Using the Inform Diagnostics database, which is a national electronic repository of histopathologic records from patients distributed throughout the entire United States, the authors performed a case-control study among 302,061 patients undergoing bidirectional endoscopy on the same day.
The database contained 3860 ulcerative colitis (UC) patients, 3330 Crohn’s disease (CD) patients, 1476 patients with indeterminate colitis with respect to UC or CD, and 5296 MC (microscopic colitis) patients.
Key findings:
EoE was less common in the overall IBD, CD, and MC case populations than the control population. Adjusted odds ratios (compared to control) :
EoE and IBD aOR 0.64
EoE and Crohn’s aOR 0.41
EoE and UC aOR 0.97
EoE and Indeterminate Colitis aOR 0.29
EoE and MC aOR 0.68
My take: (partly from authors) “Unexpectedly, the present analysis revealed statistically significant inverse relationships between EoE and CD or MC, but not UC.” Because endoscopy is often undertaken in those with a suspicion of IBD, EoE can be identified in the IBD population surreptiously; however, its frequency is likely less than in the general population.
This is a very useful article with recommendations for central venous access in children. The main recommendations are summarized in Table 3 & listed below; however, there is a lot of detailed information in the article on frequent issues like schools, travel (including dealing with TSA), sports, and even swimming. In addition, the article delineates recommendations for management and prevention of line complications.
1. Recommendations for venous access:
Tunneled, single lumen, cuffed silicone catheters should be used for children with IF.
Upper extremity access is the preferred location when available.
2. Recommendations pertaining to routine CVC care:
Proper technique and hygiene surrounding CVC care are of paramount importance in preventing CVC-associated complications. Caregivers should receive directed education regarding CVC care before initial discharge, with subsequent reinforcement education as needed.
CHG impregnated supplies (disk, sponge, or dressing) should be considered for central line dressing in pediatric IF patients.
Routine surveillance of central venous access should be performed by US. MR, CT, or traditional venography should be reserved for when further delineation of access is required.
3. Recommendations regarding general considerations—sports, travel, and emergencies:
All children with IF should be provided with an emergency letter that details the specific needs of the individual child in case of an emergency. (See at bottom for example -Figure 1)
Discuss with families the risks of swimming and sports participation with strategies to protect the dressing and central line.
All travel plans should be discussed with the intestinal rehabilitation team well in advance of travel to facilitate discussion of a plan of care in case of emergency.
4. Recommendations regarding central line-associated bloodstream infections:
All children with IF and CVC who develop a fever (≥38.0°C) should be admitted to the hospital and assessed for bacteremia with central and peripheral blood cultures while receiving broad-spectrum empiric antibiotics through the CVC for at least 48 h, awaiting culture results regardless of other infectious sources.
If clinically stable, discuss with the patient’s IRP before line removal for CLABSI.
Prophylactic lock therapy with ethanol or other nonantibiotic locks should be strongly considered in all children with IF who have had at least one central line-associated bloodstream infection or are at high risk for infection.
5. Recommendations pertaining to central line mechanical complications:
In children with IF, CVC should be repaired whenever possible to preserve central venous access.
Children with IF and a newly identified CRT should be treated with low molecular weight heparin for at least 6 weeks with guidance from a hematologist.
Children with IF who have persistence of at least one chronic thrombus should be maintained on prophylactic anticoagulation with low molecular weight heparin.
Children who have lost multiple sites of central venous access should be considered for referral to an intestinal transplant center for evaluation and management
6. Recommendations for central venous access program management:
All centers following children with IF should, at a minimum, track the number of outpatient CLABSI per 1000 catheter days.
With regard to swimming: “Swimming introduces an incompletely defined but potentially severe risk to those requiring chronic central venous access. Contamination of various chlorine-treated (swimming pools), stagnant (lakes and ponds), and flowing (oceans and rivers) bodies of water with human pathogens has been well documented, though proper maintenance may minimize outbreaks. The potentially fatal risk of such contaminants gaining access to central circulation via the CVC is unclear…Parents seeking guidance are confronted by mixed messaging from support programs, online resources and blogs, and even IRP. These conflicting recommendations and practices reflect the paucity of data to guide a safe and clear approach for swimming with a central line…[in one study of 16 home PN programs] swimming in low-risk situations [was permitted but] recommended immediate site cleaning and dressing change following water exposure and avoidance of submersion for 4–6 weeks after CVC placement. Ultimately, the decision to permit children with IF to swim lies with the parent or guardian.”
For pets (like Charlie), this article notes that “steps should be taken to promote line integrity in the presence of pets. Particularly in the setting of pets that may attempt to chew or play with tubing, adequate physical protection of the insertion site and catheter itself is recommended. Any line or tubing puncture by an animal should prompt immediate evaluation. Family awareness of zoonotic disease risk and advocacy of handwashing before and after animal care should be made clear.”Figure 1 -Emergency Letter Template
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This small (n=28) retrospective study provides useful information on the persistence of feeding problems in children with short bowel syndrome (SBS). The authors defined a pediatric feeding disorder (PFD) as “reliance on enteral feeds to sustain nutrition, reliance on high-calorie oral supplements to sustain nutrition, or feeding skill dysfunction resulting in not consuming an age-appropriate diet.” Patients who remained on PN were considered to have a PFD as well.
Key findings:
Of the 21 patients (75% of total cohort) who were weaned off parenteral nutrition, 57.1%, 81.0%, 90.5%, and 100.0% achieved this by 12, 24, 36, and 48 months of age, respectively. Median age at time of weaning PN was 10.8 months.
Of the 13 patients who were weaned off enteral nutrition (EN), 30.8%, 69.2%, 76.9%, and 100.0% achieved this by 12, 24, 36, and 48 months, respectively. Median age of weaning EN was 15.7 months. Overall, about a third of patients required EN beyond 2 years of life.
The prevalence of PFD (of entire cohort) was 100.0%, 76.5%, 68.8%, and 70.0% at 1, 2, 3, and 4 years of age, respectively
My take: When parents ask how long it will be before my child is off PN and eating by mouth, this study’s results could be useful.
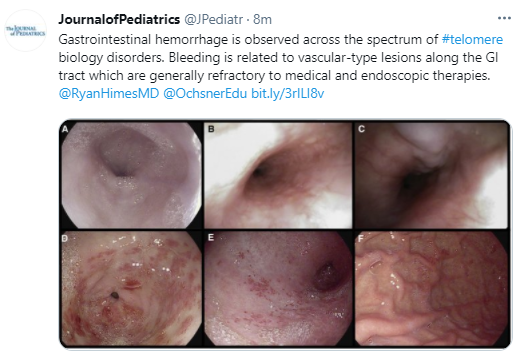
Background: Telomere biology disorders are a complex set of illnesses defined by the presence of very short telomeres; these individuals are at very high risk of bone marrow failure, cancer, and pulmonary fibrosis. There are 15 known genes which can experience damaging mutations, or other abnormalities, that can cause very short telomeres (for example the telomerase genes TERC and TERT). The most widely recognized telomere biology disorder is known as dyskeratosis congenita (DC); others include Hoyeraal-Hreidarsson syndrome, Revesz syndrome, and Coats plus.
Key findings:
Sixteen patients who experienced GI hemorrhage were identified at 11 centers. Ten patients had a history of hematopoietic cell transplantation.
Initial GI bleeding occurred at a median of 12.5 years.
Angiodysplasia of the stomach and/or small bowel was described in 8 of the 12 patients who underwent endoscopy; 4 had esophageal varices. The lesions were often diffuse and widespread (see Figures 1 & 2).
GI bleeding appeared to be more prevalent in those with TINF2, CTC1 or STN1 mutations (12 of 14 with genetic testing).
Recurrence was common, and the overall long-term outcome for affected patients was poor. 12 of 16 were deceased at time of data collection (median age of 16.5 years at time of death), though the proximate cause of death was not reported.
No single intervention was uniformly associated with cessation of bleeding, although 1 patient had a sustained response to treatment with bevacizumab. Other treatments that were tried included endoscopic treatments, thalidomide, octreotide, proton pump inhibitors, sirolimus and hormonal treatments.
My take: GI bleeding in these rare disorders is a difficult clinical problem.
This is a very useful article. Table 3 lists many of the features of some monogenic inflammatory bowel disease (IBD). Table 4 details potential immune workup tests. Table 5 lists 75 genes that should be included when testing for monogenic IBD.
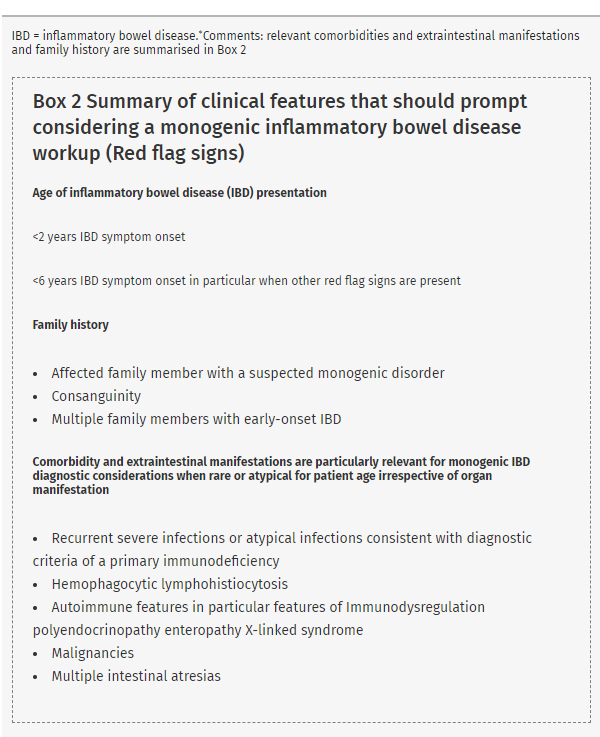
Box 2 (see below) provides a list of conditions that should prompt consideration of genetic testing. Figure 1 provides an algorithm for testing.
Table 6 provides a summary of statements
#3:”Genetic screening for monogenic IBD is recommended in all patients with infantile-onset IBD (<2 years) and should be considered in patients with very early-onset IBD (<6 years), in particular, in those patients with relevant comorbidity, extraintestinal manifestations, and/or family history”
#5: “Routine genetic screening for all IBD patients is not recommended since a monogenic cause of IBD in patients with IBD onset over 6 year of age, especially those with adolescent or adult age onset of IBD is exceptional in the absence of relevant comorbidity”
There is also some advice on variants of unknown significance: “Databases, such as Clinvar, ClinGen, or The Human Gene Mutation Database can help to assess variant phenotype relations”
In this prospective study, the authors enrolled asymptomatic pediatric patients (n=225) and compared C diff testing results with symptomatic patients (n=41) with positive nucleic-acid amplification-based testing (NAAT).
Key findings:
Of the 225 asymptomatic children enrolled in the study, 47 (21%) were colonized with C. difficile including 9/59 (15.5%) with cancer, 30/92 (32.6%) with CF, and 8/74 (10.8%) with IBD.
Overall, “use of a multistep testing algorithm with NAAT followed by EIA failed to differentiate symptomatic CDI from asymptomatic colonization in our pediatric cohort.” When symptomatic and colonized children were compared, neither EIA (enzyme immunoassay) positivity (44% vs 26%, P = 0.07) nor CCNA (functional cell cytotoxicity neutralization assay) positivity (49% vs 45%, P = 0.70) differed significantly
My take: Don’t test children who are asymptomatic for Clostridium difficile. Even in children with symptoms, C diff positivity could reflect colonization and symptoms could be due to other etiologies.
Among FOLE recipients (n=189), 65% experienced cholestasis resolution vs 16% of SOLE recipients (n=73) (P < .0001).
The aspartate aminotransferase to platelet ratio index scores improved in FOLE recipients (1.235 vs 0.810 and 0.758, P < .02) but worsened in SOLE recipients (0.540 vs 2.564 and 2.098; P ≤ .0003)
Liver transplantation was reduced in FOLE vs SOLE (4% vs 12%; P = .0245).
My main criticisms of the study:
While the methods explain that FOLE received 1 gm/kg/d, compared with 3 gm/kg/d for SOLE, this was NOT reviewed in the discussion. This is quite important in terms of proving that one product is preferred over the other. With lipid toxicity, it would be expected that delivering 3 times as much would be more damaging on the liver.
The discussion does not discuss the potential neurological consequences of lipid minimization/lower doses of lipids. In the same Journal of Pediatrics issue, Bell et al report that 77% of SBS in their cohort of extremely premature infants with short bowel syndrome had moderate-to-severe neurodevelopmental impairment (related blog post: Neurodevelopmental Impairment in the Majority of Extremely Premature Infants with Short Bowel Syndrome)
The discussion has only a single sentence regarding the change in care between the eras of SOLE and FOLE: “Additional limitations include a relatively small sample size and changes in surgical, medical, and nutritional practice between the 2 eras that could not be controlled for this study.”
Also, the discussion omits the development of other FOLE alternatives (eg. SMOFlipid) which has been a very important advance in the management of patients with SBS.
The commentary by Samuel Kocoshis (J Pediatr 2021; 230: 11-12) provides a good deal of insight. The title and first paragraph provides some interesting historical context: (full text) “Even When the Would Is Healed, the Scar Remains” “The above maxim was coined by the Roman author Publilius Syrus when referring to wounds of most tissues or body parts.1 Because hepatic regeneration was recognized (as evidenced by the story of Prometheus’s liver being eaten daily by an eagle only to regenerate the next day) in Syrus’s time, his dictum was too far too simplistic when applied to the liver. One must delve more deeply into the mechanism of liver injury to ascertain just when hepatic scaring persists or when it disappears.”
My take: This study illustrates harm reduction with the change in lipid administration. The development of new lipid products has made a huge difference in the outcomes of children with short bowel syndrome.
CHOA Nutrition Support Core Seminar -Thanks to Kipp Ellsworth for organizing this series and sharing content. This lecture is a really good review and would be a great place to start when discussing formulas with medical students and residents.
Link to Webex (49 min): “Pediatric Formula Basics” by Clancy Bryant, MS, RD (March 2, 2021). Password: FbhSgup5
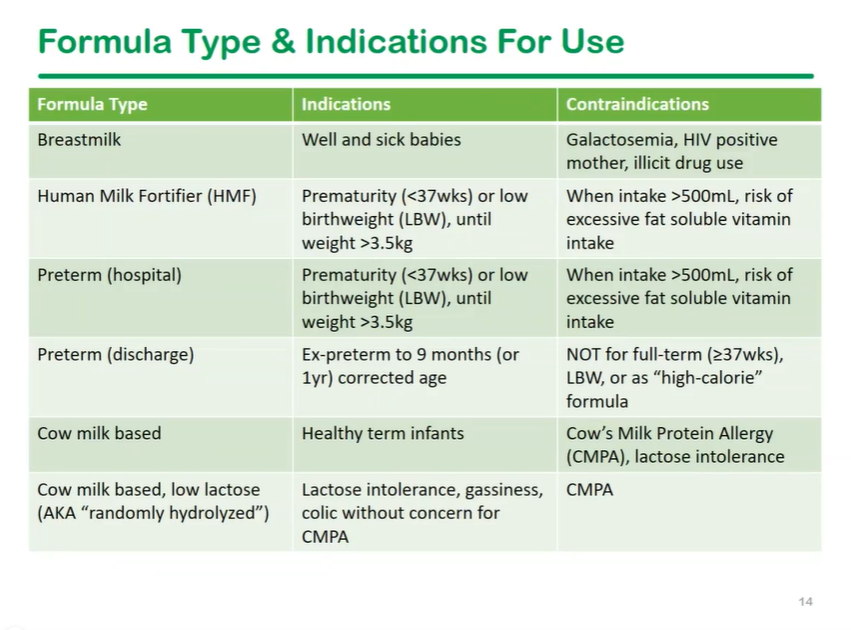
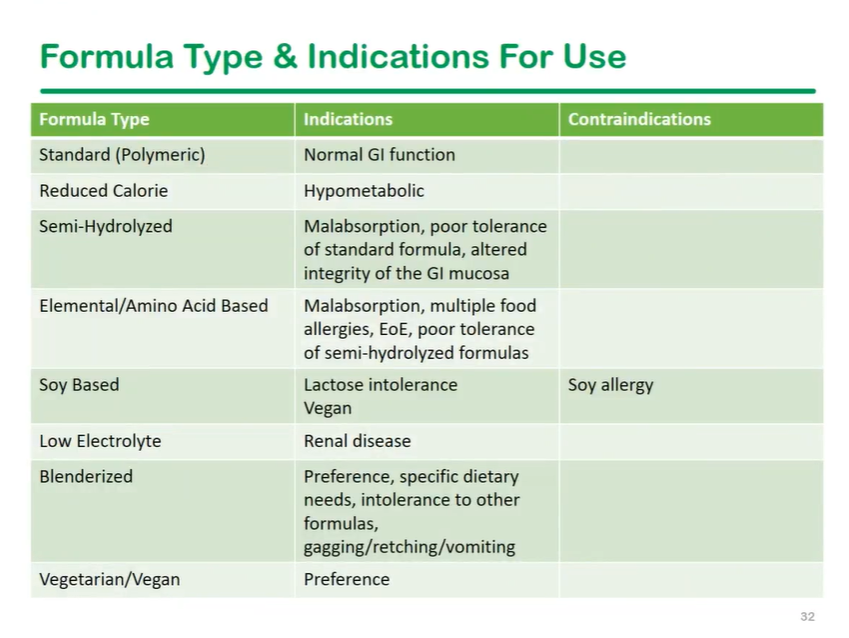
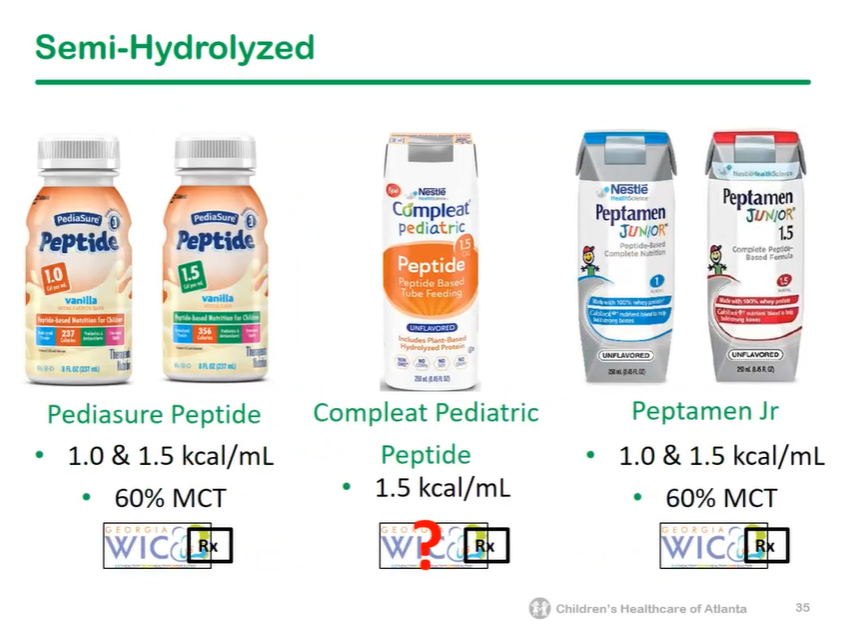
This lecture reviewed selection of formulas for infants, children and adolescents; some of the most common formula choices (but not all) were reviewed
This talk reviewed reflux guidelines as reflux symptoms often impact decisions on formula choice in infancy. Thickened formulas like Enfamil AR and Similac Spit Up do not work with acid suppression medications.
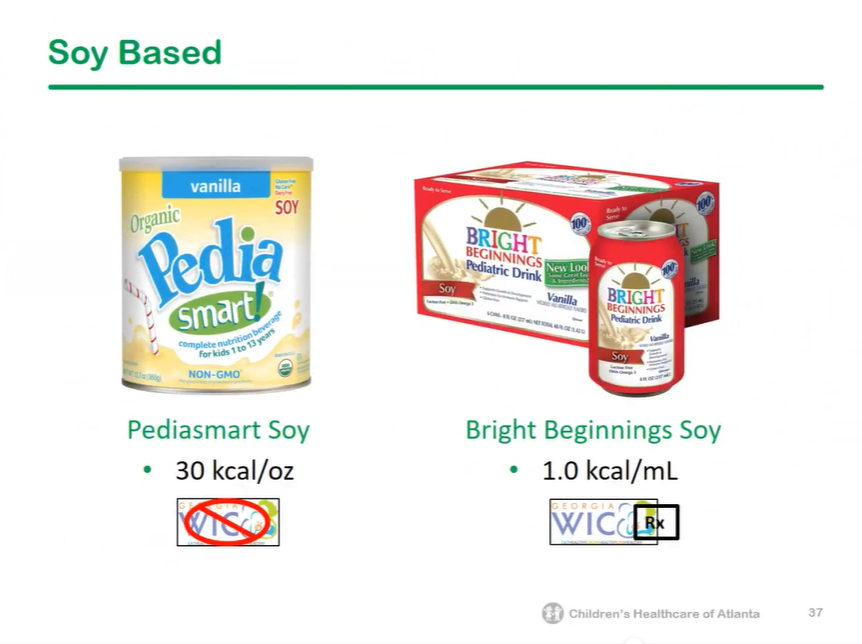
WIC script requires 2 ICD-10 diagnosis which are relevant to chosen formula
For standard formula, no prescription is needed; if formula is not on WIC formulary, it will not be covered
If child is NPO, write for “patient is NPO, please give maximum formula”
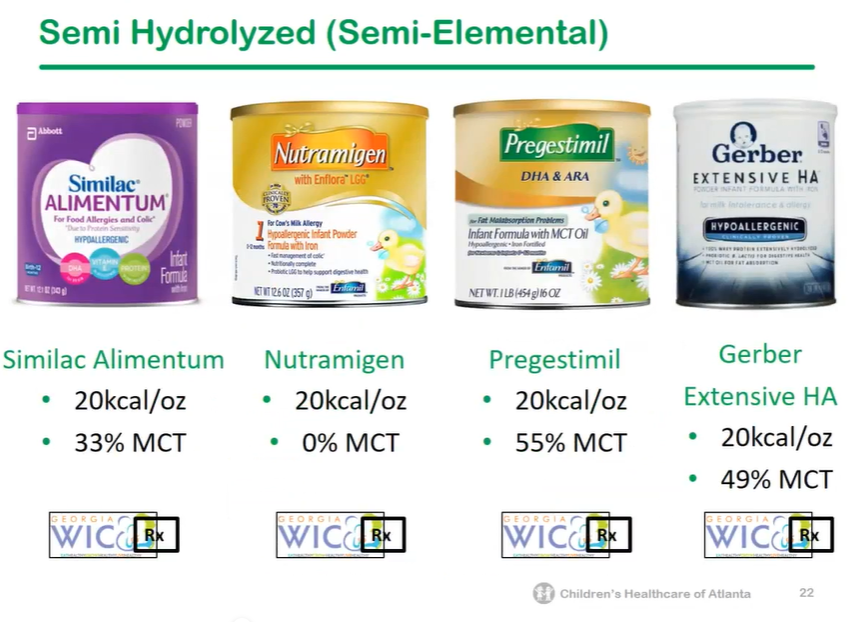
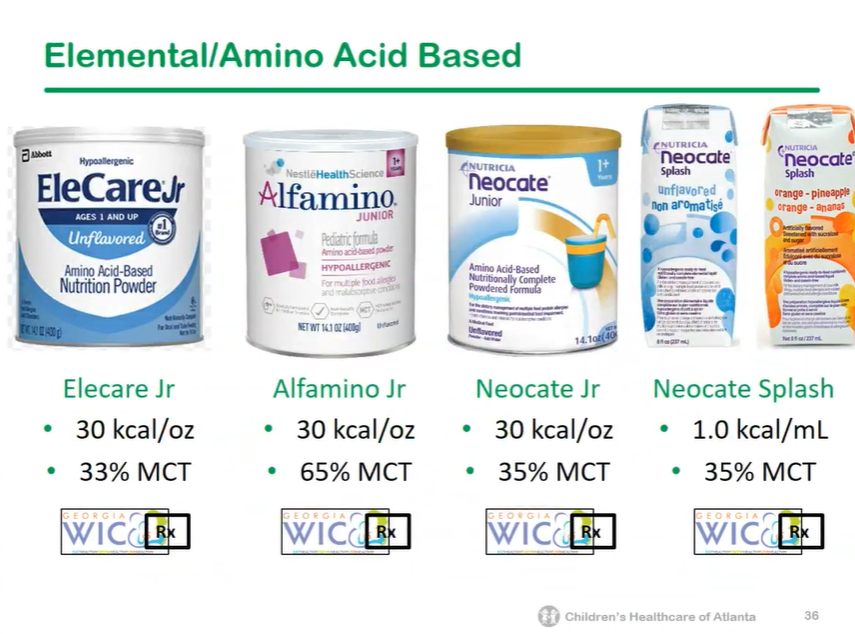
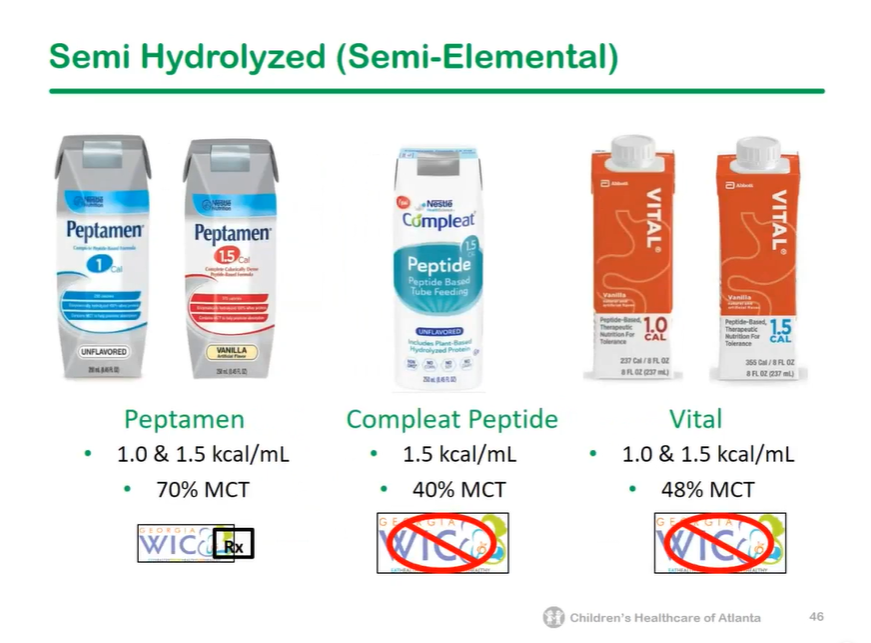
For cholestatic liver disease: high MCT formulas include pregestamil (55%), Alimentum (33%) and elemental formulas (33-49%)
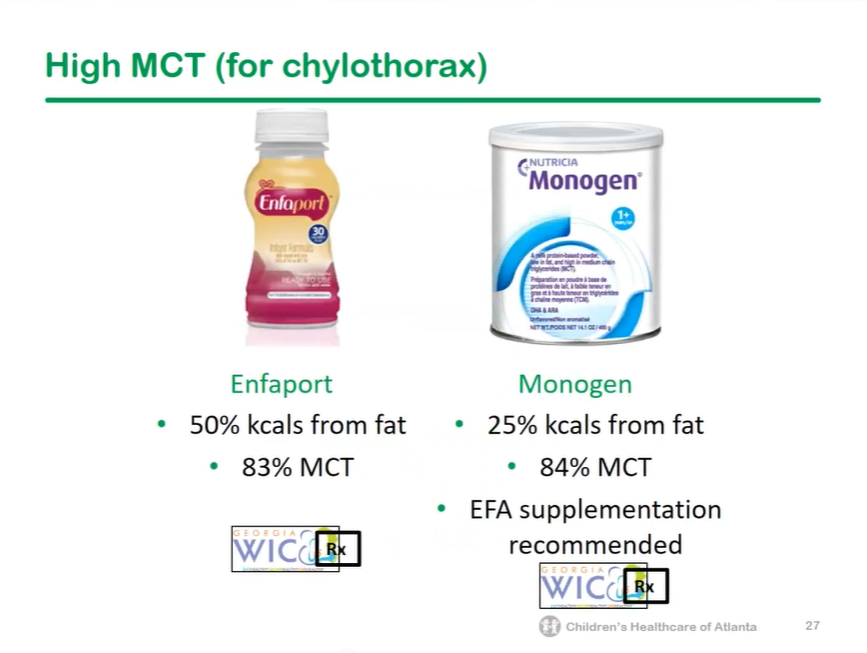
For chylous effusions, very high MCT formulas (83%, 84%) include enfaport and monogen (needs EFA supplementation)
Formulas for children and adolescents come in concentrations of 0.6 kcal/mL to 2.0 kcal/mL
Reduced calorie formulas (eg. Pediasure Reduced Calorie or Compleat Pediatric Reduced Calorie) are helpful to provide adequate micronutrients/protein in children with hypocaloric needs
Blenderized formulas often helpful for children with retching (when given via gastric route); some of these may increase vitamin A levels and beta-carotene (eg. Nourish, Compleat Pediatric Organic Blends). Real food blends are not nutritionally-complete. Harvest is able to run through enteral tube without dilution.
For those older than 10 years of age, Liquid Hope is similar to Nourish and Compleat Organic Blends is similar to Compleat Pediatric Organic Blends
Low electrolyte formulas, like Renalcal and Renastart, may be useful for children with kidney dysfunction. Corresponding formulas for >10 years of age include Suplena and Novasource Renal
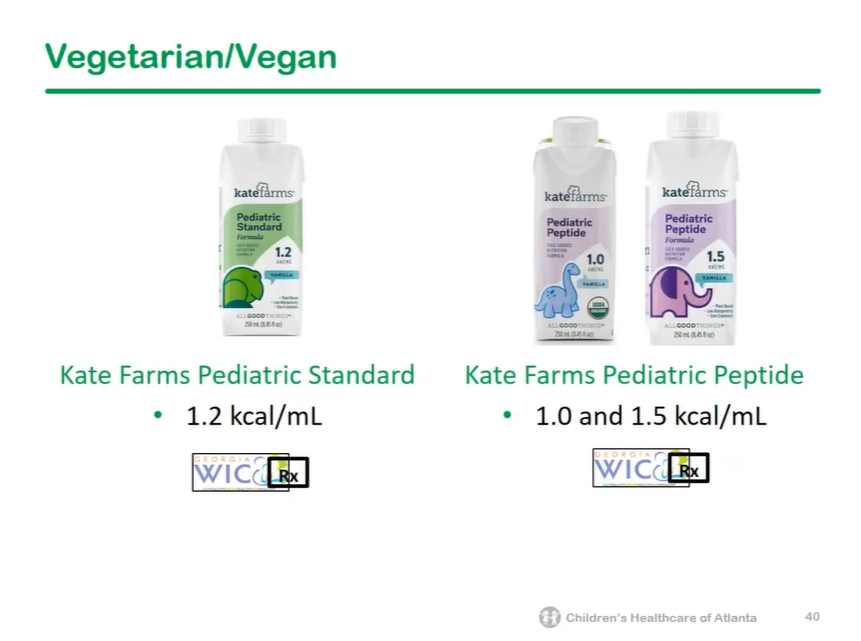
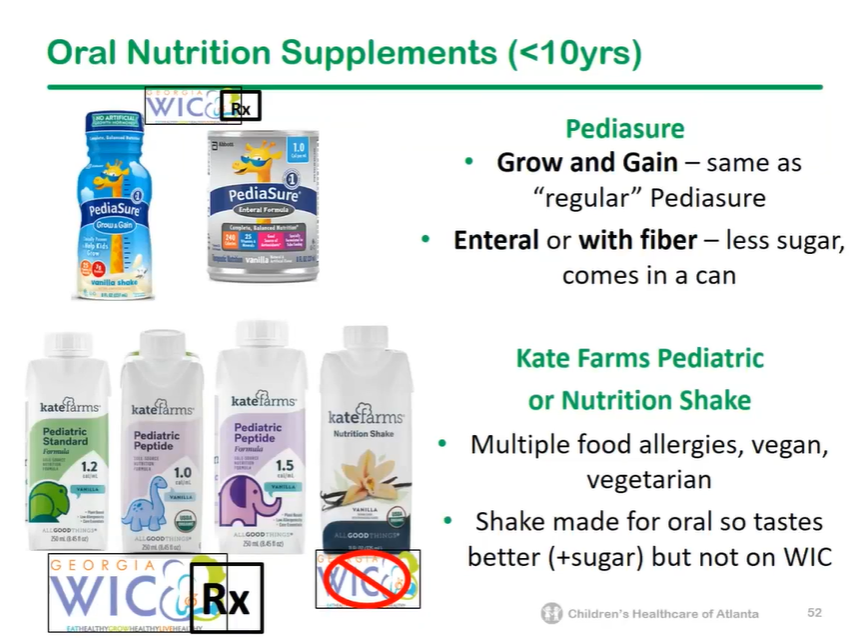
Kate Farms is often a good choice for patients with multiple allergies or eosinophilic esophagitis
In patients receiving anti-TNF agents which are usually effective for CRMO, CRMO may develop paradoxically and may be associated with a psoriaform reaction.
At the time of diagnosis of paradoxical reaction, all patients were in remission due to anti-TNFα efficiency. Trough levels of anti-TNFα were in the expected range, and there were no anti–anti-TNFα antibodies.
All patients recovered after discontinuation of infliximab (n = 2) or adalimumab (n = 1).
My take: This study describes a rare adverse effect of anti-TNFα agents. If CRMO develops while on one of these agents, an alternative treatment is needed.
Key findings from this double-blind randomized controlled trial (n=121):
ICU admissions were 9.8% in LR group compared with 25% of NS group (RR 0.4, CI 0.2-0.9)
Quicker discharge with 44% at 72 hrs in LR group compared with 28% in NS group
Median length of stay was 3.5 days (LR group) compared with 4.6 days (NS group)
Critique of study from editorial: “The strengths of their study include a well-designed protocol, reasonable sample size and inclusion of patients within 8 hours of diagnosis; thus, fluids were administered during the critical period when there is a window of opportunity to restore the intravascular volume and maintain adequate tissue perfusion. However, the study included patients with mild pancreatitis. Another issue is that the benefit shown was for secondary outcomes and, thus, these results should be taken as exploratory and hypothesis generating.”
My take: For now, lactated ringer’s is the fluid of choice in individuals with acute pancreatitis.