From Financial Times Website: Coronavirus Tracker



From Financial Times Website: Coronavirus Tracker
D Lin et atl. Clin Gastroenterol Hepatol 2020; 18: 763-6. In a retrospective chart review, the authors examined pharmacy data from patients in the Harris Health System (Harris county -Houston, TX) which had more than 1.9 million outpatient clinic visits in 2017.
In January 2018, multiple efforts were made to try to reduce inappropriate proton pump inhibitor (PPI) usage. This included grand rounds and system-wide emails to providers. In addition, a suggested tapering algorithm (order in EPIC) was given to reduce the likelihood of rebound acid hypersecretion which could undermine the goal of stopping PPI.
Key points:
My take: This study indicates that 1 in 6 PPI users were able to de-escalate off treatment. Physician initiative is crucial to improve appropriate medication use.
Related blog posts:
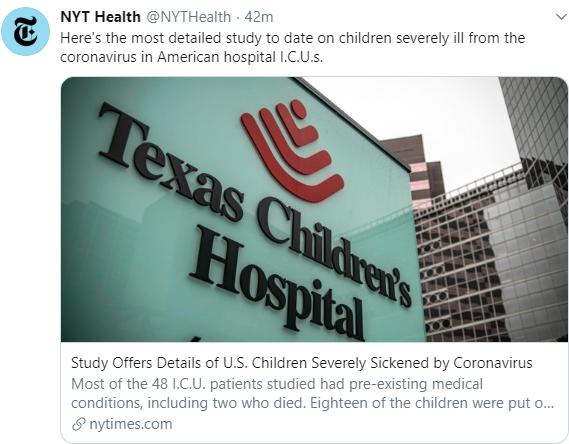
Recent study from JAMA Pediatrics (5/11/20) -Full text: Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units
Of the 48 children with COVID-19 admitted to participating PICUs (14 hospitals)… Forty patients (83%) had significant preexisting comorbidities; 35 (73%) presented with respiratory symptoms and 18 (38%) required invasive ventilation….At the completion of the follow-up period, 2 patients (4%) had died and 15 (31%) were still hospitalized, with 3 still requiring ventilatory support and 1 receiving extracorporeal membrane oxygenation. The median (range) PICU and hospital lengths of stay for those who had been discharged were 5 (3-9) days and 7 (4-13) days, respectively.
NY Times Summary of Study: Details of U.S. Children Severely Affected by Coronavirus
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
A recent retrospective study (PD Ngo et al. JPGN 2020; 70: 462-7) describes the largest published experience with intralesional steroid injection (ISI) for esophageal anastomotic strictures; the population studied in this report were strictures associated with esophageal atresia (EA) repair.
Key Details:
Key findings:
The study has a number of limitations including lack of precision/reproducibility with stricture diameter with dilatation; in addition, it was non-randomized and retrospective.
My take: This study, completed in a highly-specialized center, provides evidence that stricture dilatation following esophageal atresia repair is likely to be more successful with steroid injection.
Related blog posts:
Also, a good read (thanks to 33mail Bryan Vartabedian for this reference): Can We Discuss Flatten-the-Curve in COVID19? My Eight Assertions by JOHN MANDROLA, MD
” I will argue that the cumulative deaths from COVID19 will not be reduced significantly by flatten-the-curve policies. And that this virus will be as dangerous to vulnerable patients in 6 months to a year. We should be allowed to debate this.”
Key points: flattening of the curve does not mean that we will substantially lower the total mortality related to COVID-19 –though hospitals now have had time to avoid being overwhelmed. The virus is not contained, tests will underperform, new treatments do not help much (thus far), the overall mortality is ~1%, it may be difficult for a vaccine to prove its effectiveness, and COVID-19 (& our response) will likely lead to a large number of deaths not due to COVID-19.

Curbside Humor
NY Times: We Knew the Coronavirus Was Coming, Yet We Failed
“The vulnerabilities that Covid-19 has revealed were a predictable outgrowth of our market-based health care system.”
Here’s Why:
1. Ventilators. Operated as businesses, hospitals have zero incentive to stockpile. A vast storeroom in the basement filled with ventilators that might be needed once in a generation or never?…They are unlikely to do so unless government requires them. We’ve long required ocean liners to have lifeboats and life preservers even though their operators hope to never hit an iceberg.
2. Testing has proved the persistent Achilles’ heel in the U.S. response…[Early on] With requirements for Food and Drug Administration approval expensive and cumbersome, developing a test was a business non-starter…In contrast, South Korea, with its national health system, engaged its private test manufacturers with a plan in January, promising them quick approval for a coronavirus test and the widespread use of it in nationally organized and financed testing.
3. Testing components and P.P.E. …Conducting tests involves access to a number of components — kits, chemical reagents, swabs, personal protective equipment, sometimes custom cartridges for machines. Miss any one of those things and testing becomes impossible. It’s like trying to make bread with all the ingredients except yeast….Without a national system for such purchases in a crisis, we are essentially forcing hospitals and states to negotiate the price of water during a drought. (Alternatively, we could require all hospitals to have a 90-day supply of essential response items on hand, as Gov. Andrew Cuomo of New York has now done.)
4. Hospitals did not coordinate...In our market-based system, hospitals are primed to compete, not coordinate
5. The hospital rescue... [is needed] partly because they have delivered extraordinary treatment of Covid-19 (which doesn’t pay well) but also because they’ve had to cancel high-profit procedures like joint replacements and sophisticated scans to make room for this low-profit-margin illness…In a functioning health system, pandemic preparedness and response would be part of the expected job.
Whether regulated or run by the government, or motivated by new incentives, we need a system that responds more to illness and less to profits.
Related article: NY Times: How Health Insurers Can Be Heroes. Really.
“The industry is profiting from the pandemic. It needs to pay back by cutting premiums and co-payments, help private practices and finance more protection and care…A great paradox of this pandemic is that while Covid-19 is overwhelming the health care system, health care spending is down a whopping 18 percent. ”

NEJM: Children with Covid-19 in Pediatric Emergency Departments in Italy
Key points:
My take: This study provides additional data indicating that severe outcomes are rare in children with Covid-19.
Related article from NY Times: How Coronavirus Mutates and Spreads
An excerpt:
Researchers have found that the coronavirus is mutating relatively slowly compared to some other RNA viruses, in part because virus proteins acting as proofreaders are able to fix some mistakes. Each month, a lineage of coronaviruses might acquire only two single-letter mutations.
In the future, the coronavirus may pick up some mutations that help it evade our immune systems. But the slow mutation rate of the coronavirus means that these changes will emerge over the course of years.
That bodes well for vaccines currently in development for Covid-19. If people get vaccinated in 2021 against the new coronavirus, they may well enjoy a protection that lasts for years.
Related blog posts:

From NPR: COVID-19 Tests That Are Supposed To Be Free Can Ring Up Surprising Charge
An excerpt:
This reality means some medical providers… must rule out other respiratory diseases before ordering a COVID-19 test, leaving some patients with a difficult choice. Do they seek medical attention and risk a high medical bill? Or do they forgo care altogether?
A second hole in these federal protections may leave patients holding the bill for their COVID-19 test. The law prohibits insurers from charging patients for testing, but it does not block medical providers from doing so. If an insurer does not cover the total amount charged by a provider, the patient may get balance-billed, or slapped with a surprise charge.

From USAToday:


Related blog post:‘Quietly’ Testing Famotidine for COVID-19
From NY Times:

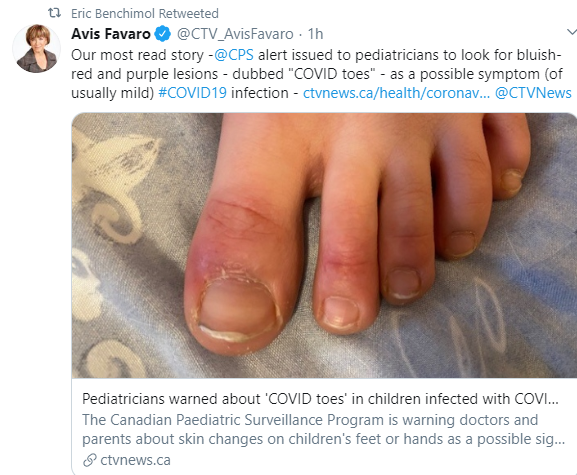
USA Today (4/27/20): Doctors find more cases of ‘COVID toes’ in dermatological registry. Here’s what they learned
An excerpt:
Dr. Esther Freeman, director of Massachusetts General Hospital Global Health Dermatology and member of the AAD task force on COVID-19, said COVID toes are pinkish-reddish “pernio-like lesions” that can turn purple over time…
While experts can’t confirm why COVID toes appear, they have some educated guesses. One could be inflammation in the toes’ tissue… Another hypothesis is inflammation of the blood vessel wall, medically known as vasculitis. And finally, … it is possible COVID toes could be caused by small blood clots that form inside the blood vessel…
COVID toes have appeared in some cases of asymptomatic patients. The majority of the toe cases manifested simultaneously or after more common COVID-19 symptoms, rather than before.
My take: During this pandemic, I need to look at my patient’s feet.
Yesterday, I received two emails (first from Steven Liu) about an article in Science and today I’ve already seen this article is referenced in a CNN report:
New York Clinical Trial Quietly Tests Heartburn Remedy Against Coronavirus
Key points:
My take: Famotidine may be a hot commodity –at least until studies are completed. Based on experience with hydroxychloroquine, some of our patients may need to look for alternative acid blockers.
Related blog posts:

Correction: Today’s earlier blog post has been updated:
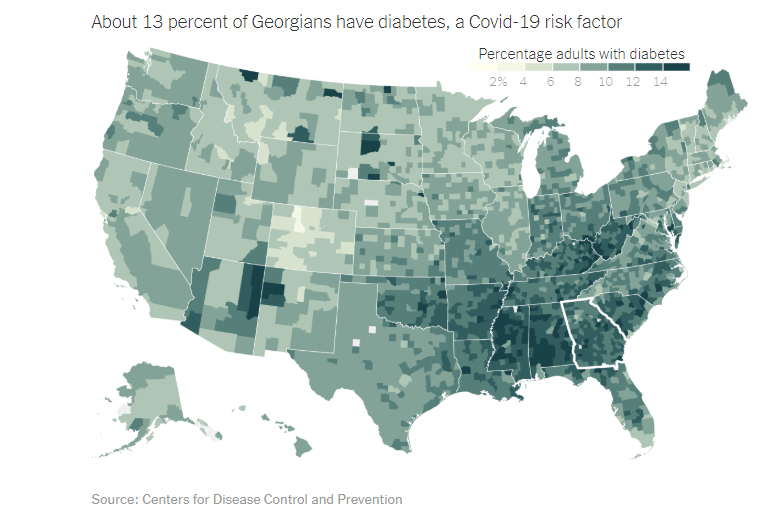
From NY Times: Why Georgia Isn’t Ready to Reopen
Key points: