
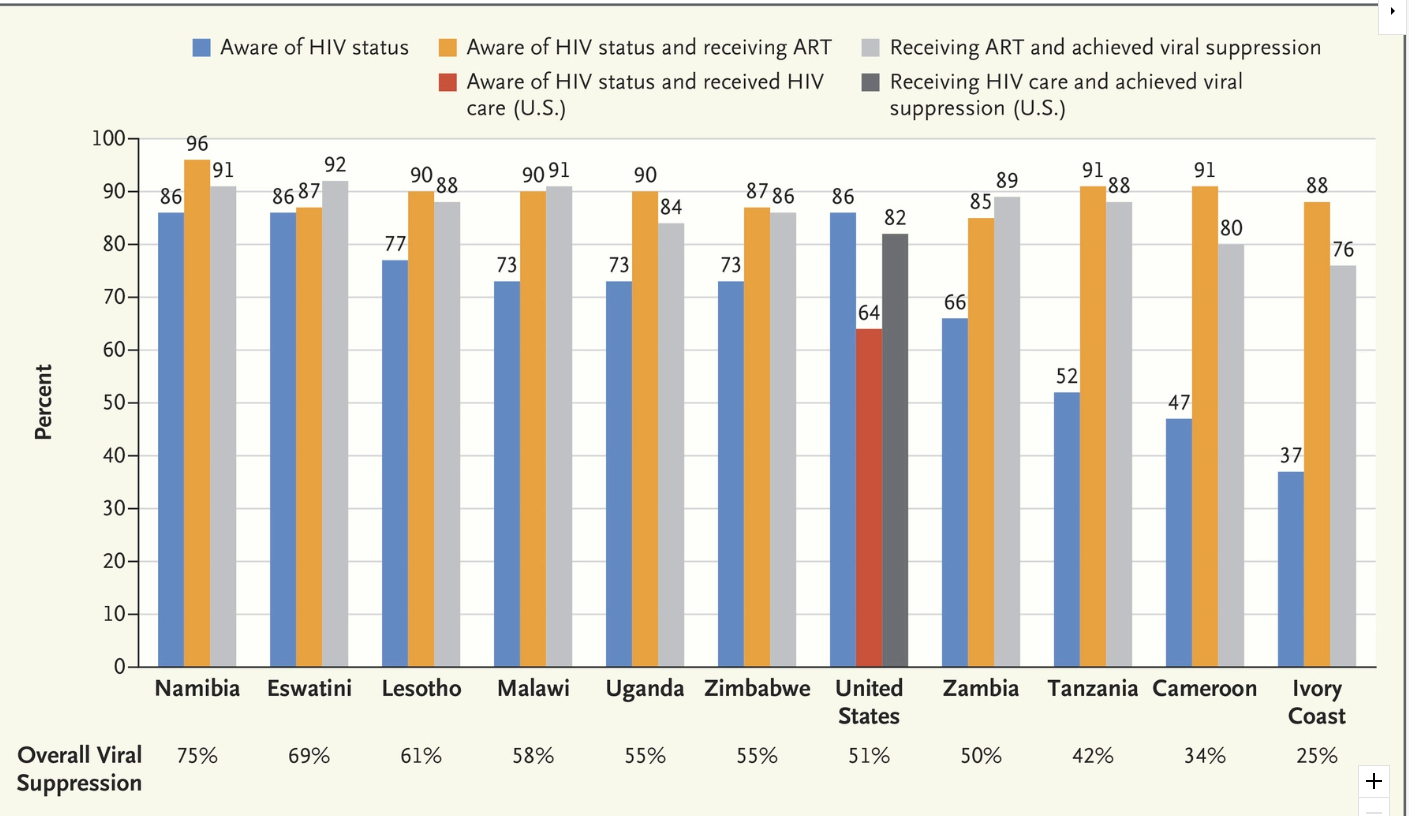
A recent commentary (WM El-Sadr et al. NEJM 2019; 380; 1985-7) shows how poorly we are doing in our efforts to diagnose and treat HIV in this country and what we need to do to make progress in eliminating HIV.
Overall, the U.S. overall viral suppression rate, which is the percentage of all people with HIV in whom the virus is suppressed, is only 51%. In contrast, the rates for Nambia, Uganda, and Zambia are 75%, 55%, and 50% respectively (U.S. measures use slightly different denominators than other countries.)
From NEJM twitter feed: AIDS in America –Back in the Headlines at Long Last
From NEJM twitter feed: https://www.nejm.org/doi/full/10.1056/NEJMp1904113

Link to Podcast: Ending the U.S. HIV Epidemic
A large retrospective study (M Deneau, M Perito, A Ricciuto, N Gupta et al. J Pediatr 2019; 209: 92-6) examined the outcomes/response of ursodeoxycholic acid (UDCA) for pediatric primary sclerosing cholangitis (PSC).
Background:
Study population/methods:
Key findings:
The authors note that “patients who do not achieve normalization could reasonably stop UDCA as they are likely not receiving clinical benefit.”
My take: This study shows that patients who have improvement/normalization of GGT with UDCA therapy have improved outcomes. The retrospective design of the study limits conclusions about whether UDCA therapy actually improves long-term outcomes, particularly since UDCA at higher doses has been associated with detrimental affects in adults with PSC.
Related blog posts:

Pablo Picasso, Le Compotier (Fruit Bowl) at Sofia Reina
https://www.museoreinasofia.es/en/collection/artwork/compotier-fruit-bowl
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Full Text via AGA Journal Link: Events Within the First Year of Life, but Not the Neonatal Period, Affect Risk for Later Development of Inflammatory Bowel Diseases
A recent study (CN Bernstein et al. Gastroenterol 2019; 156: 2190-7; editorial 2124) delves into the topic of early life risk factors for the development of IBD. In the background, the author note that in 2018, 267,983 Canadians (0.73%) were estimated to be living with IBD and there is a forecast that this will increase to 402,853 by 2030.
This study used a Manitoba database and examined the records of individuals diagnosed with between 1984-2010. In addition, they correlated this data with individual data of the postnatal period between 1970-2010. From this database, they analyzed 825 individuals with IBD and 5999 matched controls.
Key Findings:
It is unclear whether infections in early life increase the risk of IBD or whether other factors like antibiotics contribute to the higher rate of IBD. The authors did not find more immunodeficiency disorders in the IBD cohort compared to controls.
My take: This study identified genetic risk as substantially greater than specific environmental risks. However, the increasing incidence of IBD suggests that environmental factors are quite significant, as genetic risk factors are less likely to change enough to account for the changes in epidemiology. As such, there are a few explanations:

From AGA Journal link
Related blog posts:
1.From John Pohl Twitter Feed: FDA Warns of One Death Linked to Fecal Transplants (6/13/19)
An excerpt:
The consent should include, at a minimum, a statement that the use of FMT to treat C. difficile is investigational and a discussion of its potential risks.
“Two immunocompromised adults who received investigational FMT developed invasive infections caused by extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli (E.coli). One of the individuals died,” the agency said Thursday…
Openbiome, a nonprofit stool bank based in Cambridge, MA, told Focus: “We are saddened to hear of the recent patient death due to an infection from a multi-drug resistant organism (MDRO) transmitted through a fecal transplant. OpenBiome material was not involved. OpenBiome screens its donors and fecal transplant material for MDROs and related risk factors, and this serious event further highlights the importance of rigorous screening and clinical oversight for all fecal transplant procedures.”

2. FDA approval for IB-stim (a.k.a. Neuro-stim) device.
An excerpt:
IB-Stim treatment resulted in at least a 30% decrease in usual pain at the end of three weeks in 52% of treated patients compared to 30% of patients who received the placebo, and at least a 30% decrease in worst pain in 59% of treated patients compared with 26% of patients who received the placebo.
:Kovacic K1, Hainsworth K2, Sood M1, Chelimsky G1, Unteutsch R1, Nugent M3, Simpson P3, Miranda A4. Lancet Gastroenterol Hepatol. 2017 Oct;2(10):727-737. doi: 10.1016/S2468-1253(17)30253-4. Epub 2017 Aug 18.
Link to abstract of relevant study: Neurostimulation for abdominal pain-related functional gastrointestinal disorders in adolescents: a randomised, double-blind, sham-controlled trial.

3. FDA Approves Gattex (Teduglutide) for Pediatric SBS
From CenterWatch: Gattex New FDA Drug Approval
Pediatric SBS: “In a 24-week pediatric study 59 pediatric patients with SBS aged 1 year through 17 years chose whether to receive Gattex or standard of care (SOC)…Based on patient-diary data, patients who received Gattex 0.05 mg/kg/day experienced a 42% mean reduction in PS volume (mL/kg/day) from baseline (-23 mL/kg/day from baseline). At week 24, 38% of patients (10/26) were able to reduce PS infusion by at least 1 day per week. Patients reduced their PS infusion time by 3 hours per day on average compared to baseline.”
Related blog post: Teduglutide for SBS
Jeppesen PB, Pertkiewicz M, Messing B, Iyer K, Seidner DL, O’keefe SJ, Forbes A, Heinze H, Joelsson B Teduglutide reduces need for parenteral support among patients with short bowel syndrome with intestinal failure. Gastroenterology 2012 Dec;143(6):1473-1481
Jeppesen PB, Gilroy R, Pertkiewicz M, Allard JP, Messing B, O’Keefe SJ Randomised placebo-controlled trial of teduglutide in reducing parenteral nutrition and/or intravenous fluid requirements in patients with short bowel syndrome. Gut 2011 Jul;60(7):902-14.

NPR coverage of story: What’s Doctor Burnout Costing America?
An excerpt:
The study authors calculate that for health care organizations, the cost of burnout comes out to $7,600 per physician per year. The study notes that their cost estimate is conservative, only taking into account lost work hours and physician turnover. But other research shows burned out doctors are also more likely to make medical mistakes, have less satisfied patients, and get sued for malpractice, all of which have indirect costs.
Related blog posts:
A recent study (P Hopson et al. JPGN 2019; 68: 854-60) reports a high rate of isolated amylase deficiency of 10.1% in their cohort. Is this really accurate? I am skeptical.
Amylase Levels:
The technique for obtaining ePFT is detailed in the review (JPGN 2019; 68: 768-76) and includes the following:
I would suggest a more selective approach in utilizing endoscopy to check for both pancreatic function as well as disaccharidases. The sensitivity, specificity, positive predictive value and negative predictive value of a test is highly dependent on the study population. In those at low risk, the results of the testing is highly suspect.
My take: The reference to the review article is worth keeping as it gives a clear description of endoscopic pancreatic function testing. The study describing a 10% rate of amylase deficiency among a large cohort of pediatric patients requires careful interpretation, particularly as more than 80% of the deficiency group were less than 2 years of age. Clearly, a prospective study is needed. In those with possible isolated amylase deficiency at a young age (<2 years), a double-blind randomized trial may be needed to determine if enzyme supplementation is beneficial.
Related blog posts: Transient Exocrine Pancreatic Insufficiency or Misleading Tests?
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Camille Passaro, Rue Saint-Honore por la Tarde. Efecto de lluvia. Thyssen-Bornemisza Museum; https://www.museothyssen.org/en/collection/artists/pissarro-camille/rue-saint-honore-afternoon-effect-rain

Becker’s Hospital Review: Highest-paid CEOs in 2018: Who made the list from healthcare The full list includes 200 chief executives from public companies with revenue of at least $1 billion. Thanks to Jeff Lewis for pointing out this list.
Total compensation may include salary, bonuses, perks, stock and options.

Canaletto. El Gran Canal desde San Vio. Thyssen-Bornemisza Museum. https://www.museothyssen.org/en/collection/artists/canaletto/grand-canal-san-vio-venice
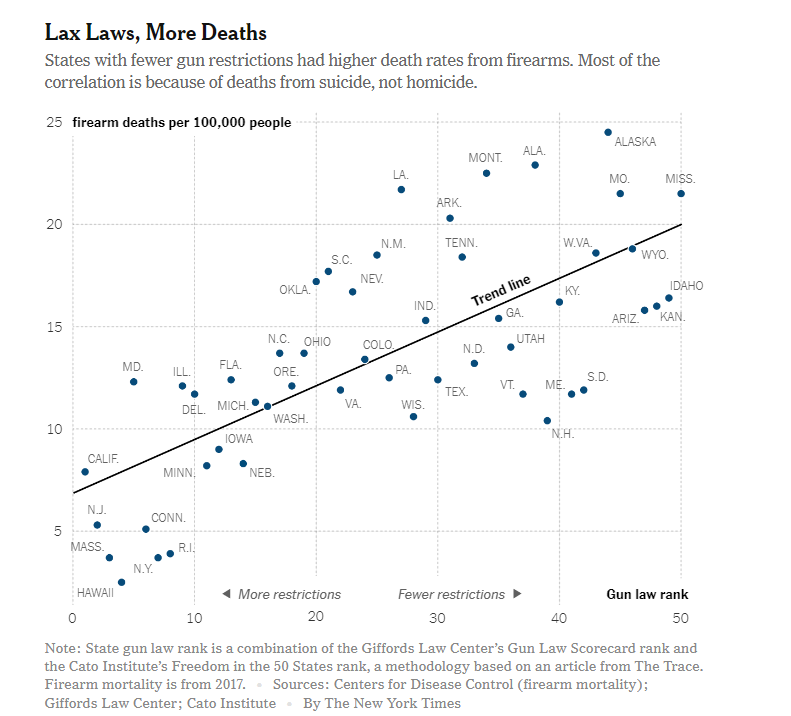
Those opposed to gun safety provisions (a.k.a. gun control legislation) argue that laws will not prevent criminals from obtaining firearms illegally. A recent commentary in NY Times provides some data that shows that states with more gun safety provisions have lower levels of gun-related deaths (especially suicides).
NY Times: A Gun Killed My Son. So Why Do I Want to Own One?
Related blog posts: