GI Care for Kids physician, Jeff Lewis, helped bring fecal microbiota transplant (FMT) to Georgia. Here’s a success story from Fox5 Atlanta from August 31, 2015. Here’s the link:
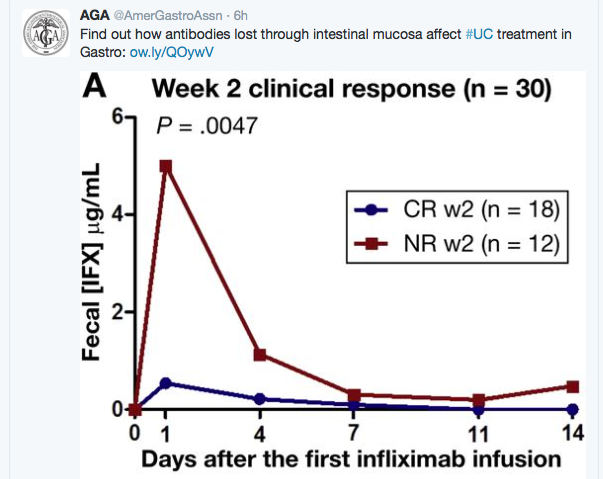
In this study, the authors obtained fecal samples from 30 consecutive patients with moderate to severe UC during the 1st 2 weeks of therapy. In addition, they obtained serum infliximab levels as well as assessed clinical and endoscopic response at 2 weeks, 8 weeks, and 3 months after treatment began.
Key findings:
Fecal infliximab was detected in 129 of 195 (66%) samples. The greatest loss was observed approximately 2 days after infusion. Low serum albumin was associated with greater infliximab levels in the stool.
Clinical nonresponders at week 2 had significantly higher fecal infliximab
The authors did not observe a correlation between fecal and serum infliximab concentrations. However, it is possible that stool losses could indicate lower mucosal concentrations of infliximab.
From AGA twitter account
From AGA twitter account
From AGA twitter feed
Bottomline: It is not clear whether stool losses of infliximab directly contribute to drug failure or whether the loss is another biomarker of disease activity/high-risk patients.
The study authors note that “intestinal loss of IFX in moderate to severely active UC is associated with a diminished response to this treatment. Patients with severe disease can, therefore, benefit from more intensive dosing regiments. This strategy warrants a prospective clinical trial.”
The best data to date: D Lee et al. Inflamm Bowel Dis 2015; 21: 1786-93. In this prospective study, the authors studied treatment initiation in children (N=90), comparing partial enteral nutrition (PEN, n=16), exclusive enteral nutrition (EEN, n=22), and anti-TNF therapy (n=52).
Results:
Clinical response, defined by PCDAI reduction ≤15 or final PCDAI ≤10, was achieved by 64% PEN, 88% EEN, and 84% anti-TNF.
Fecal calprotectin ≤250 noted in 14% PEN, 45% EEN, and 62% anti-TNF
Because of the discrepancy between EEN and PEN, the authors speculate that the “efficacy of EEN may be a consequence of elimination of table food rather than providing a uniquely therapeutic method of delivering nutrients.” They note that “choice of formula has not impacted the efficacy of enteral nutrition.”
More extensive information on this subject: D Lee et al. Gastroenterol 2015; 148: 1087-1106.
Bottomline: Anti-TNF therapy was as effective or more effective than EEN. And, “for patients who prefer treatment with a nutrition-based therapy, EEN seems superior to PEN.”
While entecavir and tenofovir have been in use for many years in adult hepatology for hepatitis B virus (HBV) infection, a well-designed study supporting their use in pediatrics has been lacking until now. Recently, a study (M Jonas et al. Hepatology 2015; DOI: 10.1002/hep.28015) has shown that entecavir is effective for pediatric HBV
This ongoing, randomized phase III study assesses the safety and efficacy of entecavir versus placebo in nucleos(t)ide-naive children (2 to <18 years) with HBeAg-positive chronic hepatitis B (CHB). Blinded treatment was administered for a minimum of 48 weeks. After Week 48, patients with HBeAg seroconversion continued blinded treatment; those without, switched to open-label entecavir. The primary endpoint was HBeAg seroconversion and HBV DNA <50 IU/mL at Week 48. A total of 180 patients were randomized (2:1) and treated. Baseline median age was 12 years, with approximately 50% of children aged >12 to <18, and 25% each aged ≥2 to ≤6 and >6 to ≤12. Rates for the primary endpoint at Week 48 were significantly higher with entecavir than placebo (24.2% [29/120] versus 3.3% [2/60]; P=0.0008). Furthermore, higher response rates were observed with entecavir compared with placebo for the key Week 48 secondary endpoints: HBV DNA <50 IU/mL (49.2% [59/120] versus 3.3% [2/60]; P < 0.0001), alanine aminotransferase normalization (67.5% [81/120] versus 23.3% [14/60]; P < 0.0001), and HBeAg seroconversion (24.2% [29/120] versus 10.0% [6/60]; P = 0.0210). Among entecavir-randomized patients there was an increase in all efficacy endpoints between Weeks 48 and 96, including an increase from 49% to 64% in virologic suppression. The cumulative probability of emergent entecavir resistance through Years 1 and 2 of entecavir was 0.6 and 2.6%, respectively. Entecavir was well tolerated with no observed differences in adverse events or changes in growth compared with placebo. Conclusion: In childhood CHB, entecavir demonstrated superior antiviral efficacy to placebo with a favorable safety profile. These results support the use of entecavir as a therapeutic option in children and adolescents with CHB.
Picky eating, even at moderate levels, is linked with psychiatric problems, including anxiety and symptoms of depression in kids, according to a study published Monday in the journal Pediatrics. It found the mental problems worsened as the picky eating became more severe.
“We need to do a better job of giving advice to these parents,” Nancy Zucker, study co-author and associate professor of psychology at Duke University, told NBC News.
“The first take-home message is that you’re not to blame. The second take-home message is that it’s more complicated than we think.”
The study screened more than 1,000 children ages 2 to 5, and found 20 percent were picky eaters. The researchers stress this goes beyond kids who just hate broccoli or have certain dislikes.
More than 17 percent of kids were classified as moderate picky eaters: These children had a very limited range of foods they would eat and they would not try anything else, Zucker said.
About 3 percent were considered severe picky eaters: Their sensitivities to smell or taste were so strong that even eating outside of the home was difficult. As they get older, it could be hard for them to go out with friends or eat at school. …
The researchers also note the term “picky eating” may now be obsolete. They suggest the condition might be better described as avoidant/restrictive food intake disorder (ARFID).
A recent study indicates that a fairly high number of adults with appendicitis could avoid surgery (JAMA 2015 June 15 [doi:10.1001/jama.2015.6154]).
In this study, patients with CT-confirmed acute uncomplicated appendicitis were randomly assigned to either immediate surgery (n=273) or a 1-day of IV ertapenem followed by 7 days of levofloxacin and metronidazole.
The primary endpoint for the antibiotic group – resolution of acute appendicitis with no recurrences for a full year – occurred in 73%. The remaining 27% of patients in this group underwent appendectomy during follow-up, at a median of 102 days after initial presentation. None of these patients developed abscesses or serious infections, “suggesting that the decision to delay appendectomy … can be made with a low likelihood of major complications,” the investigators said
And commentary from Edward Livingston, M.D., is deputy editor of JAMA. Corrine Vons, M.D., Ph.D., is in the digestive surgery department at Jean-Verdier Hospital, Bondy, France. :
The study findings dispel the notion that appendectomy is always an emergency and suggest instead that, given our current precise diagnostic capabilities and effective wide-spectrum antibiotics, a trial of antibiotic therapy is reasonable. However, it’s important to note that children, adolescents, pregnant women, and patients with complications were excluded from this trial so the findings do not apply to those patient groups.
Dr. Livingston and Dr. Vons made these remarks in an editorial accompanying Dr. Salminen’s report (JAMA 2015;313:2327-8).
My Take: This study indicates, at least in adults with uncomplicated appendicitis, that antibiotic treatment is an option. I think resolving the problem definitively would be my preference. If you had appendicitis, which therapy would you choose? Take the poll.
They used another virus called MS2 that’s similar to norovirus, that doesn’t make people sick and that’s easy to grow in the lab.,,
“We think that there’s a at least a million particles released in a vomiting event and maybe more.”
Not all of it goes into the air. In fact, very little did in their experiments. But it was enough. They estimate that as many as 13,000 virus particles can be released into the air with a single retch. They made a video that shows how it works.
“There was evidence of aerosolized MS2 after every simulated vomiting episode,” they wrote in their report, published in the Public Library of Science journal PLoS ONE.
People can be infected with as few as 20 to 1,300 microscopic viral particles, so their study shows that vomiting could indeed spread the infection through the air….
“WHEN ONE PERSON VOMITS, THE AEROSOLIZED VIRUS PARTICLES CAN GET INTO ANOTHER PERSON’S MOUTH AND, IF SWALLOWED, CAN LEAD TO INFECTION.”
“There are 21 million cases of human norovirus infection in the U.S. each year, and this virus genus is now recognized as the leading cause of outbreaks of acute gastroenteritis,” the researchers wrote.
It kills up to 800 people a year in the U.S. alone and puts 70,000 into the hospital, so understanding how it spread sand finding ways to stop it could prevent many illnesses, the researchers said.
An interesting study in Pediatrics has found that avoiding temporary NICU names can result in fewer errors. Here is the NY Times summary:
More than 80 percent of neonatal intensive-care units, or NICUs, use temporary first names for patients — Babygirl Jackson or Babyboy Goldsmith, for example — a convention that may lead to errors in prescribing medicines. A new study has found that a simple change in this procedure can significantly reduce such errors.
The NICUs at Montefiore Medical Center in the Bronx instituted a new system two years ago. They started naming babies using the mother’s first name — Jennifersgirl Jackson and Karensboy Goldsmith. Researchers compared the number of wrong-patient electronic orders of medicines in the year before the change with the number in the year after. The study, in Pediatrics, included 158,000 orders before the change and 142,000 after.
Over all, the new system reduced errors by 36.3 percent.
My Take: Both with electronic records and with ‘paper’ records, the lack of a specific name leads to errors. With electronic records, another frustration is when multiple records for the same patient have not been merged into a single entity, allowing key information to be unavailable.
In 2003, Wald and Law proposed to combine 3 half-dose antihypertensive agents, an intermediate-dose statin, low-dose aspirin, and folic acid into a once per day polypill for primary and secondary prevention of cardiovascular disease. Based on epidemiological models, they estimated that daily use by individuals aged 55 years or older could reduce the incidence of MI and stroke by more than 80%.
In the 12 years since this report was published,3 versions of the polypill have been successfully tested in several phase 2 (safety) studies and a few modest-sized phase 3 (efficacy) trials. Collectively, these studies demonstrated that the polypill was well tolerated, achieved good adherence, and based on intermediate end points, such as reduction of blood pressure and low-density lipoprotein cholesterol level, is efficacious…
The 4 drugs in the current version of the polypill have long histories of safe use. Although all 4 are frequently prescribed in the United States, the US Food and Drug Administration (FDA) has not approved combining them in a single pill…
Although the polypill could produce substantial public health benefits, people in the United States are unlikely to find out anytime soon. This is because the pill’s price is so low (≤$1 per tablet) and the cost of the large clinical trials required for FDA approval is so high, it is unattractive to investors. The inventor’s dilemma is that creating a product that improves health is not enough; the product must also be able to generate a healthy return on investment. In the United States, the surest way to generate a healthy return on investment is to increase health care spending, not reduce it.
This past week I’ve been on call and had not finished a few articles. One article that was on the to do list: A Lang et al. Clinical Gastroenter Hepatol 2015; 13: 1444-9.
I’ve read it now. However, even before finishing the article, I read a few good summaries of this article, including one from my colleague Stan Cohen/Nutrition4Kids: Curcumin Helps (A Lot) in Ulcerative Colitis
Here’s an excerpt:
The cover of a prestigious medical journal shows a pile of curcumin and over it, the announcement reads: Curcumin Helps Induce Remission in Mild-to-Moderate Ulcerative Colitis. That’s big news for a lot of reasons: first, this Indian spice (derived from tumeric) is inexpensive and well-tolerated; second, in a well-designed scientific study, curcumin showed that it was more effective than some medicines; and third, it showed, again, that careful trials of long-used herbs can be done with important results being shown. Again, because an earlier study (H Hanai, Clinical Gastroenterology 2006, pages 1502-6) had previously shown that curcumin can help keep ulcerative colitis (UC) patients from flaring for up to 12 months.
This new study (A Lang, Clinical Gastroenterology 2015, pages 1444-9) compared curcumin to a placebo in patients who were not doing well on the standard therapy (mesalamine) for mild to moderate UC. With a single daily dose of 3 grams of curcumin in capsule form, 65% responded (compared to 12% with a placebo) and 54% actually went into remission, having essentially no symptoms. Perhaps even, more importantly, 38% of those taking the curcumin showed improvement in the intestinal tissue when a colonoscopy was performed. That’s comparable or better than some of the medications that are being used.
A few other details: The researchers used a product called Cur-Cure from Bara Herbs Inc (Yokneam, Israel). Also, the associated commentary in the same journal by CN Bernstein (pages 1450-52) suggests that the study may have targeted mild ulcerative colitis (rather than moderate ulcerative colitis). He comments that the increasing rates of ulcerative colitis among Indian immigrants could be related to including less curcumin in their now more westernized diets. He also notes, as did Dr. Cohen, that there were previous promising studies dating back to 2006. Why has it taken nine years for this report?
My Take: This is probably an article worth reading. Although curcumin appears promising, I worry that a lack of financial incentive may hamper research efforts to better define its place as an agent for treatment of ulcerative colitis.