K Payne et al. JPGN Reports: 2021; August 2021 – Volume 2 – Issue 3 – p e097. Open Access Repeat Biopsy to Assess Duodenal Healing in Children With Celiac Disease and Eosinophilic Gastrointestinal Disorders
Background: “Current standard of care in the management of uncomplicated CD is not to undergo multiple esophagogastroduodenoscopies (EGDs)… In this study, patients with both CD and eosinophilic gastrointestinal disorders (EGID) …) were identified to explore [the mucosal response to a gluten-free diet], as it is standard for patients with EGID to undergo repeat EGDs for disease surveillance.”
Key findings in this retrospective study from CHOP:
- At second biopsy, 44% (17/39) of patients showed no histologic evidence of active CD and 36% (14/39) of patients had negative tTG-IgA values
- 9/15 (60%) of patients with no evidence of CD on biopsy had abnormal tTG-IgA levels
- 8/14 (57%) of patients with normal tTG-IgA levels had evidence of active disease on biopsy
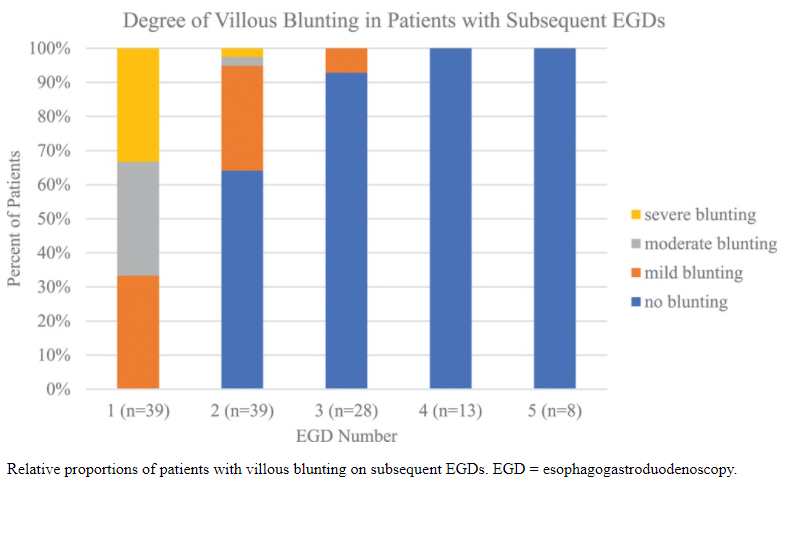
- Among the 18 who had been on a GFD for at least 2 years, 94% (17/18) had normal duodenal biopsies after 2 years, and 83% (15/18) had normal tTG-IgA values after 2 years
- Of the patients with elevated tTG-IgA and normal duodenal biopsies, 66% (6/9) had inflammation elsewhere in the upper gastrointestinal tract, including 4 patients with active EOE and 2 patients with gastritis
My take: This study confirms that tTG-IgA levels are not optimal for monitoring. Current guidelines recognize this and recommend repeat biopsy in patients with persistent or relapsing symptoms even with negative serology
Related blog posts:
- Persistent Villous Atrophy in Celiac Disease Despite a Gluten-Free Diet
- Real-World = Partially-Treated Celiac Disease
- Is a Gluten-Free Diet Possible? DOGGIE BAG Study
- #NASPGHAN19 Postgraduate Course (part 2)
- Celiac Disease: “”80 percent of success is just showing up”
- Improving Care Process in Celiac Disease
- How Slow Do Objective Markers of Celiac Disease Improve
- How Accurate is Serology at Predicting Mucosal Healing in Pediatric Patients with Celiac Disease
- Oral Treatment of Celiac Disease & Research Optimist | gutsandgrowth