M Roca et al. JPGN: October 2017 – Volume 65 – Issue 4 – p 394–398 Fecal Calprotectin and Eosinophil-derived Neurotoxin in Healthy Children Between 0 and 12 Years


M Roca et al. JPGN: October 2017 – Volume 65 – Issue 4 – p 394–398 Fecal Calprotectin and Eosinophil-derived Neurotoxin in Healthy Children Between 0 and 12 Years
A recent retrospective study (SY Yung et al. Ann Pediatr Endocrinol Met 2017; 22 https://doi.org/10.6065/apem.2017.22.3.189 –thanks to Jeff Schwimmer for this reference) describes the problem of nonalcoholic fatty liver disease (NAFLD) in long-term survivors of childhood-onset (CO) craniopharyngioma.
This study reviewed 75 children with CO-craniopharyngioma who had surgery prior to 15 years of age. The mean followup was 4.3 years.
Key findings:
This study had many limitations, including reliance of ultrasonography for diagnosis and incomplete evaluations. Despite this, it is clear that hypothalamic obesity places patients at a high risk for developing NAFLD. In addition, NAFLD in this population may be more aggressive.
My take: This study documents the well-recognized phenomenon of NAFLD in CO-craniopharyngioma with obesity. Current treatment relies on trying to preserve hypothalamic function and optimizing lifestyle/nutrition.
Briefly noted: D Valentini et al. J Pediatr 2017; 189: 92-7. Using ultrasound in 280 Italian children with Down syndrome, the authors identified NAFLD in 45% of those considered nonobese and 82% of those overweight/obese. In a related commentary (pg 11-13 Full text: Down syndrome and Pediatric NAFLD …), the authors (AD Matteo, P Vajro) note that Down syndrome patients may have increased NAFLD due to less activity, more obesity including possible excess adiposity in those with normal BMI, obstructive sleep apnea, or perhaps other mechanisms.
Related blog posts:
A recent retrospective study (S Jitaruch et al. J Pediatr 2017; 189: 79-85) documents the important association of autoimmune liver disease in children with sickle cell disease (SCD). I have seen children with hemoglobinopathy and autoimmune hepatitis.
Key findings:
My take: this report is a good reminder that though there are a good number of reasons for abnormal liver blood tests in children with SCD, it is important to follow these children closely and to obtain serology (including ANCA) in those with persistent elevations.
Related blog post: Blood is not enough

South Kaibab Trail at the basin of the Grand Canyon (Colorado River)


A recent prospective study (DA Katzka et al. Am J Gastroenterol 2017; 112: 1538-44 -thanks to Ben Gold for this reference) provided more information regarding the potential utility of the cytosponge for eosinophilic esophagitis (EoE); the cytosponge has been studied for Barrett’s esophagus.
Background: 86 adult patients were recruited; 6 could not swallow sponge. In the remainder, 105 procedures were performed comparing the cytosponge to standard endoscopic biopsies. The cytosponge technique can be completed in ~5 minutes without sedation. “All that is required is centrifuging the cytosponge specimen in its preservative to create a pellet followed by routine paraffin embedding and processing.”
Key findings:
The sensitivity of 75% is likely due to inadequate contact between cytosponge and esophageal wall which could be related to technique, especially in those with a normal caliber esophagus.
My take: The cytosponge appears to identify active EoE in the majority of adult patients. In those with abnormal cytosponge, the likelihood of active EoE would be very high; as such, it could be a useful biomarker. It is still probable that many with normal cytosponge result would need endoscopy due to suboptimal sensitivity.
Related blog posts:

NEJM 2017; 377: e22. In this patient with lingual papillomas, hx/o melenoma, and both hyperplastic and adenomatous polyps, a genetic mutation identifying Cowden syndrome was identified.
A recent study (Barnes EL et al. Clin Gastroenterol Hepatol 2017; 15: 1390-6) found an association between the intake of certain fatty acids and the risk of an ulcerative colitis flare. This is nicely summarized in the AGA Journals Blog.
Here’s the link: Does Consumption of Certain Fatty Acids Increase Risk of Ulcerative Colitis Flares?
Here’s an excerpt:
Diets with high levels of fatty acids such as myristic acid (found in palm oil, coconut oil, and dairy fats) increased risk of flare in patients with ulcerative colitis (UC), researchers report in the September issue of Clinical Gastroenterology and Hepatology. Their findings, from a prospective study of more than 400 patients in remission during treatment with aminosalicylates, could guide future studies of supplements or compounds that reduce risk of flares in patients with UC in remission…
Edward L. Barnes et al performed a prospective study of dietary patterns among 412 patients, from 25 sites, with UC in remission during monotherapy with an aminosalicylate (mesalamine, sulfasalazine, or balsalazide for at least 3 months before enrollment). Patients completed a validated food frequency questionnaire (on consumption of dairy, fruits, vegetables, eggs, meat, fish, cereals, breads, and starches, beverages, sweets, and baked goods) at enrollment and were followed for 12 months…
Forty-five patients (11%) had a relapse of UC within 1 year of study enrollment… In multivariable analysis, higher intake of myristic acid (odds ratio, 3.01) and alpha linolenic acid (odds ratio, 5.50) were associated with increased risk of relapse, although a dose–response relationship was retained only for myristic acid intake.
Other foods previously implicated in flares of UC, such as processed meat, alcohol, and foods high in sulfur, were not associated with an increased risk of flare.
Related blog posts:

From Andy Warhol Exhibit at the High Museum
A recent study (A Kloop et al. J Pediatr 2017; 190: 192-9) examined the relationship between mode of infant feeding and the development of asthma. The authors used prospective data from 3296 Canadian children in the Canadian Healthy Infant Longitudinal Development (“CHILD” study) cohort.
Key finding:
The authors speculate that the direct breastfeeding may offer some advantages over expressed breast milk:
Since this is an observational study and patients were not randomized there may be other unrecognized confounding variables.
Another study in the same issue (AF Beck et al. J Pediatr 2017; 190: 200-6) assessed whether the Child Opportunity Index (COI) was associated with asthma outcomes in a retrospective cohort of 5462 children in Hamilton County, Ohio. The COI (see below for the measures in this index) has previously been linked to life expectancy, low birth weight, and prematurity. Interestingly, one can go to diversitydatakids.org to see how this affects your location (here is the link for a heat map of this index in the Atlanta area: Atlanta COI)
Key finding:
My take: The first study indicates that direct breastfeeding is associated with lower rates of asthma. The second study shows that issues related to education, environment, and social/poverty have an enormous impact on need for asthma-related hospitalization.
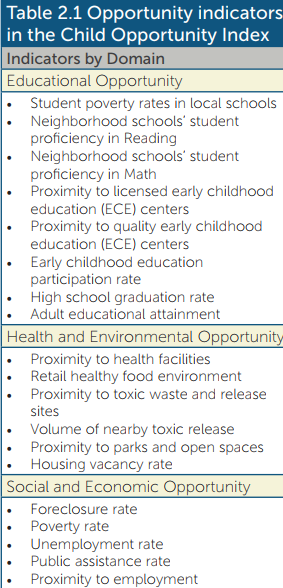
Accessed 12/10/17 from: http://www.diversitydatakids.org/files/Library/Child%20Opportunity/COI%20Report%20Final%207_29_16.pdf
A recent study examines the market share and costs of biologic therapies for inflammatory bowel disease:
Excerpt from abstract:
The vast majority of costs allocated to out-patient IBD medications in the USA is attributed to increasing use of biologic therapies despite the relative minority of biologic-taking patients.
My take: Biologic therapies are costly but also very effective.
Related Blog Posts:
A recent study (M Lazzerini et al. Clin Gastroenterol Hepatol 2017; 15: 1382-9) used data from 2 multicenter trials of 70 children to assess the efficacy of thalidomide in pediatric patients with refractory inflammatory bowel disease (37 with Crohn’s disease, 23 with ulcerative colitis)
Key findings:
My take: I have not used thalidomide therapy and remain concerned about long term side effects (eg. peripheral neuropathy). Though, the authors are correct that its safety “may be acceptable compared with the safety of other” treatments, especially if there are few remaining options.
Related blog posts:

A recent study (J Kamgno et al. NEJM 2017; 377: 2044-52) used an innovative cell-phone-based device (the LoaScope) to improve treatment of onchocerciasis (river blindness).
Background (summarized in editorial: pg 2088-90): Ivermectin has been distributed in Africa since 1988 to treat onchocerciasis; in fact, the 2015, Nobel Prize in Medicine was shared by the discoverers of ivermectin. However, in 1996, it was recognized that central nervous system adverse events were occurring in ivermectin-treated patients with coexistent Loa loa infection.
Kamgno et al show that not treating patients with L loa counts >20,000 microfilariae per mL helps target ivermectin to those who will benefit. The LoaScope identified 340 persons who were at high risk for serious adverse events; the authors estimate that 62 serious central nervous system complications and 8 deaths were avoided with this approach.
Despite the apparent success of this mobile Health (mHealth) application, a separate editorial cautions that most mHealth has little data to support its use (A Roess. NEJM 2017; 377: 2010-11). Key points:
My take (with help from editorial): mHealth tools are here and increasing. Advances like the LoaScope for treating river blindness has been shown to improve outcomes. Before recommending other mHealth tools, we need to insist on adequate evaluation or we will “arrive in an increasingly fragmented mHealth landscaped littered with poor-quality, unproven apps.”
Related blog posts:

Sunrise at the Grand Canyon’s South Rim