A recent ‘clinical quality forum’ sponsored by The Children’s Care Network (TCCN) and Nutrition4Kids featured several good lectures. The symposium was titled, “It’s Alimentary.” What follows are my notes –the full lectures from these talks will be available in the coming weeks on the Nutrition4Kids website. My notes may include some errors in transcription and errors of omission.
In my view the best lecture from this symposium was given by Kathleen Zelman (WebMD, Director of Nutrition): Diet and Nutrition Trends Impacting Health
Key points:
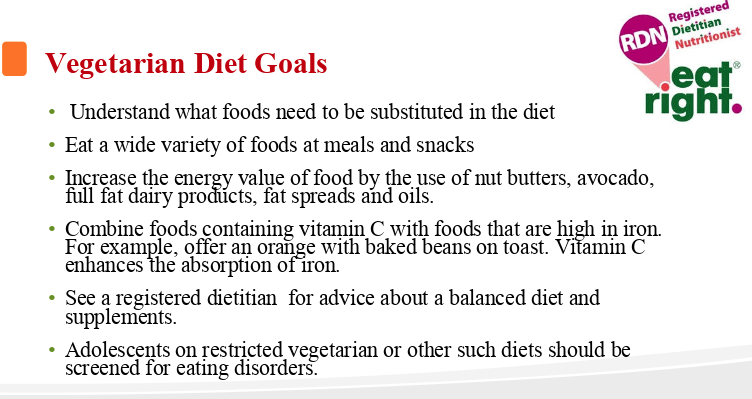
- There have been more individuals pursuing vegetarian and vegan diets. Though increasing vegetables/fruits is a good trend, vegan diets are particularly challenging (& potentially dangerous) in children. In those who take milk and eggs, this diet is much more likely to meet nutrient needs. These diets necessitate the assistance of a dietician.
- Unfavorable trends: increased consumption of highly processed foods and restrictive food fads. Some processed foods (eg. canned beans) can be a healthy addition to diet.
- ‘Organic diets are not more nutritious. They are great if you can afford it. Key is eating more vegetables and fruits.’
- GMOs are safe.
- MyPlate.gov is a good resource
- Encourage families to eat together and to shop for a ‘rainbow of colors’
Related posts:
- War on Science and Genetically-Modified Food | gutsandgrowth
- Expert Review: GMOs are safe | gutsandgrowth
- Understanding Your Food and Biotechnology (Part 2) | gutsandgrowth








A subsequent lecture on “Nutrition for the Premature Infant” by Heidi Karpen (Emory University, Professor of Pediatrics) provided a good overview of the ongoing efforts to improve nutritional outcomes for premature infants.
Key points:
- Good nutrition is crucial for better neurodevelopmental outcomes and stronger bones.
- Despite efforts like instituting TPN on first day of life, most neonates are losing ground during their hospitalization.
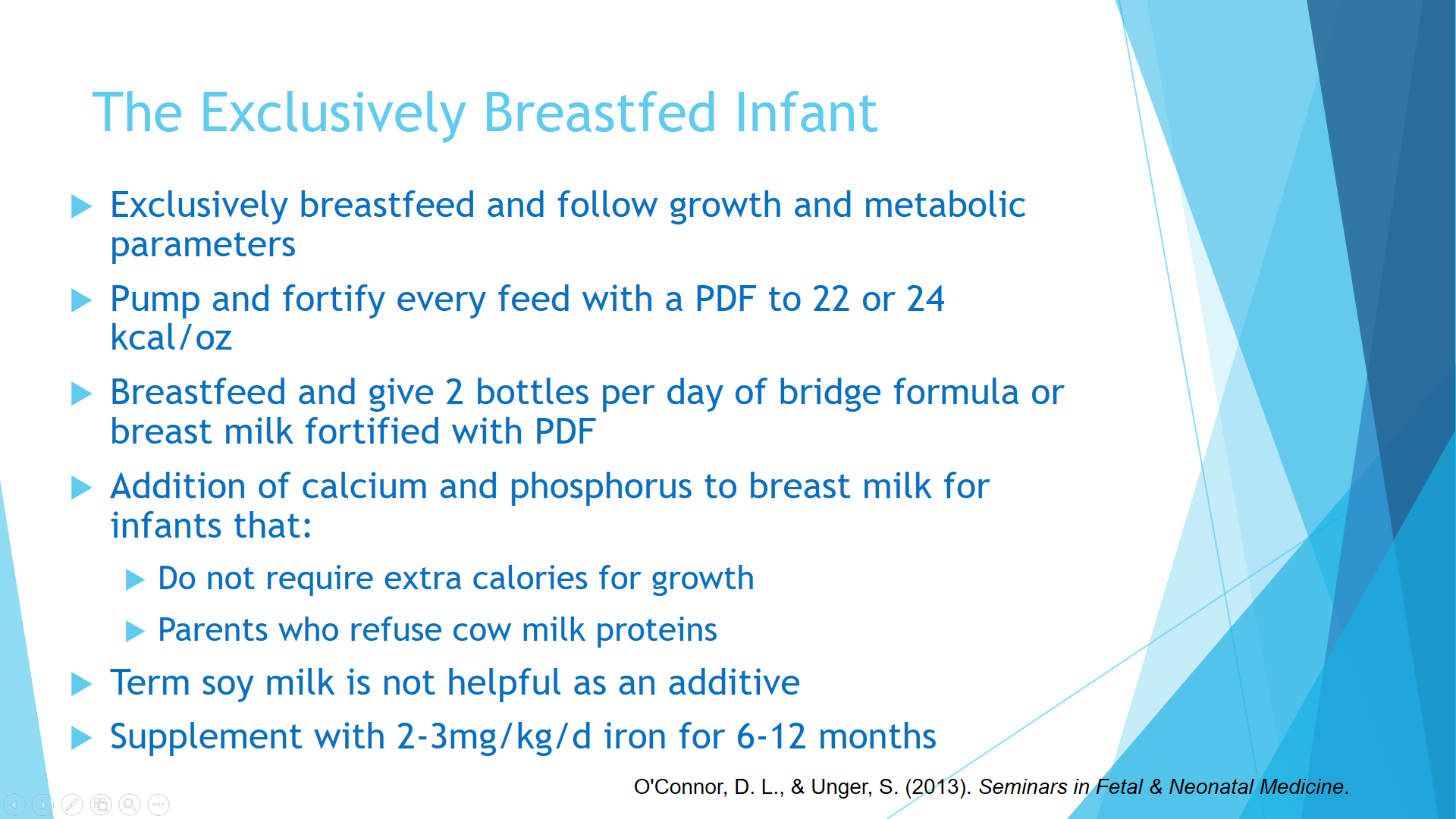
- Breastmilk is best at reducing sepsis, necrotizing enterocoliitis, and improving IQ. However, it is not perfect –less protein, less calcium, and less phosphorus than formulas; thus, breastmilk needs to be augmented and/or supplemented.
- Informal breastmilk donation can be dangerous. Donor breastmilk needs to be carefully screened.
Related blog posts:
- Improving Outlook for Neonatal Nutrition
- Neonatal Nutrition Lecture -What We Know Right Now …
- Current Mortality from Being Born Premature | gutsandgrowth
- Visual Acuity and LCPUFA | gutsandgrowth
- What’s Happening on the Edge of Viability | gutsandgrowth
- Weight Gain in Preemies, Neurodevelopmental Outcomes, and Reverse Causation | gutsandgrowth