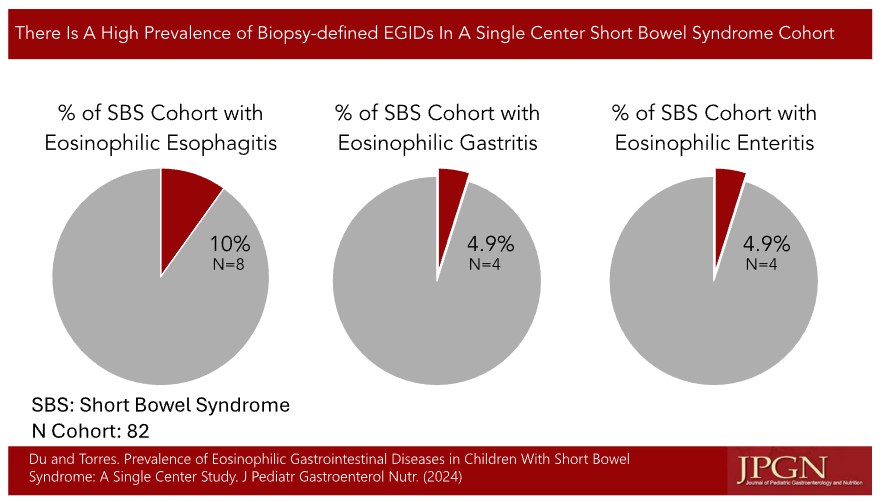
Key findings in this retrospective study (n=82):
- The prevalence of eosinophilic esophagitis in our SBS cohort was10%, eosinophilic gastritis was 4.9%, and eosinophilic enteritis was 4.9%
- SBS patients with history of allergy or atopy were more likely to have esophageal and intestinal eosinophilia on biopsy than patients without allergy
- One patient had EoC
In their discussion, the authors speculate on the potential role for dysbiosis, possibly related to parenteral nutrition. They note that “rare SBS patients were on amino acid‐based formulas alone and almost all were exposed to food allergens around the same age as the general population.” I did not see any information about PPI use in this cohort.
My take: This report reinforces the fact that eosinophilic disorders are more frequent in SBS (see related post below). The exact role of altered diet/use of amino acid based formulas and the role of medications like PPIs in regards to the development of EGIDs remains unclear.
Related blog posts:
- Eosinophilic Disease in Children with Intestinal Failure (re: J Pediatr Gastroenterol Nutr. 2016;63:336‐339)
- Practical Intestinal Rehabilitation (Part 1)
- Practical Intestinal Rehabilitation (Part 2)