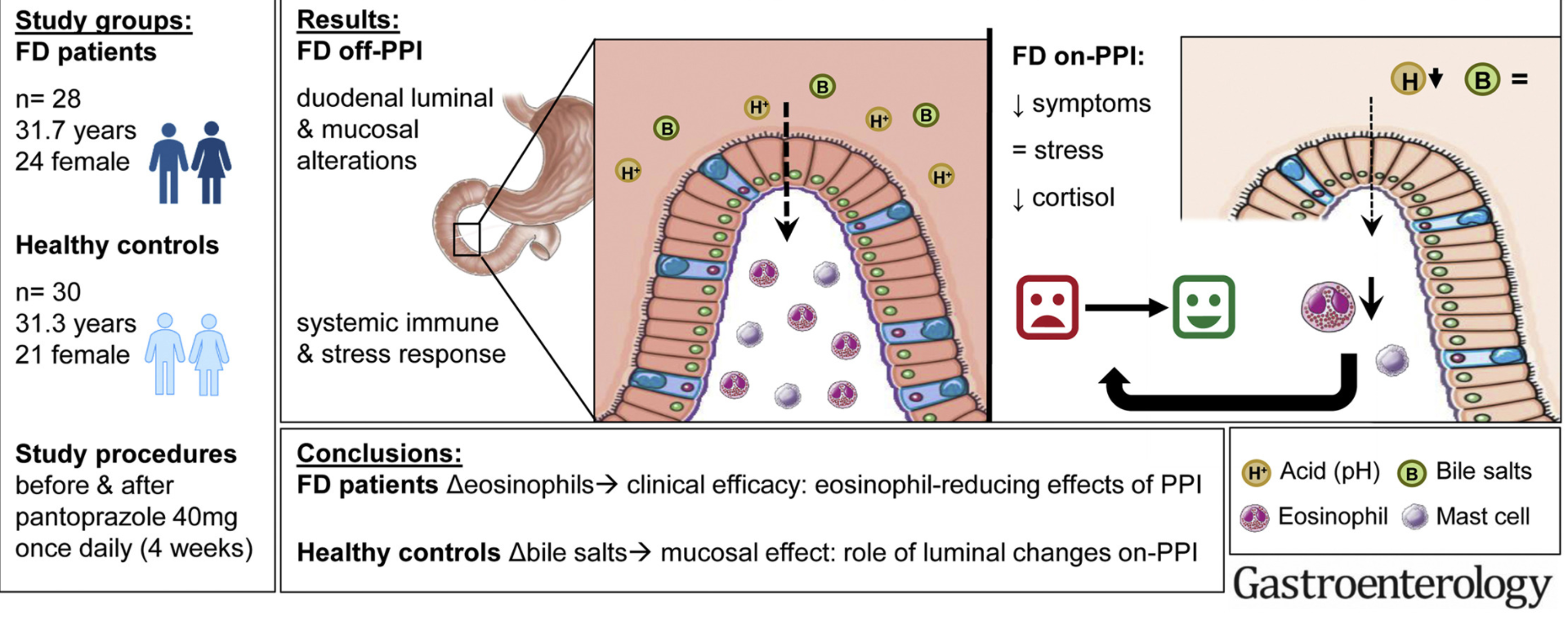
L Wauters et al. Gastroenterol 2021; 160: 1521-1531. Proton Pump Inhibitors Reduce Duodenal Eosinophilia, Mast Cells, and Permeability in Patients With Functional Dyspepsia
In this single-center prospective study, the authors show that pantoprazole (40 mg daily for 4 weeks) improves symptoms and duodenal eosinophilia in adults with functional dyspepsia (FD).
Key finding:
- Symptoms and duodenal eosinophils, mast cells (all, P < .0001), and paracellular passage (P = .02) were significantly higher in FD-starters (patients new to PPI treatment) vs HVs and reduced with PPI therapy.
- The authors note that systemic inflammation, subjective stress and salivary cortisol were also higher in patients with FD vs controls (off PPI).
My take: This study indicates that improvement in symptoms in FD related to PPIs is likely often due to improvement in duodenal mucosal inflammation and barrier dysfunction rather than by changing acidity.
Related blog posts:
- Algorithm for ‘Cursed’ Dyspepsia
- NEJM: Functional Dyspepsia (2015)
- Dreaded Nausea (2017) | gutsandgrowth
- Mirtazapine for Functional Dyspepsia
- A 6-Year Study of Amitriptyline, Escitalopram, and Functional …
- Will I Have This Stomach Pain Forever? (Part 1) | gutsandgrowth
- Cyproheptadine for dyspepsia | gutsandgrowth
- Does buspirone help functional dyspepsia? | gutsandgrowth
- Brave New World: Psychotropic Manipulation & Pediatric …