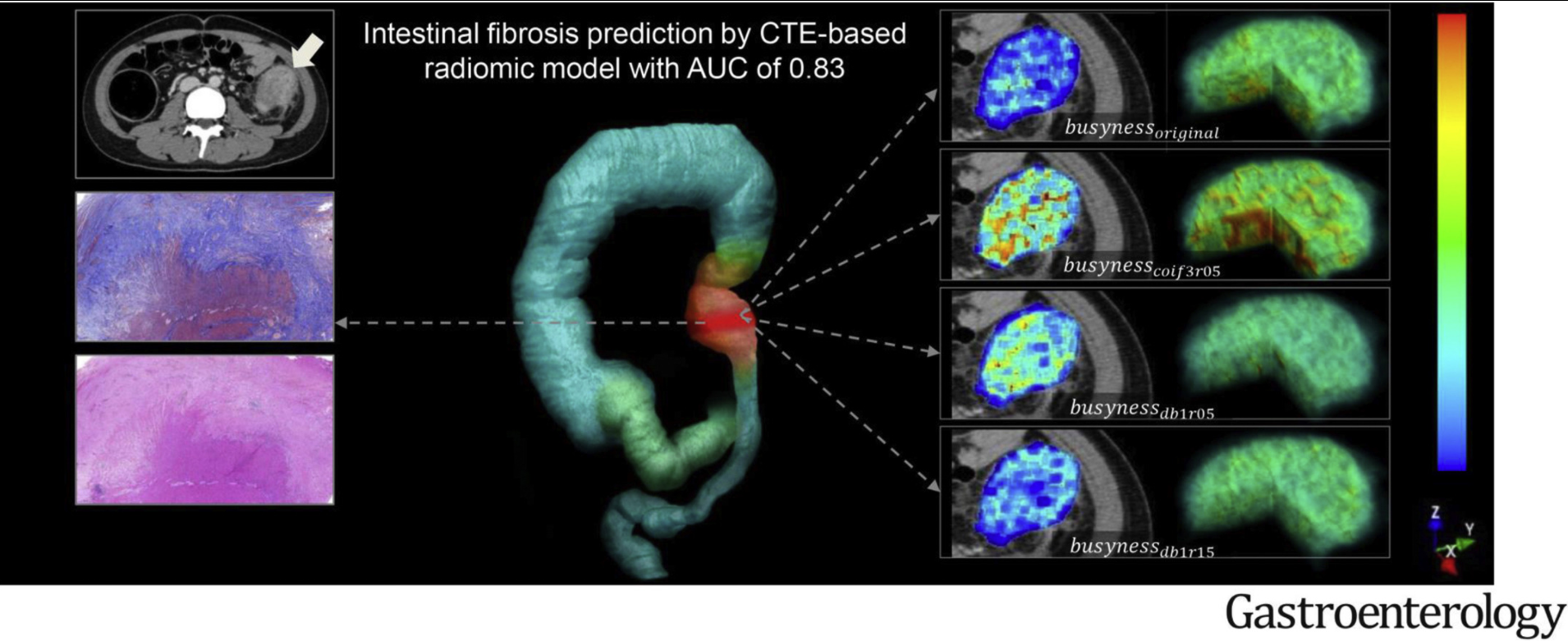
X Li et al. Gastroenterol 2021; 160: 2303-2316. Development and Validation of a Novel Computed-Tomography Enterography Radiomic Approach for Characterization of Intestinal Fibrosis in Crohn’s Disease
Methods: This article describes the development a computed-tomography enterography (CTE)–based radiomic model (RM). This retrospective multicenter study included 167 CD patients who underwent preoperative CTE and bowel resection. 1454 radiomic features were extracted from venous-phase CTE and a machine learning–based RM was developed based on the reproducible features using logistic regression. The RM was validated in an independent external test cohort recruited from 3 centers.
Key findings:
- In the training cohort, the area under the ROC curve (AUC) of RM for distinguishing moderate–severe from none–mild intestinal fibrosis was 0.888.
- In the test cohort, the RM had an AUC of 0.816.
- RM was more accurate than visual interpretations by either radiologist (radiologist 1, AUC = 0.554; radiologist 2, AUC = 0.598; both, P < .001) in the test cohort
My take: This CT approach with RM allowed for accurate characterization of intestinal fibrosis in CD. The images look pretty cool too.