This great article/commentary is available as open access: Separating Fact from Fiction in the Diagnosis and Management of Food Allergy EM Abrams et al. J Pediatr 2022; 241: 221-228.
Key points:
- “The risk of fatal anaphylaxis is about 1 in 10 million (about equivalent to being struck by lightning)..and fatality on first ingestion of an allergen in infancy has never been described”
- Food allergy causes considerable morbidity/worsens quality of life (QOL): bullying, meal preparation, stress, social activities, and school attendance (with 10% choosing home schooling because of a food allergy). Some of this detriment on QOL is due to fear “that accidental exposure could result in fatal anaphylaxis”
- “The impact of peanut allergy on QoL has been noted to be significantly worse than the impact of other chronic childhood diseases such as rheumatologic disease and type 1 diabetes mellitus”
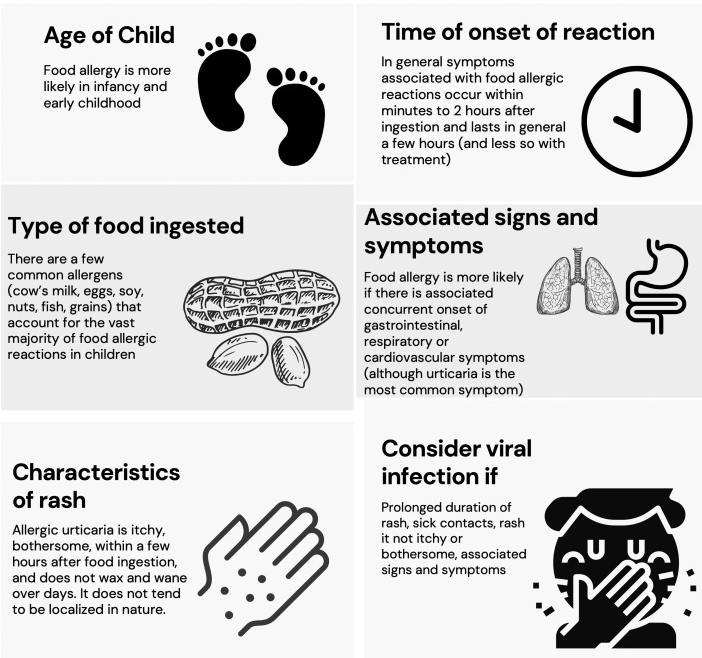
- Uriticaria does not equal allergy. “Although urticaria is commonly equated with a food allergy, food allergy accounts for less than 10% of the causes of all acute urticaria and is not a cause of chronic urticaria.” Urticaria can be triggered by an acute infection (most common etiology)
- “Food proteins are digested within several hours; therefore, urticaria associated with a food ingestion will occur within minutes to 2 hours of ingestion, but typically last no more than a few hours (and less with treatment)” (an exception is meat anaphylaxis owing to galactose-α-1,3-galactose allergy)
- Other common symptoms that are often incorrectly attributed to food allergy include headaches, chronic behavioral symptoms, or chronic nonspecific abdominal pain
- Allergy testing: “the presence of a food-specific IgE is not itself indicative of an allergy…Although both skin prick testing and food-specific IgE testing are highly sensitive (>90% for skin prick tests, 70%-90% for sIgE), the specificity and positive predictive values of testing are often very low. The rate of false-positive tests is up to 40%.”
- Broad “panel testing” (eg, to a panel of “common” foods), or any food allergy diagnostic testing in the absence of a convincing clinical history has high potential to overdiagnose food allergy and result in unnecessary food avoidances
- Don’t do IgG testing. “There is no evidence that IgG testing marks food sensitivity; in fact, the presence of IgG is both expected and is a potential indicator of ongoing tolerance”
- For first-line management anaphylaxis, (intramuscular) epinephrine is the “only life-saving intervention available.” Antihistamines are useful only in the treatment of cutaneous symptoms/urticaria.
- “Although oral corticosteroids are often administered in the setting of anaphylaxis, there is no convincing evidence that their use prevents a biphasic reaction…their routine use is not recommended” (for anaphylaxis)
Related blog posts:
- “The Truth About Allergies and Food Sensitivity Tests”
- Poorly-Conceived Allergy Testing Can Lead to Unnecessary Diet Restrictions and Complications
- Best Allergy Articles 2021 (Part 5): Allergy Test Ordering
- Best Allergy Articles 2021 -Cow’s Milk Allergy (Part 3)
- What’s Wrong with “I Want My Kid Tested For Food Allergies” | gutsandgrowth
- How Allergy Testing Can Lead to More Allergies
- Eczema Rarely Linked to Food Allergy | gutsandgrowth