This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Safety in Pediatric IBD Therapy: Is it time to stop using thiopurines?
Jeffrey Hyams Connecticut Children’s Medical Center
Key points from this lecture:
- Dr. Hyams: “There are better options than thiopurines in 2017 due to infrequent but serious risks”
- The DEVEVOP study showed that anti-TNF agents did NOT increase the risk of lymphoma or hemophagocytic lymphohistiocytosis (HLH). In contrast, these risks do occur with thiopurines –this is infrequent but remains significant.
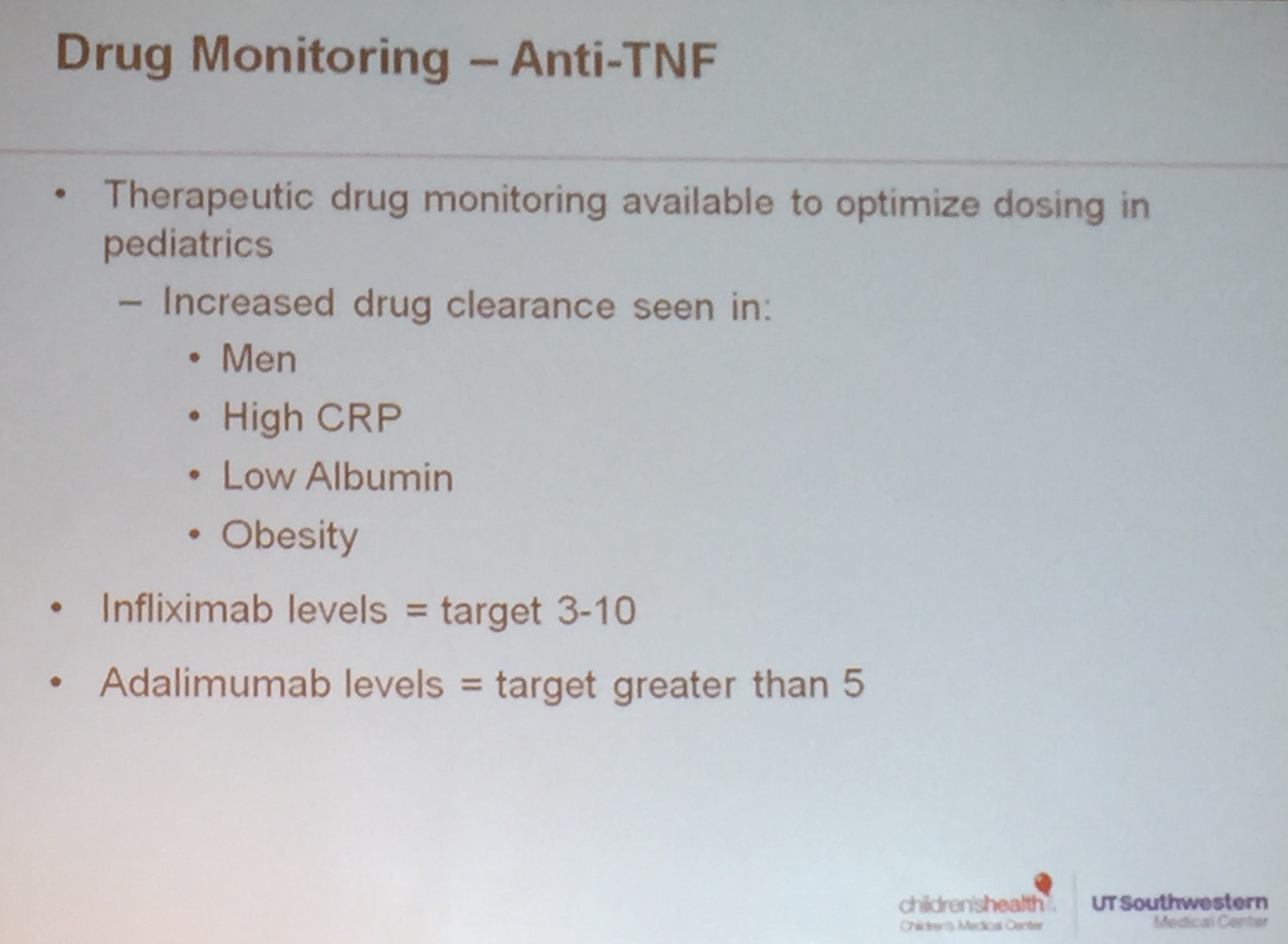
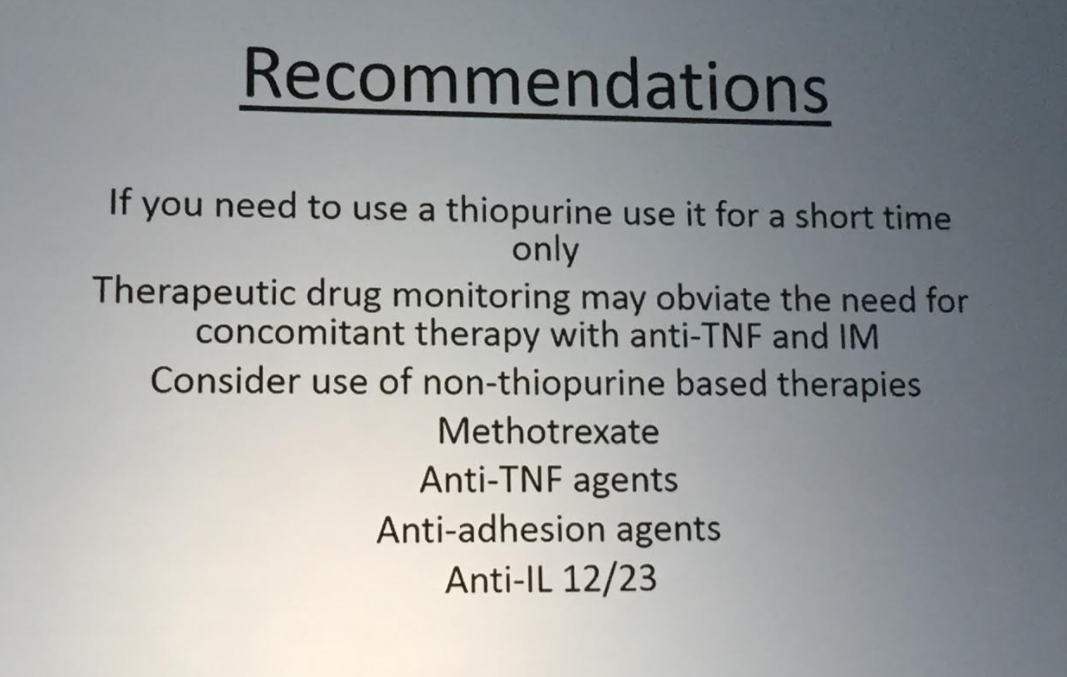
- Therapeutic drug monitoring may obviate the need for combination/dual therapy which has been shown to improve response rates to anti-TNF agents; methotrexate may work for combination therapy and may be safer than thiopurines
- If a thiopurine is used as part of combination therapy, short duration (~6 months) is likely to have low risks
- In addition to Dr. Hyams, Dr. Baldassano, in his discussion of treat to target (discussed in subsequent post), echoed the sentiment that he no longer recommends thiopurine therapy
Dr. Hyams slides list some of the relative risks of thiopurine therapy. To understand these risks, the absolute risk is probably more helpful.
My take: This lecture did not focus on the main benefit of thiopurines which is its use in combination therapy. Many experts consider combination therapy to be the standard of care for adults with Crohn’s disease. The advantages of combination therapy are mainly due to improved durability of anti-TNF therapy and lower antidrug antibodies. How this benefit stacks up against the risks discussed in this lecture and whether this benefit can be supplanted by the use of therapeutic drug monitoring is uncertain.





Related blog posts:
- Develop Study. Good Safety Data on Infliximab
- Three Studies Show Benefit of Concomitant Therapy (Part 1)
- Three Studies Show Benefit of Concomitant Therapy (Part 2)
- Combination therapy with adalimumab –is it helpful?
- ‘Don’t Believe Our Study’
- Should All Pediatric Patients with Crohn’s Disease Continue …
- Don’t be Fooled About Withdrawing Immunomodulator …
- Digging into the COMMIT Study | gutsandgrowth
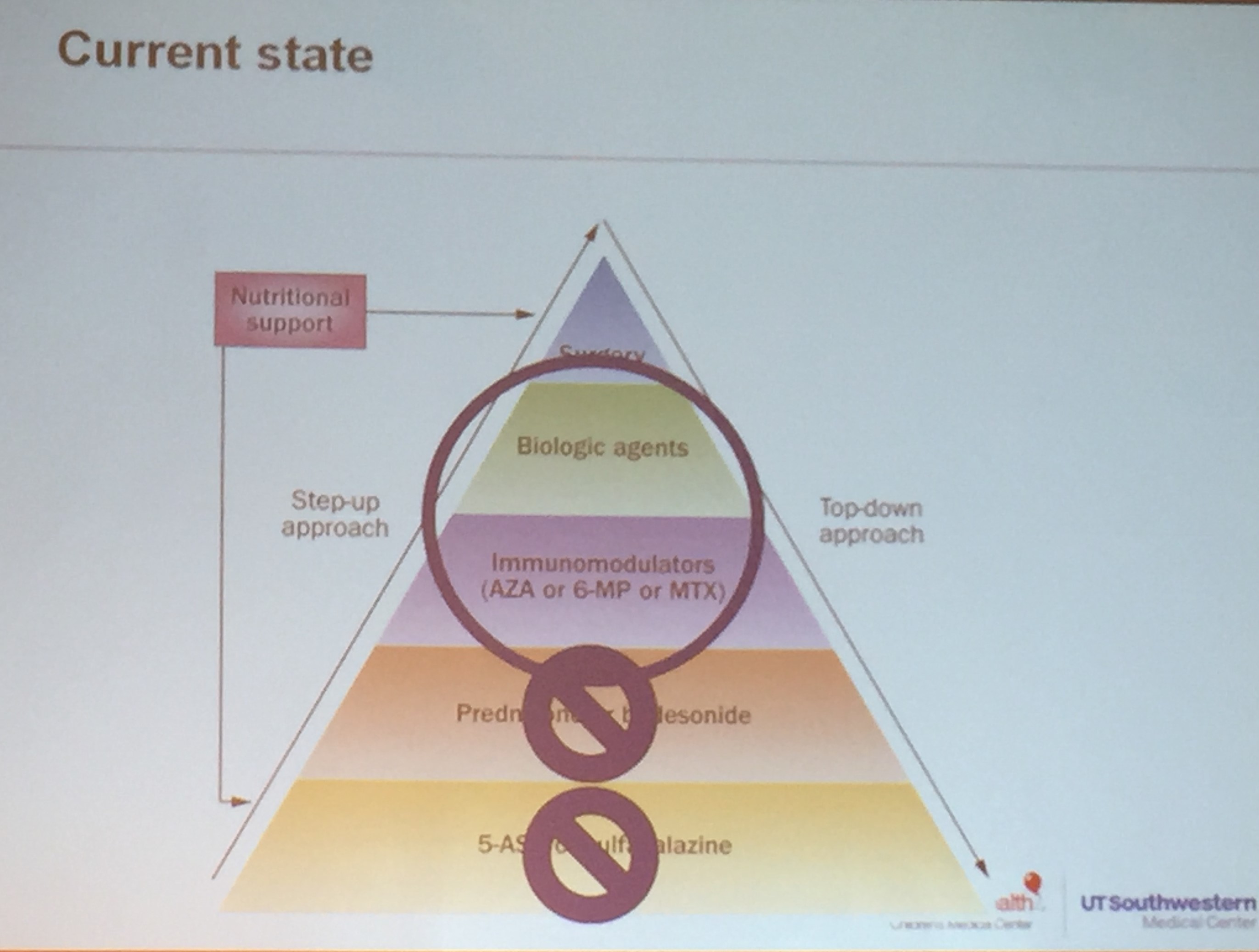
- Support for Step-Up Therapy and Thiopurines | gutsandgrowth
- More NASPGHAN Meeting Notes –Hot Topics
- Anti-TNF agents in Pediatrics have not been shown to cause lymphoma gutsandgrowth
- Don’t forget HLH | gutsandgrowth
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.