HH Uhilg et al. JPGN 2021; 72: 45-473. Free Full Text: Clinical Genomics for the Diagnosis of Monogenic Forms of Inflammatory Bowel Disease: A Position Paper From the Paediatric IBD Porto Group of European Society of Paediatric Gastroenterology, Hepatology and Nutrition
- This is a very useful article. Table 3 lists many of the features of some monogenic inflammatory bowel disease (IBD). Table 4 details potential immune workup tests. Table 5 lists 75 genes that should be included when testing for monogenic IBD.
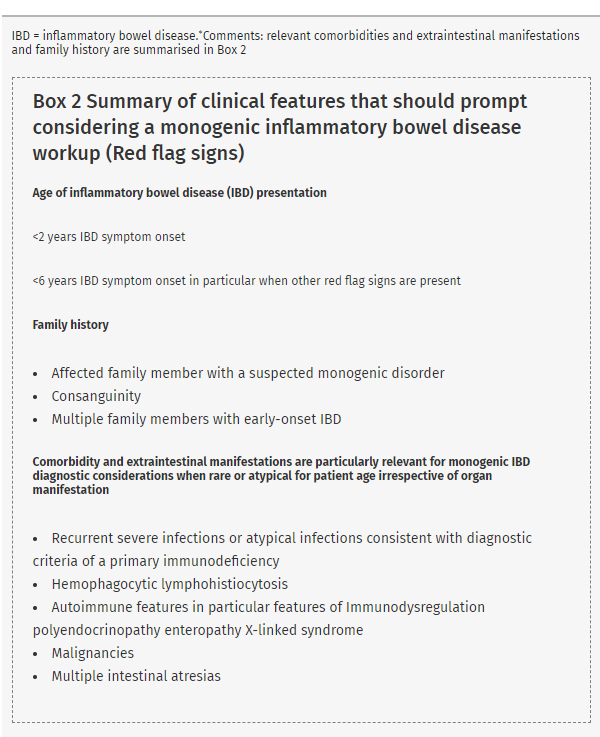
- Box 2 (see below) provides a list of conditions that should prompt consideration of genetic testing. Figure 1 provides an algorithm for testing.
- Table 6 provides a summary of statements
- #3:”Genetic screening for monogenic IBD is recommended in all patients with infantile-onset IBD (<2 years) and should be considered in patients with very early-onset IBD (<6 years), in particular, in those patients with relevant comorbidity, extraintestinal manifestations, and/or family history”
- #5: “Routine genetic screening for all IBD patients is not recommended since a monogenic cause of IBD in patients with IBD onset over 6 year of age, especially those with adolescent or adult age onset of IBD is exceptional in the absence of relevant comorbidity”
- There is also some advice on variants of unknown significance: “Databases, such as Clinvar, ClinGen, or The Human Gene Mutation Database can help to assess variant phenotype relations”
Related blog posts:
- VEO-IBD -Useful “Position” Paper Is Really A Review
- Patterns and Puzzles with VEO-IBD This is a very good review and the image on this day has one of my favorite patient t-shirts.
- In Case You Missed It: IBD Year in Review (Eric Benchimol) (2020)
- How Very Early Onset-Inflammatory Bowel Disease is Different, Plus One
- More IBD Cases Than Ever in Young Canadian Children | gutsandgrowth
- Expanding VEO Variants
- Why the Genetics of Inflammatory Bowel Diseases Matter Now
- IBD and Immune-Mediated Diseases | gutsandgrowth
- More IBD Cases Than Ever in Young Canadian Children | gutsandgrowth
- IBD Shorts: September 2019 NCF4 defects
- Just the Beginning: Mutations in Very Early Onset … – gutsandgrowth
- Exome Sequencing in VEO-IBD: More Data | gutsandgrowth
From The Onion: