Dr. Joseph D. Feuerstein, gastroenterologist at Beth Israel Deaconess Medical Center in Boston… “It’s rising in incidence and prevalence throughout the world,” he said, and gastroenterologists are still trying to figure out why it shows up when it does in different people.
Crohn’s disease was first described in 1932 by Dr. Burrill B. Crohn…
Prompt diagnosis and appropriate therapy to suppress inflammation in the digestive tract are extremely important because a delay can result in scar tissue and strictures that are not reversed by medication…
Crohn’s is not curable and most patients have to stay on medication indefinitely. That can create yet another stumbling block. The biologics are very costly…
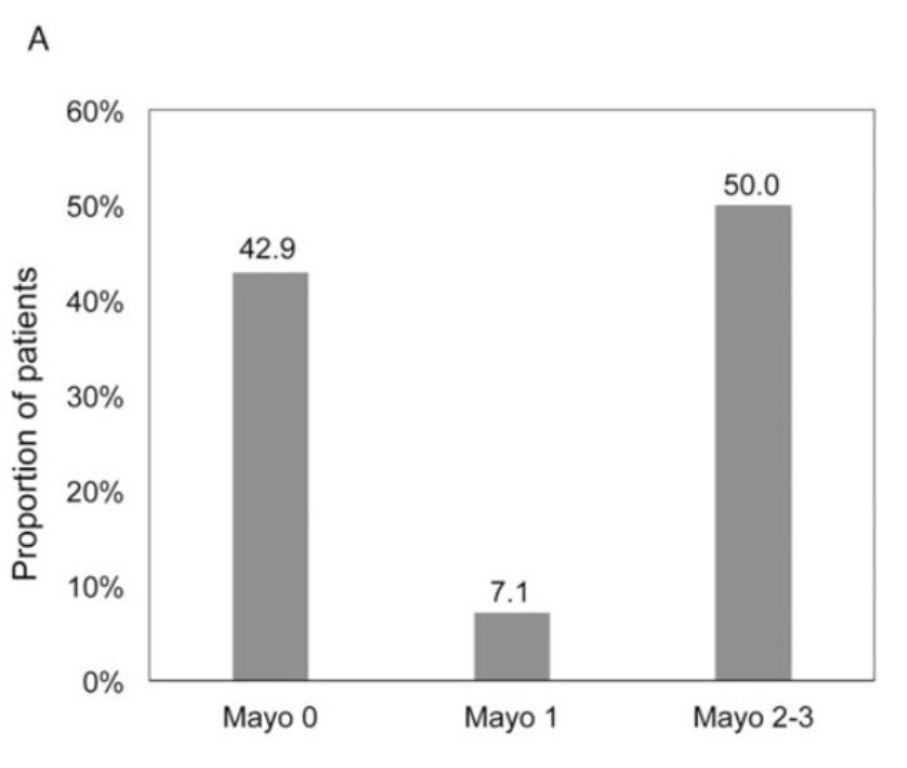
This study prospectively assessed for mucosal healing by endoscopy 3 to 5 months after clinical remission, PUCAI <10, was documented. Key findings:
28 children in continuous clinical remission at time of sigmoidoscopy were included. Mayo 0 was present in 12/28 (43%), Mayo 1 in 2/28 (7%) and Mayo 2 to 3 in 14/28 (50%) endoscopies.
Among 23 patients with follow-up through 18 months, remission was sustained in 6/12 (50%) with Mayo score 0 to 1 versus 2/11 (18%) of patients with Mayo 2 and 3
16 (57%) of the patients were receiving 5-ASA treatment
It would have been helpful to have calprotectin values as well. In their discussion, the authors note that “a normal calprotectin is quite convincing with regard to endoscopic remission” and ECCO ESPGHAN guidelines “provide guidance that a colonoscopy should only be performed if fecal calprotectin” is >250 mcg/g.
My take: Clinical remission in ulcerative colitis should be verified. It is reasonable to start with a fecal calprotectin and if elevated to proceed with endoscopic evaluation (colonoscopy or sigmoidoscopy).
Also: new therapy for Crohn’s disease with favorable phase III study. From Pharmacy Times: Risankizumab (Skyrizi) Demonstrates Significant Improvements In Patients with Crohn Disease Two studies, ADVANCE and MOTIVATE showed similar results for Crohn’s disease. In the ADVANCE study: “40% of patients receiving 600 mg, and 32% of patients receiving 1200 mg achieved endoscopic response at week 12, compared to 12% in the placebo group.” In the MOTIVATE study, “29% and 34% of patients receiving 600 mg and 1200 mg achieved endoscopic response, respectively, compared to 11% in the placebo group.”
Outcomes of VEO-IBD. B Kerur et al. Inflamm Bowel Dis 2021; 27: 295-302.Bowel Disease in North America: A Retrospective Cohort Study The study population included 269 children (105 [39%] Crohn’s disease, 106 [39%] ulcerative colitis, and 58 [22%] IBD unclassified). Key findings:
By the end of follow-up, stricturing/penetrating occurred in 7 (6.6%) children.
Median age at diagnosis was 4.2 years. 71 (26%) were ❤ yrs.
Only 5 (1.7%) had a coexisting immunological disorder.
Over 5 years, cumulative use of an immunomodulator and biologic was 61% and 41% respectively. Exclusive enteral nutrition was used in 10 children (4%).
11.5% (n=19) had a change in diagnosis from UC/IBD-U to Crohn’s disease
The risk of any bowel surgery in Crohn’s disease was 3% by 1 year, 12% by 3 years, and 15% by 5 years and did not differ by age at diagnosis.
The risk of colectomy in ulcerative colitis/IBD unclassified was 0% by 1 year, 3% by 3 years, and 14% by 5 years and did not differ by age of diagnosis.
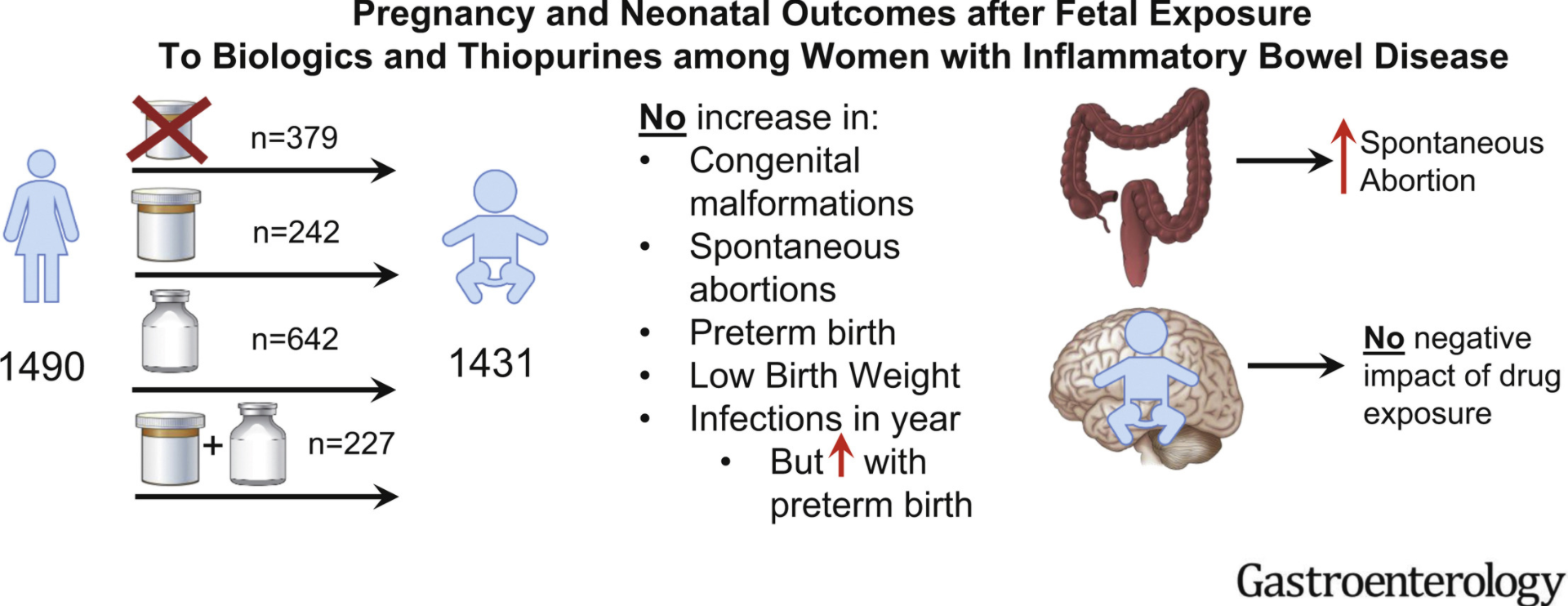
In this PIANO study (2007-2019), pregnant women with IBD were enrolled in a prospective, observational, multicenter study across the United States. PIANO is an acronym for Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes.
Exposure was to thiopurines (n = 242), biologics (n = 642), or both (n = 227) vs unexposed (n = 379).
In this study, which analyzed Medicaid Analytic eXtract data from 4 states (California, Georgia, North Carolina, and Texas) between 2006 and 2011, the authors identified 14,735 patients with IBD (4672 black [32%]). Key finding: “In patients with Medicaid insurance, where access to IBD-specific therapy should be similar for all individuals, there was no significant disparity by race in the utilization of IBD-specific therapies.”
This was a retrospective cohort study which included 169 patients who never smoked actively, 91 patients (54%) were exposed to passive smoking.
Key finding:
Exposed patients were more likely to undergo intestinal surgery than nonexposed patients (67% vs 30%; P < 0.001). Multivariate Cox regression analysis revealed that passive smoking was an independent risk factor for intestinal surgeries (hazard ratio, 1.7; 95% CI, 1.04–2.9; P = 0.034)
Smoking has long been identified as one of the strongest environmental risk factors for both the development of Crohn disease (CD) and the worsening of the disease course.
Studies in smokers with CD have reported that the risk of flares and complications matches that of nonsmokers with CD after 1 year of abstinence.
It would be reasonable to expect that a similar risk reduction exists for patients who can become passive-smoke-free. In addition, their likelihood of remaining smoke-free themselves is increased if they live in a smoke-free household.
My take (from editorial): “Clinicians should consider widening the scope of smoking cessation counseling to include not just patients but also their cohabitants.”
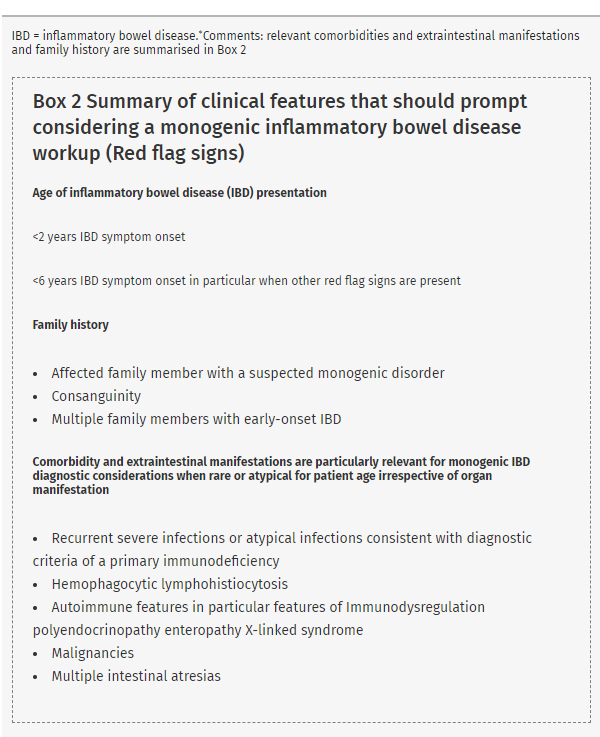
This is a very useful article. Table 3 lists many of the features of some monogenic inflammatory bowel disease (IBD). Table 4 details potential immune workup tests. Table 5 lists 75 genes that should be included when testing for monogenic IBD.
Box 2 (see below) provides a list of conditions that should prompt consideration of genetic testing. Figure 1 provides an algorithm for testing.
Table 6 provides a summary of statements
#3:”Genetic screening for monogenic IBD is recommended in all patients with infantile-onset IBD (<2 years) and should be considered in patients with very early-onset IBD (<6 years), in particular, in those patients with relevant comorbidity, extraintestinal manifestations, and/or family history”
#5: “Routine genetic screening for all IBD patients is not recommended since a monogenic cause of IBD in patients with IBD onset over 6 year of age, especially those with adolescent or adult age onset of IBD is exceptional in the absence of relevant comorbidity”
There is also some advice on variants of unknown significance: “Databases, such as Clinvar, ClinGen, or The Human Gene Mutation Database can help to assess variant phenotype relations”
In patients receiving anti-TNF agents which are usually effective for CRMO, CRMO may develop paradoxically and may be associated with a psoriaform reaction.
At the time of diagnosis of paradoxical reaction, all patients were in remission due to anti-TNFα efficiency. Trough levels of anti-TNFα were in the expected range, and there were no anti–anti-TNFα antibodies.
All patients recovered after discontinuation of infliximab (n = 2) or adalimumab (n = 1).
My take: This study describes a rare adverse effect of anti-TNFα agents. If CRMO develops while on one of these agents, an alternative treatment is needed.
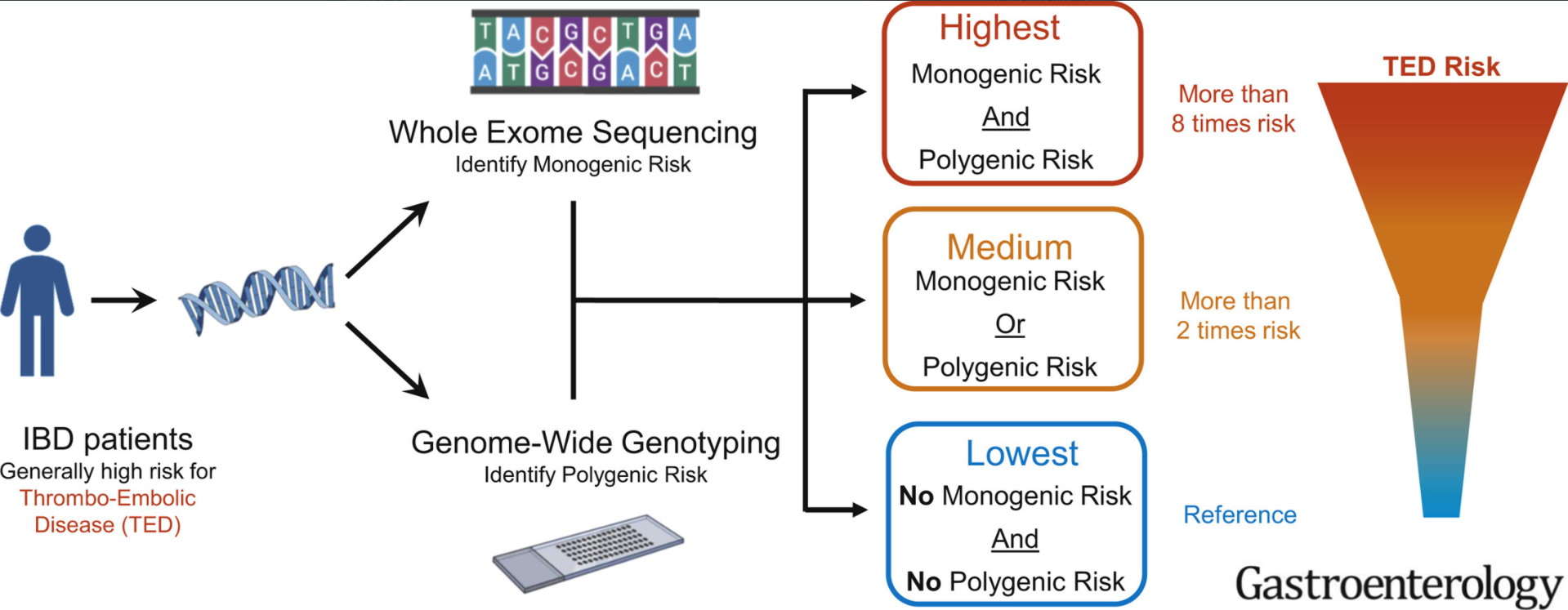
Background: 10% of healthy subjects are genetically at high risk for thromboembolic disease (TED). For adults with inflammatory bowel disease, TED is “largest cause of mortality in patients”
Key findings:
In total, this retrospective study had 792 IBD patients who had both whole-exome sequencing and genotyping data to identify thrombophilia pathogenic variants. 122 of 792 IBD patients (15.4%) as genetically high risk for TED.
Genetic TED risk was significantly associated with increased TED event (odds ratio,2.5; P ¼ .0036).
Patients with high TED genetic risk more frequently had thrombosis at multiple sites (78% vs 42%, odds ratio, 3.96; P ¼ .048)
“Our analyses demonstrate that approximately 1 in 7 patients with IBD have odds 2.5 times higher than nongenetically high-risk patients with IBD for experiencing TED.” The risk of TED in IBD is generally 3- to 4-fold higher than the general population
My take: In children, the risk of clots is much lower than in adults. Thus, the potential to identify those at highest risk would be useful in order to target interventions. Also, patients at higher risk for TED may affect choice of treatment (eg. avoiding JAK inhibitors).
In patients with Crohn’s disease, dose escalation of biologic therapy (eg. anti-TNF agents, vedolizumab) has been shown to be helpful in recapturing response to treatment. In a retrospective study with 110 patients, Ollech et al explore the outcomes in those who had their subcutaneous ustekinumab interval shortened to 4 weeks (from every 8 weeks).
Key findings:
Following dose interval shortening, the patients’ median Harvey Bradshaw Index (HBI) decreased from 4.5 to 3 ( P = .002), the median level of CRP decreased from 8 mg/L to 3 mg/L ( P = .031), and median level of fecal calprotectin decreased from 378 μg/g to 157 μg/g ( P = .57).
Among patients with active disease (HBI >4, CRP ≥/=5mg/dL, fecal calprotectin >250ug/g, or endoscopic evidence for disease activity), dose interval shortening was associated with a 28% clinical remission (an HBI score ≤4), and 50% had reduced levels of fecal calprotectin; 36% achieved endoscopic remission.
The authors did not identify serious adverse events with dose shortening.
My take: Prospective studies are needed. This study indicates that more frequent dosing improves outcomes in a significant fraction of those with active disease.
Unrelated article: C-H Lo et al. Clin Gastroenterol Hepatol 2021; 19: 87-95. Healthy Lifestyle Is Associated With Reduced Mortality in Patients With Inflammatory Bowel Diseases In this study, using data from three large cohort studies, the authors assessed the impact of 5 healthy lifestyle factors: never smoking, body mass index 18.5–24.9 kg/m 2, vigorous physical activity in the highest 50% with non-zero value, alternate Mediterranean diet score ≥4, and light drinking [0.1–5.0 g/d]. Key finding:
Compared to patients with IBD with no healthy lifestyle factors, patients with IBD with 3–5 healthy lifestyle factors had a significant reduction in all-cause mortality (hazard ratio [HR], 0.29; 95% CI, 0.16–0.52; Ptrend < .0001).
My take: Like the general population, healthy lifestyle choices are important in individuals with IBD; this study provides some data on the effects on outcomes.
“The U.S. Food and Drug Administration (FDA) is alerting the public that preliminary results from a safety clinical trial show an increased risk of serious heart-related problems and cancer with the arthritis and ulcerative colitis medicine Xeljanz, Xeljanz XR (tofacitinib) compared to another type of medicine called tumor necrosis factor (TNF) inhibitors. FDA required the safety trial, which also investigated other potential risks including blood clots in the lungs and death. Those final results are not yet available….
Patients should not stop taking tofacitinib without first consulting with your health care professionals, as doing so may worsen your condition. Talk to your health care professionals if you have any questions or concerns.”
In this retrospective observational longitudinal cohort study with 3007 patients with IBD from the ImproveCareNow Network, the authors found a high rate of continued linear growth after expected growth plate closure (15 years in females, 17 years in males).
Key findings:
80% manifested continued growth beyond the time of expected growth plate closure, more commonly in CD (81%) than UC (75%; P = 0.0002)
Median height gain was greater in males with CD (1.6 cm) than in males with UC (1.3 cm; P = 0.0004), and in females with CD (1.8 cm) than in females with UC (1.5 cm; P = 0.025)
My take: This study provides additional information about delayed skeletal maturation in the pediatric population with inflammatory bowel disease. Interestingly, the rate of continued growth with ulcerative colitis was nearly as high as with Crohn’s disease.











{kind=link}