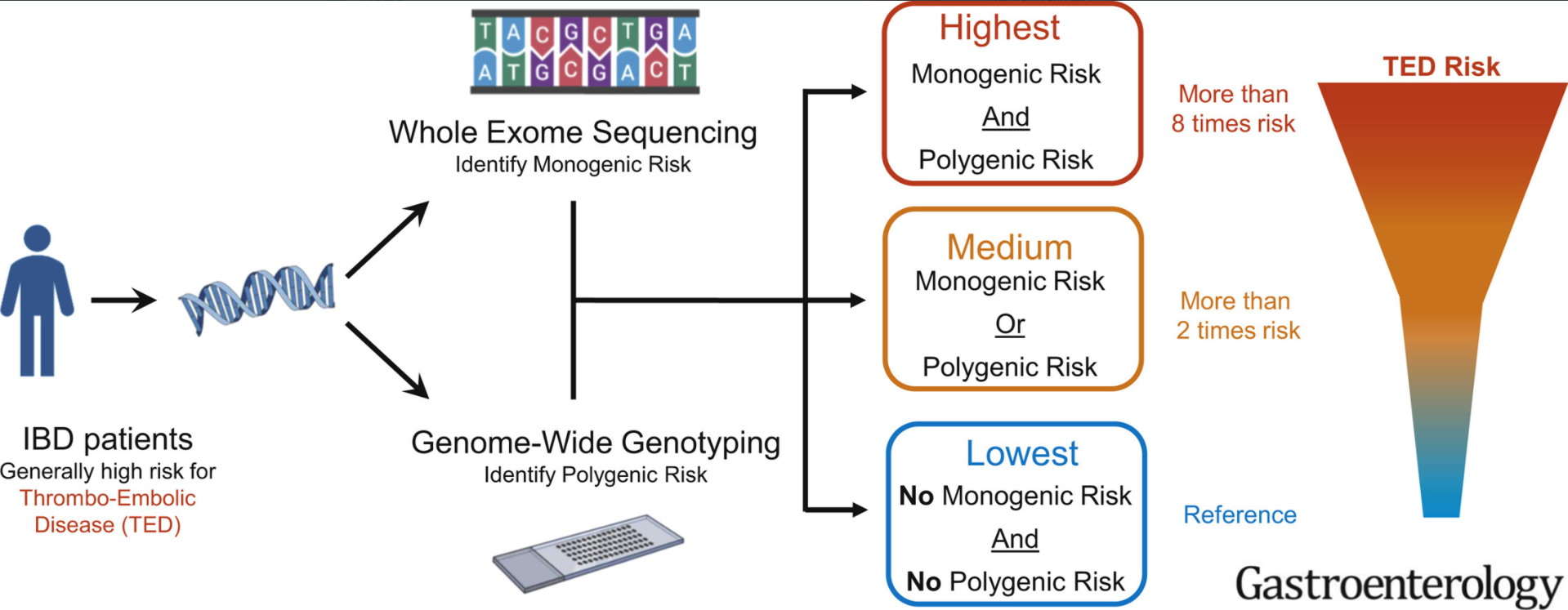
T Naito et al. Gastroenterol 2021; 160: 771-780. Full text: Prevalence and Effect of Genetic Risk of Thromboembolic Disease in Inflammatory Bowel Disease
Background: 10% of healthy subjects are genetically at high risk for thromboembolic disease (TED). For adults with inflammatory bowel disease, TED is “largest cause of mortality in
patients”
Key findings:
- In total, this retrospective study had 792 IBD patients who had both whole-exome sequencing and genotyping data to identify thrombophilia pathogenic variants. 122 of 792 IBD patients (15.4%) as genetically high risk for TED.
- Genetic TED risk was significantly associated with increased TED event (odds ratio,2.5; P ¼ .0036).
- Patients with high TED genetic risk more frequently had thrombosis at multiple sites (78% vs 42%, odds ratio, 3.96; P ¼ .048)
“Our analyses demonstrate that approximately 1 in 7 patients with IBD have odds 2.5 times higher than nongenetically high-risk patients with IBD for experiencing TED.” The risk of TED in IBD is generally 3- to 4-fold higher than the general population
My take: In children, the risk of clots is much lower than in adults. Thus, the potential to identify those at highest risk would be useful in order to target interventions. Also, patients at higher risk for TED may affect choice of treatment (eg. avoiding JAK inhibitors).
Related blog posts:
- Venous Thromboembolism: A Good Question for Pediatric Collaboration | gutsandgrowth
- Venous Thrombosis in Pediatric Inflammatory Bowel Disease | gutsandgrowth
- VTE in IBD
From The Onion: