More from our recent CCFA Conference. My notes may include some errors in transcription and errors of omission.
Subra Kugasthasan -RISK Updates
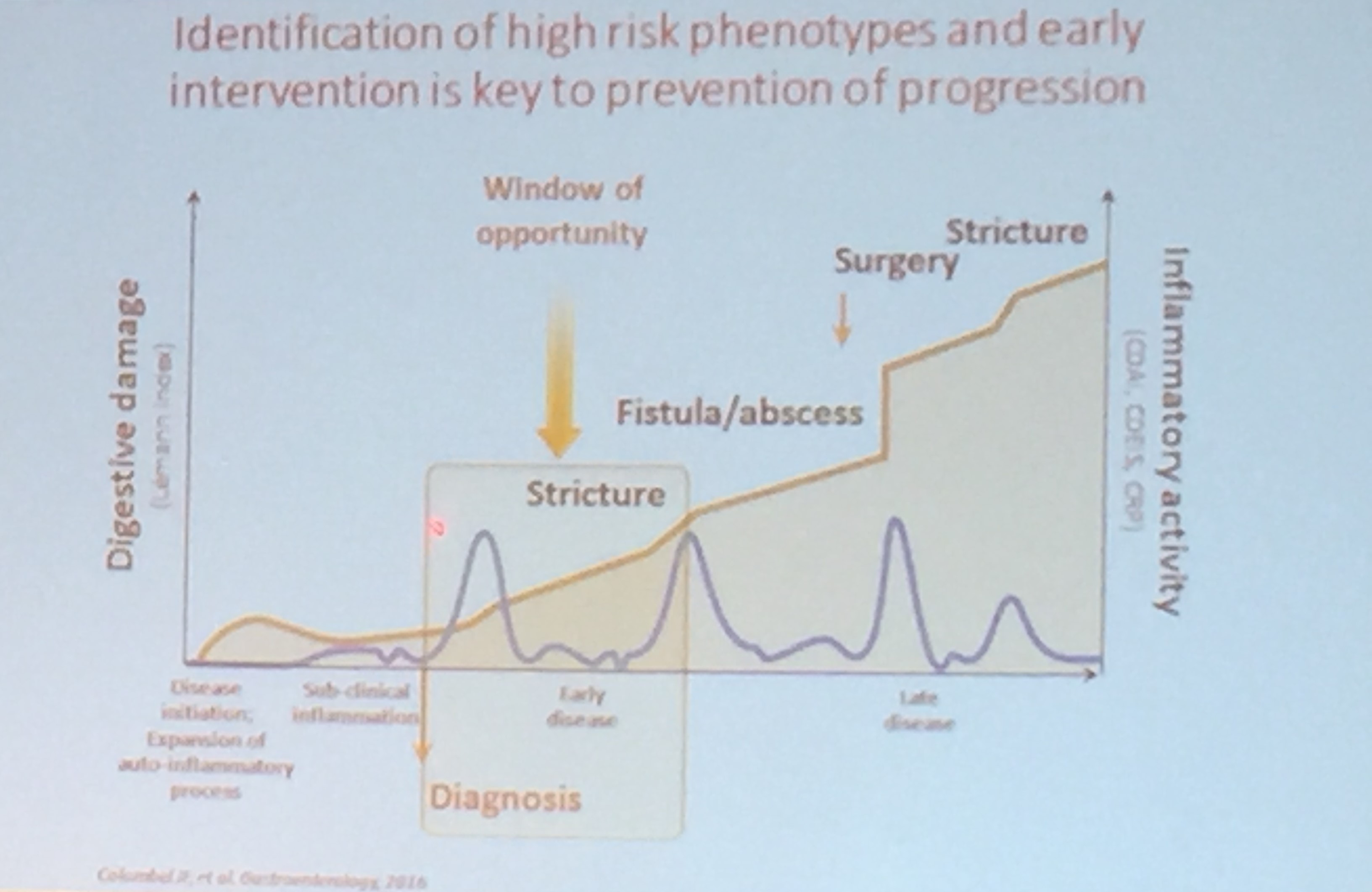
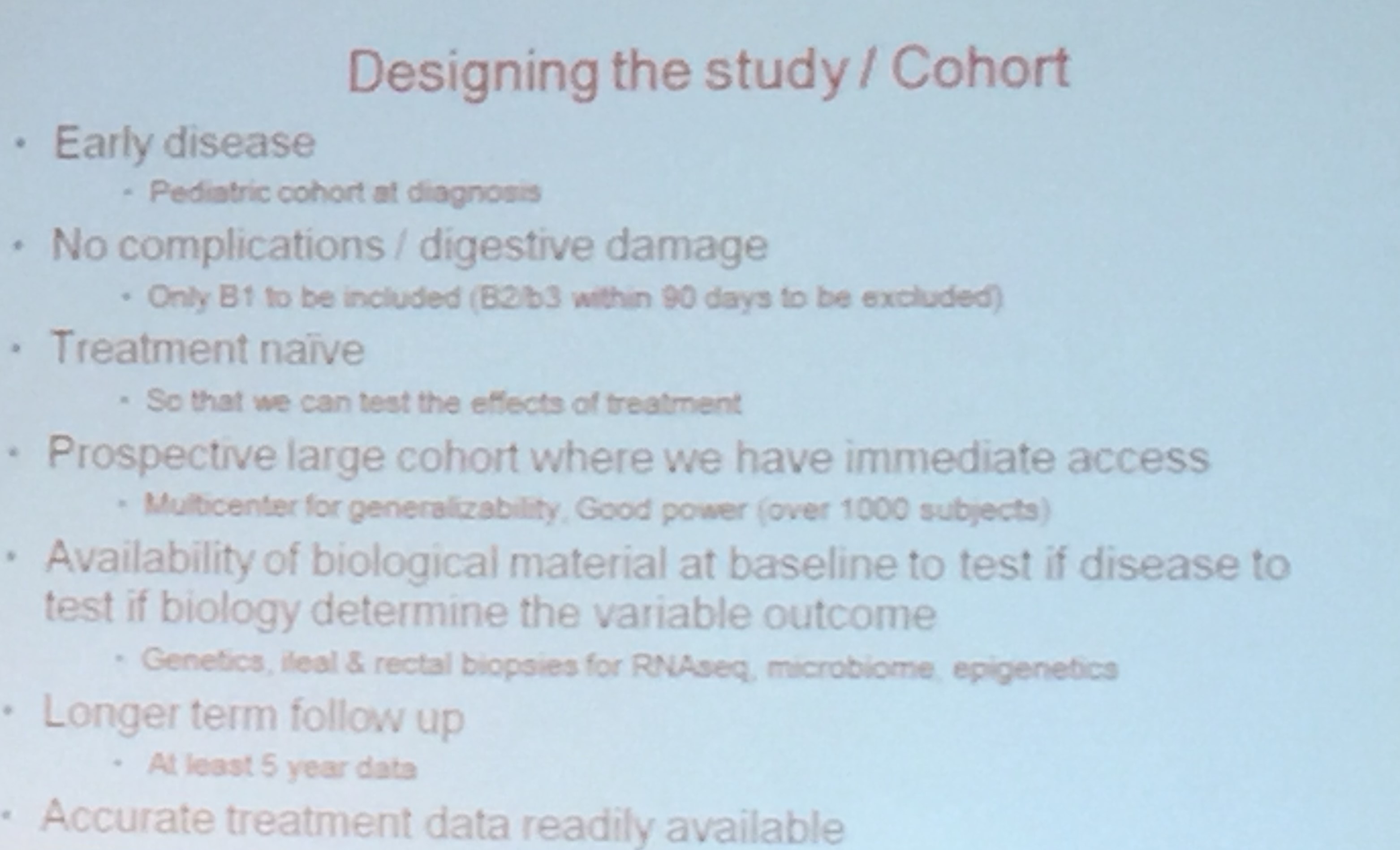
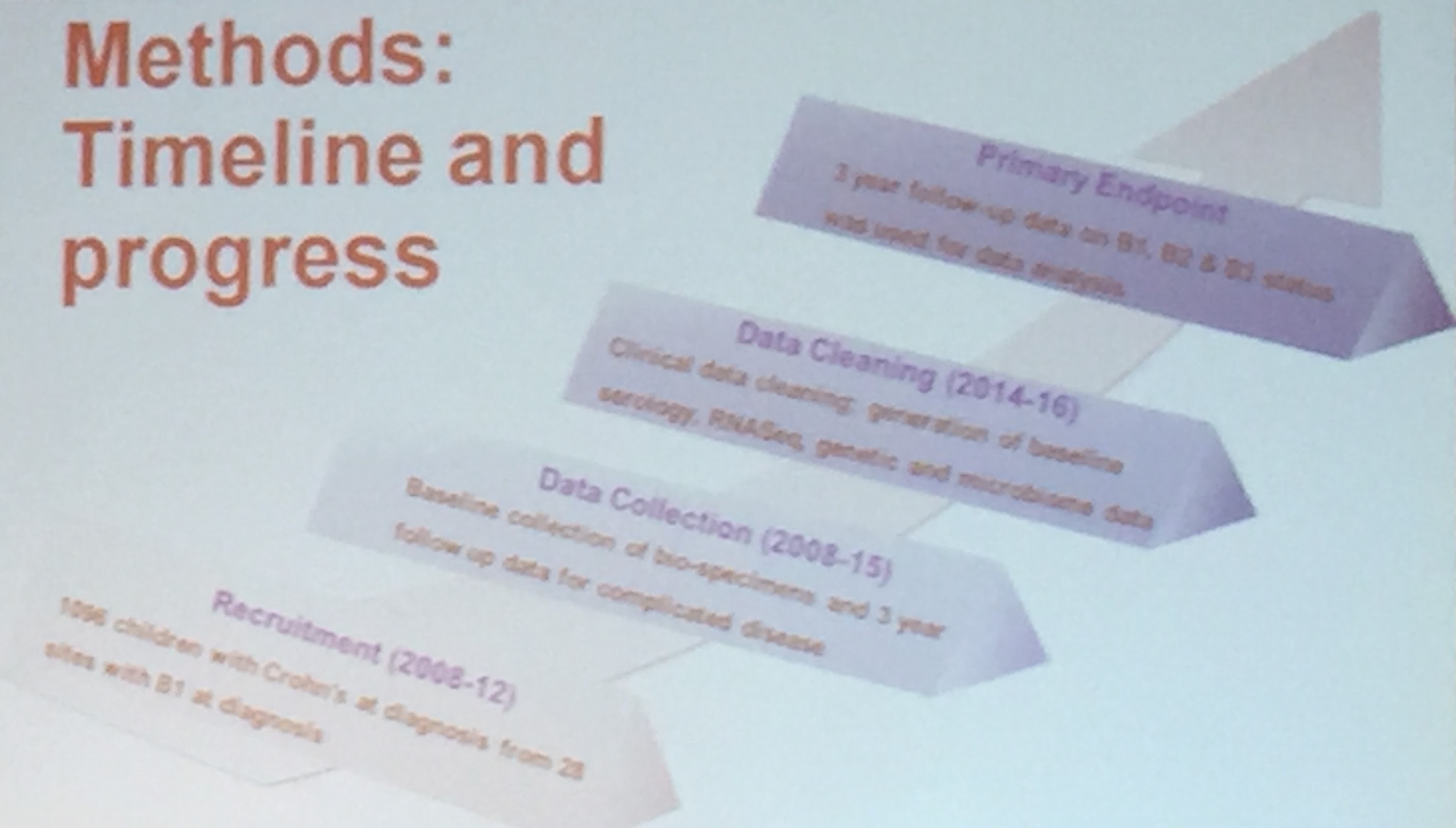
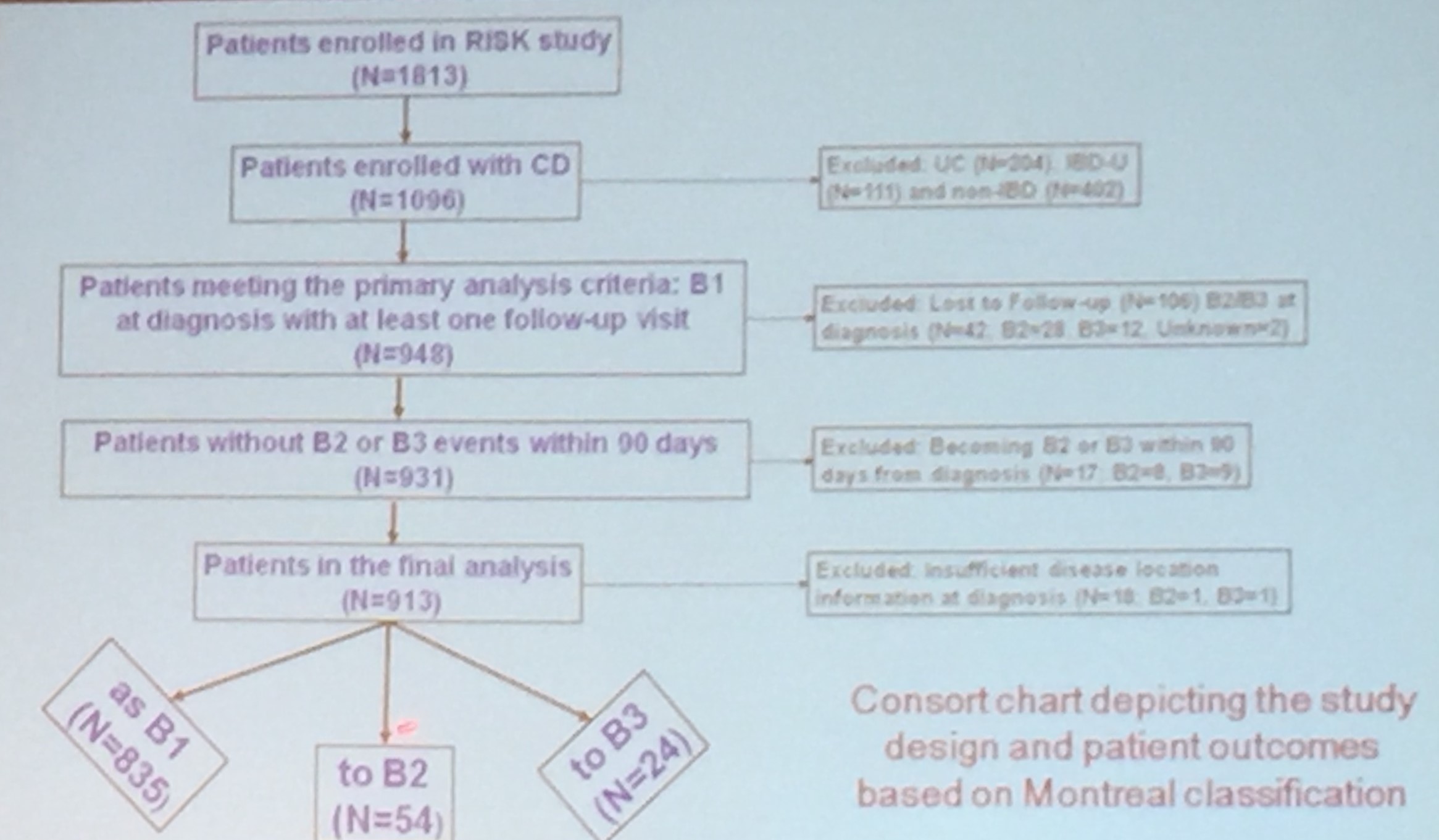
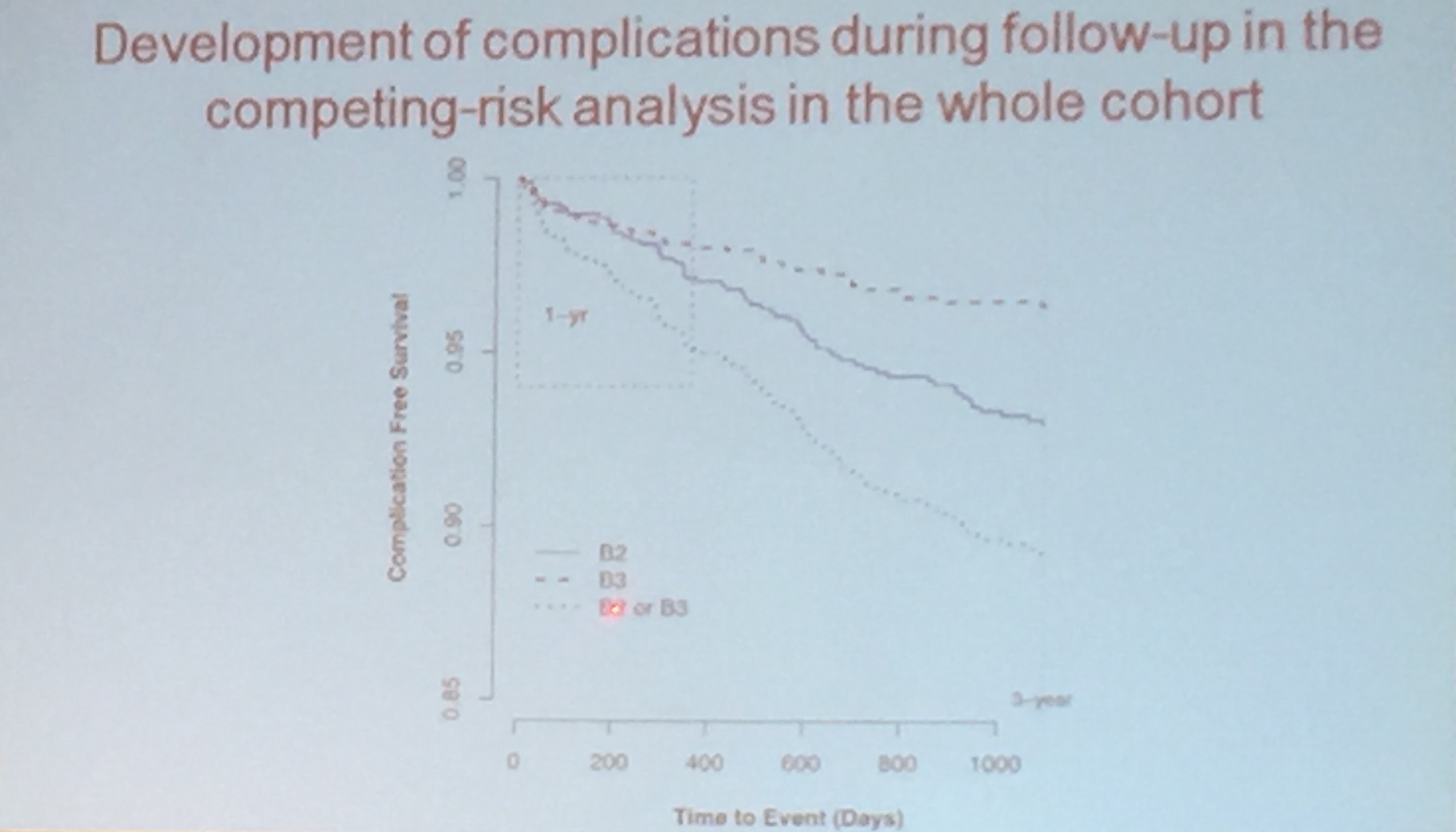
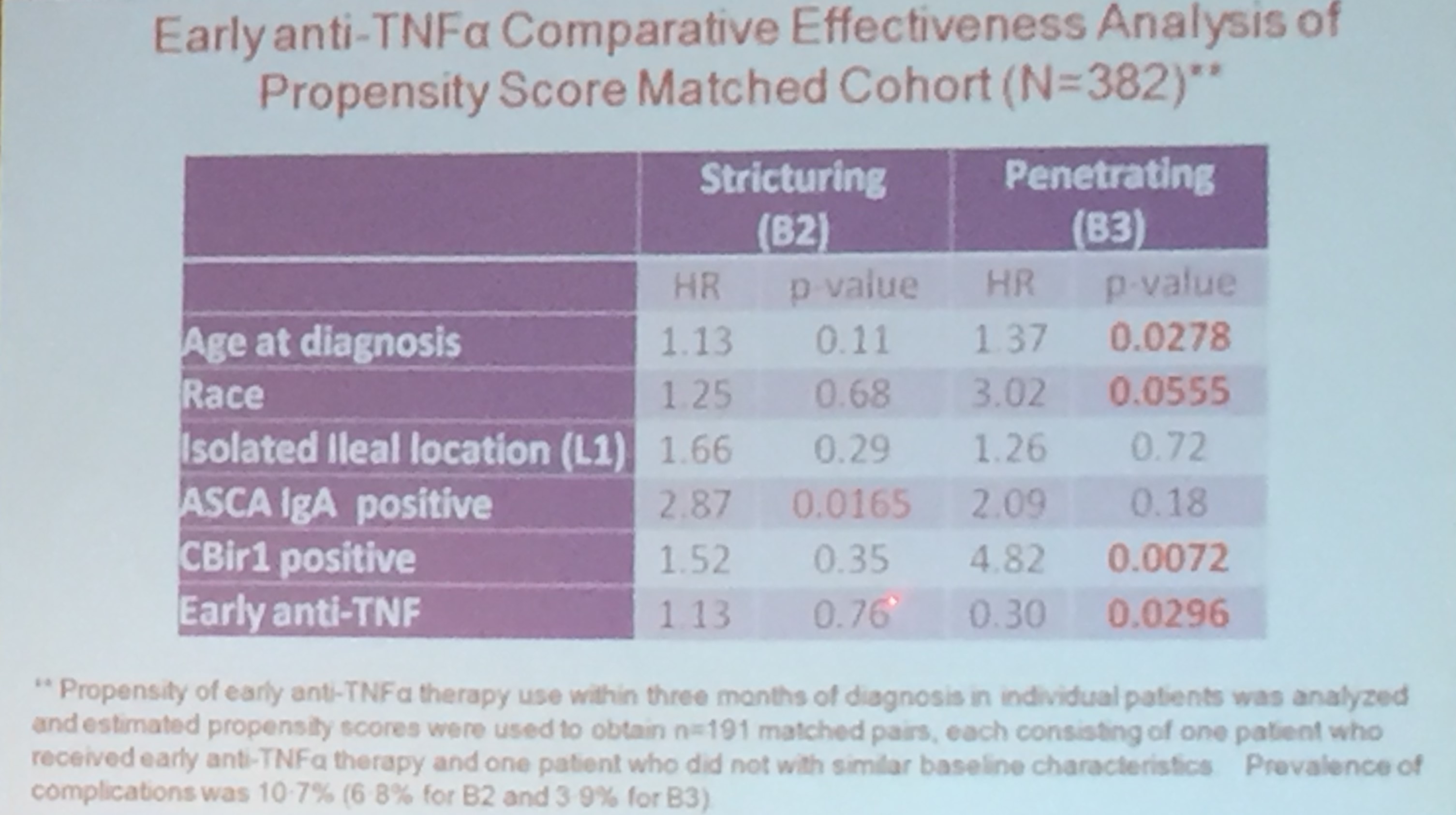
Dr. Kugasthasan’s lecture was excellent. He reviewed the typical clinical course of Crohn’s disease; in most patients, it has a remitting and relapsing course. The goal of the CCFA-sponsored RISK study was to determine how early approaches to treatment affect long-term outcomes. There is likely a window of opportunity to more favorably affect natural history of the disease. In addition, the goal is to determine whether there are predictive markers of severe disease course. This prospective study analyzed 913 patients. In this cohort, 835 remained with B1 (inflammatory) phenotype and 90 developed either B2 (stricturing) phenotype or B3 (penetrating) phenotype.
RISK Study Abstract: Prediction of complicated disease course for children newly diagnosed with Crohn’s disease: a multicentre inception cohort study (S Kugathasan et al. Lancet 2017; 389: 17108. DOI: http://dx.doi.org/10.1016/S0140-6736(17)30317-3)
Key findings:
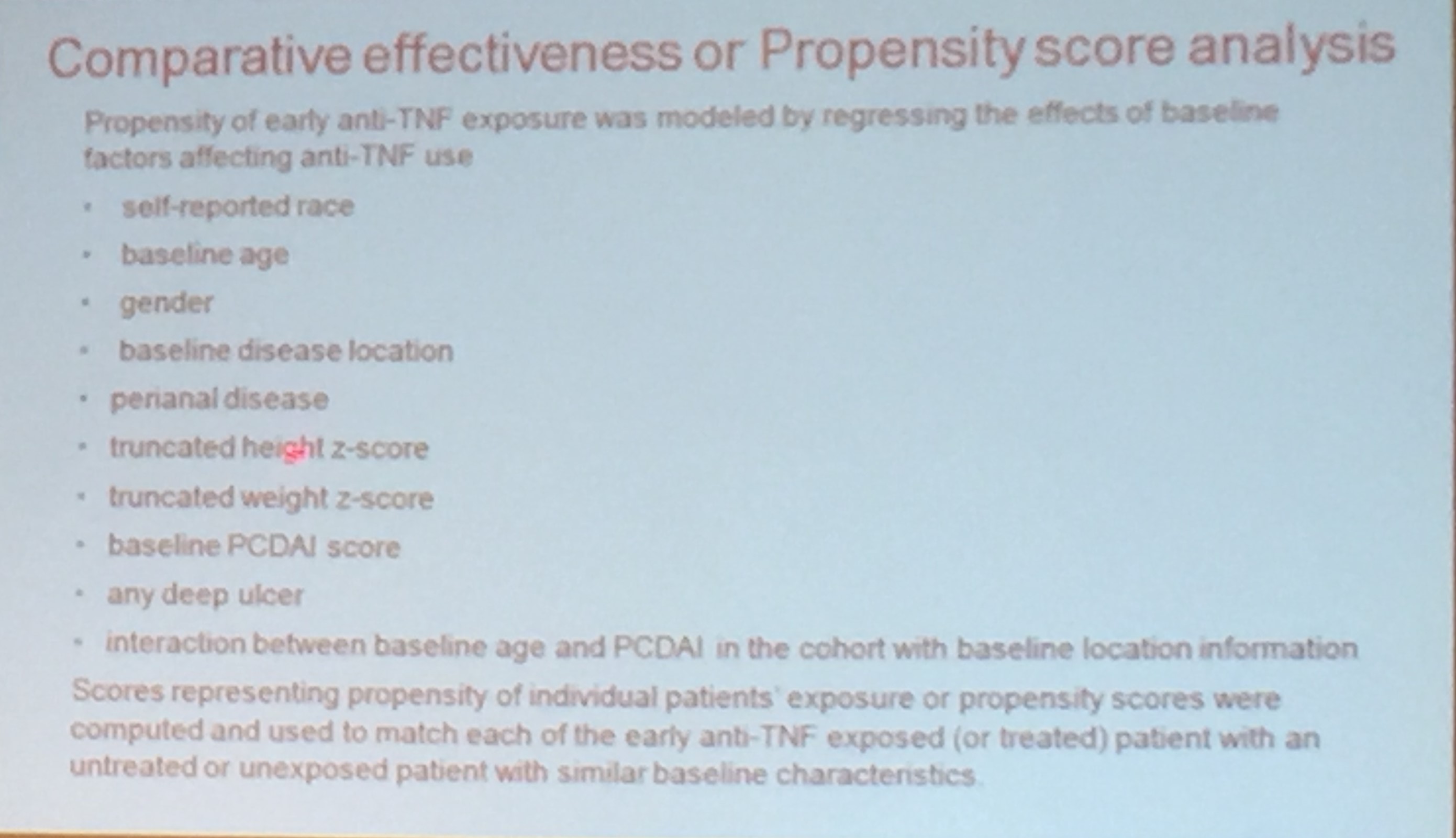
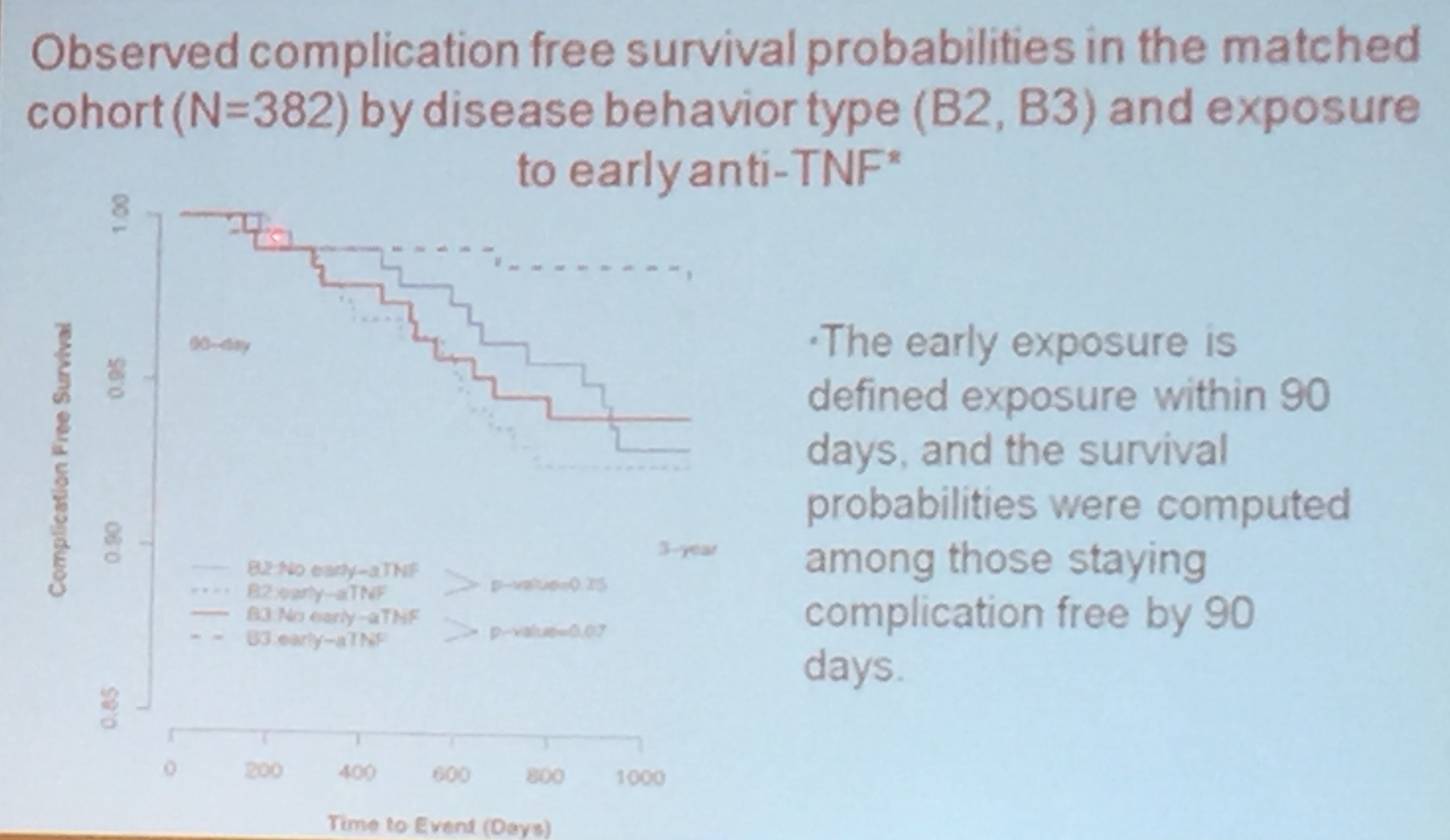
- Early TNF therapy reduced the likelihood of penetrating (B3) but not stricturing (B2) disease
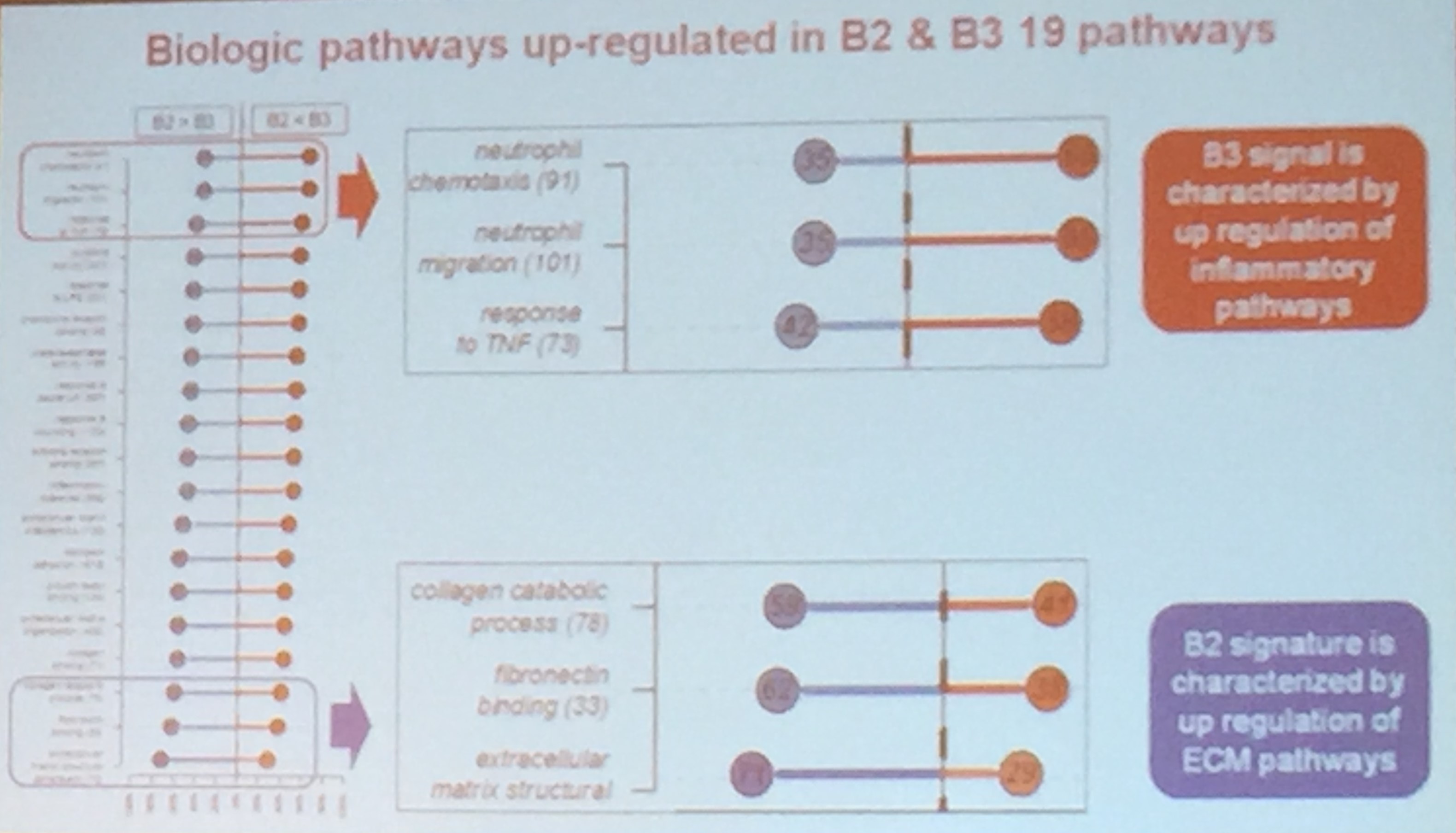
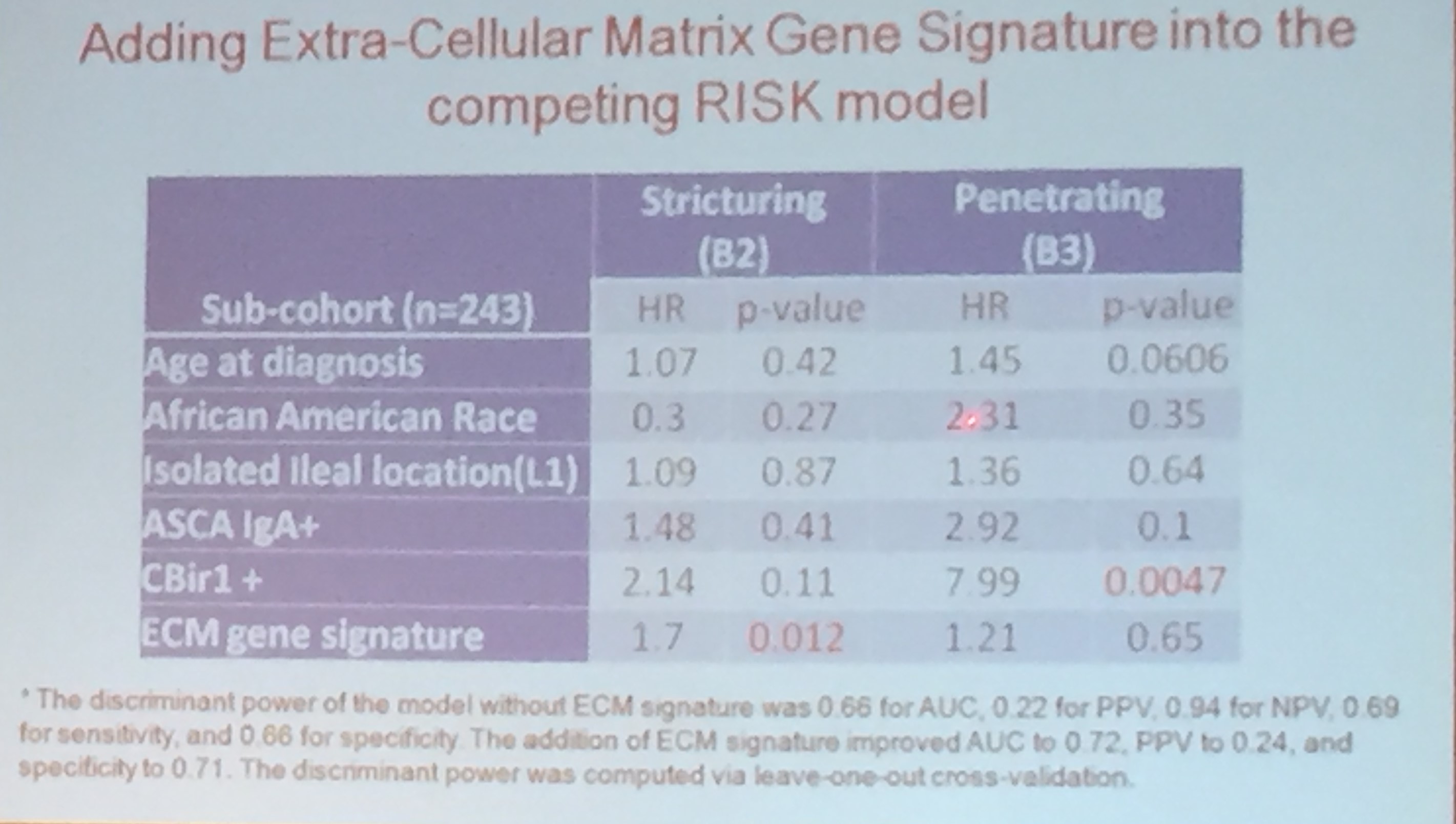
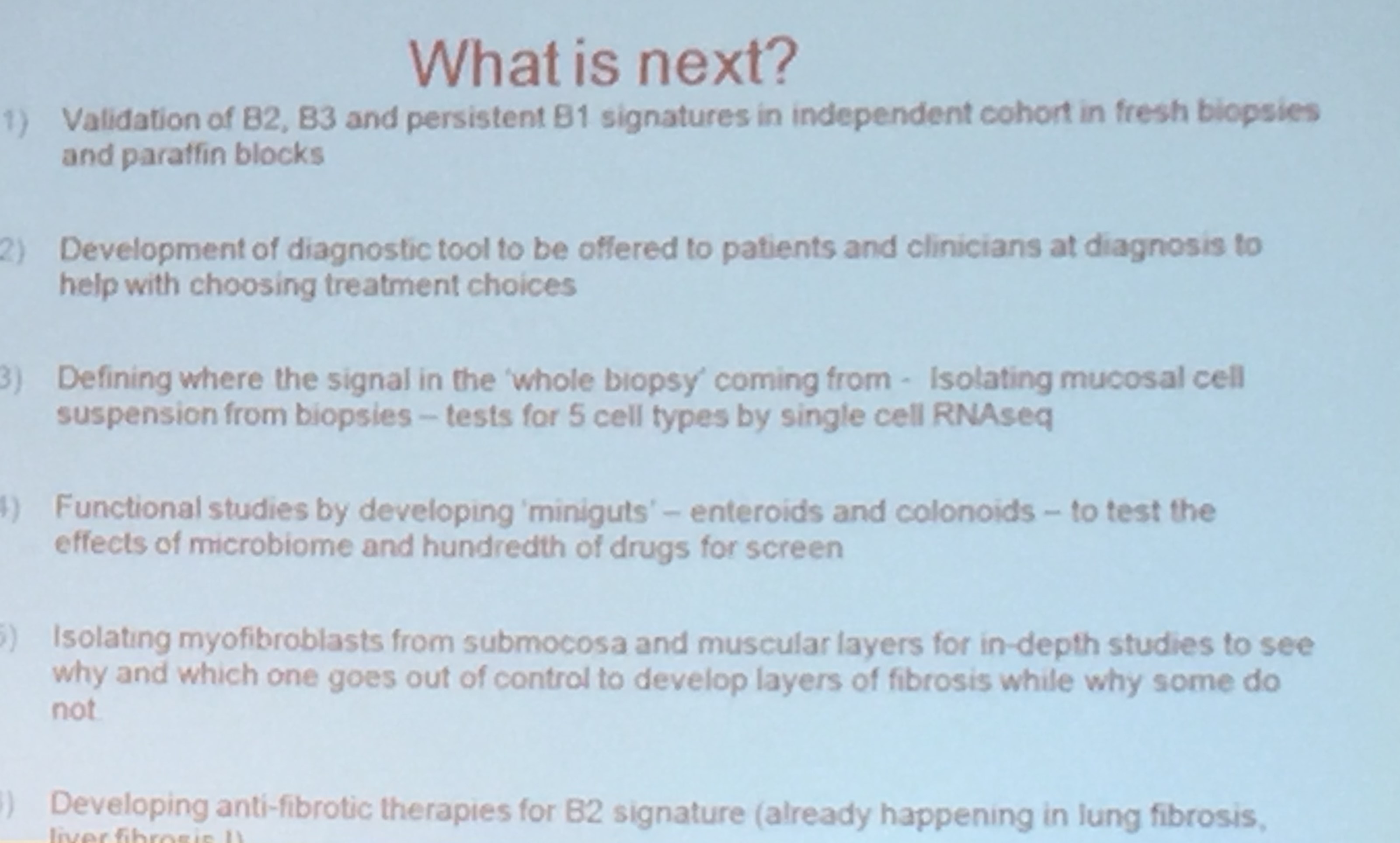
- Based on analysis of genetic expression at baseline, individuals who are likely to develop B2 or B3 disease can be identified. This assay may be available clinically in a few years

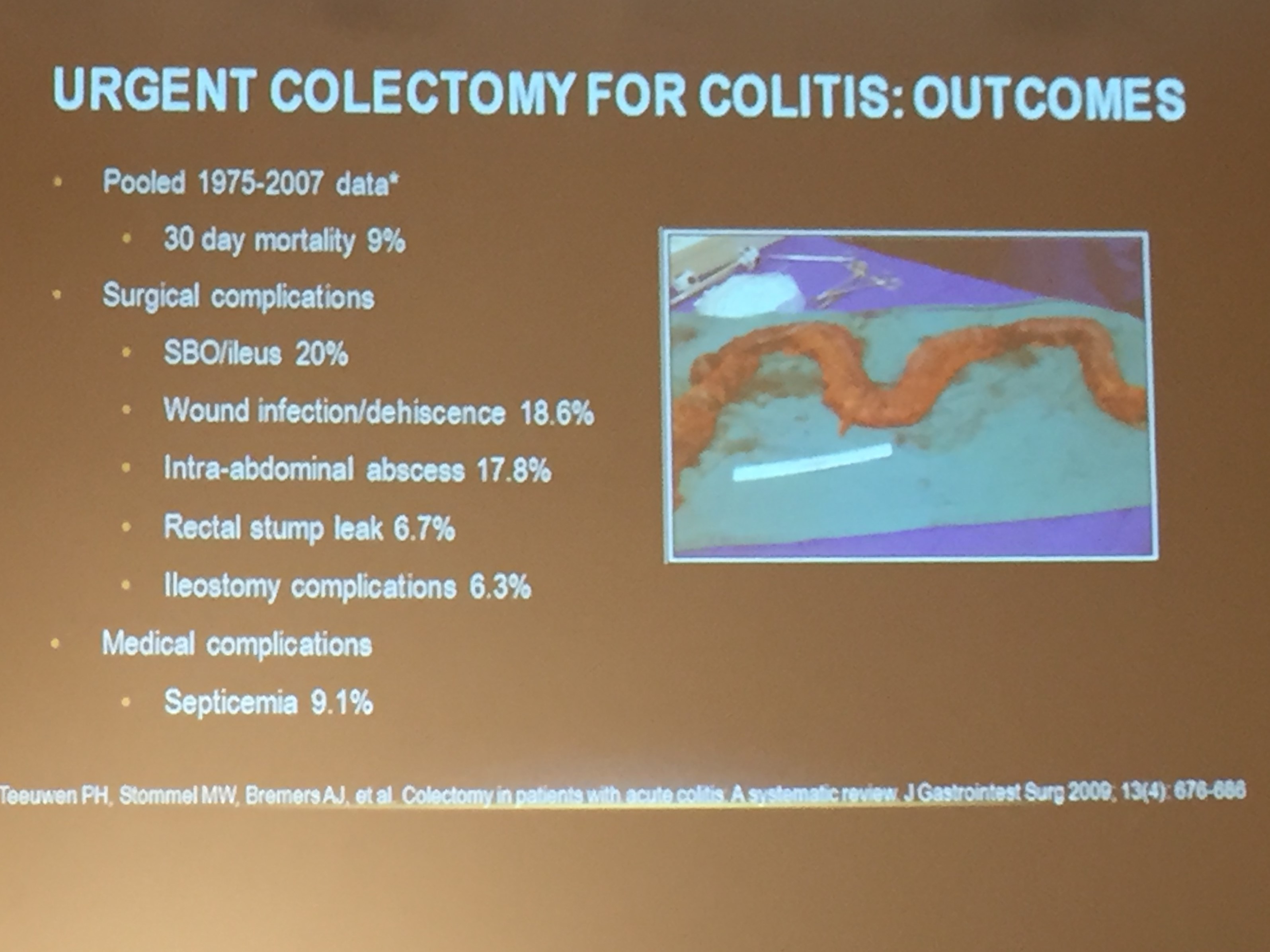
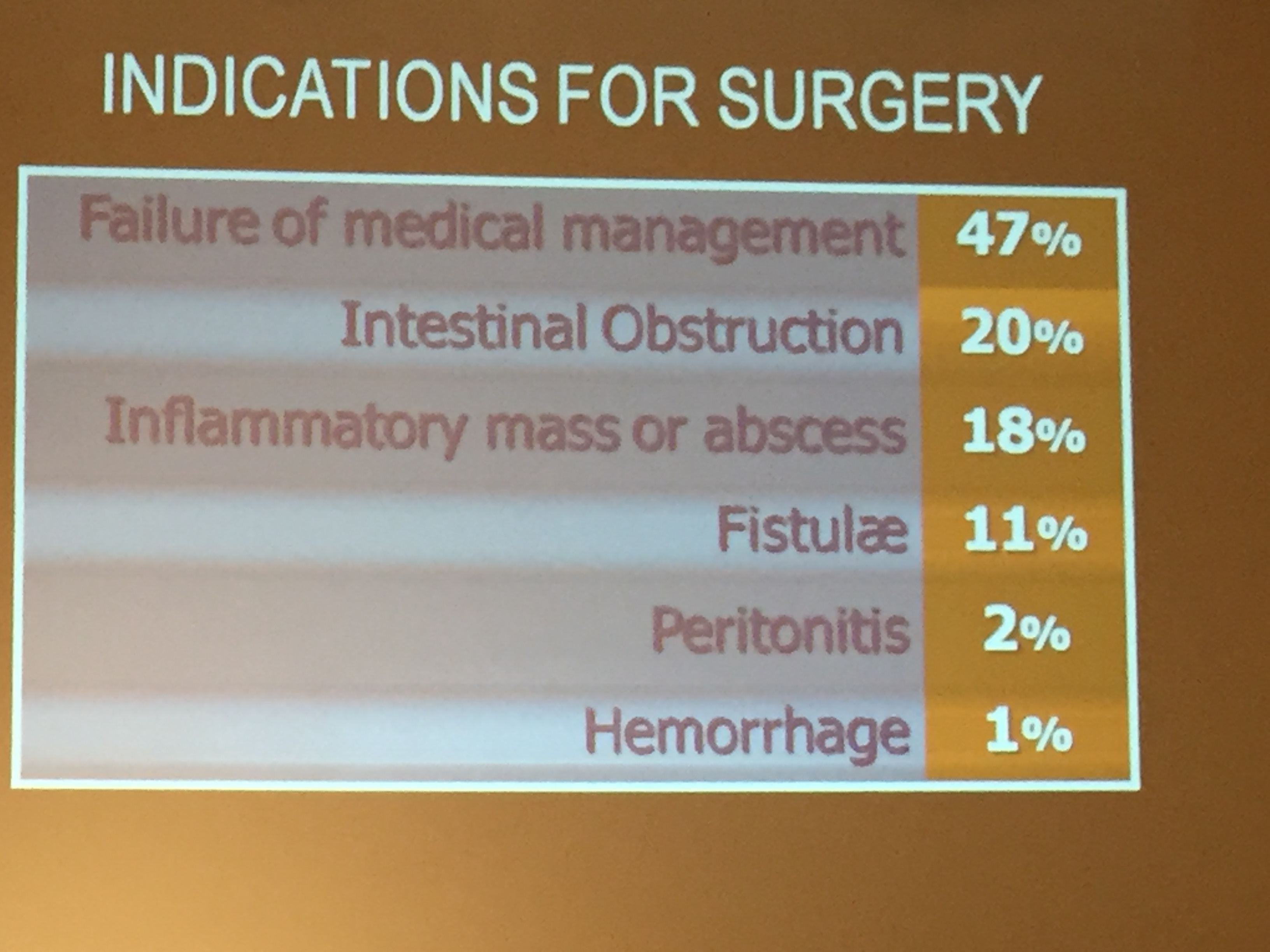
Jahnavi Srinivasan -Multi-Disciplinary Approach to IBD A Surgical Perspective
- Teeuwen PH et al study spans a long period and there have been many changes since that time. The study’s 9% 30-day mortality rate is very high (current Whipple 30-day mortality ~2%)
- 3-stage surgery most common now for ulcerative colitis due to sicker patients who now need operation
- Harder to differentiate UC and CD
- Try to get patients off steroids; this is a key factor in surgical complications. Nutritional support may be helpful though some effects may be mediated by helping with steroid tapering
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) and changes in diet should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.