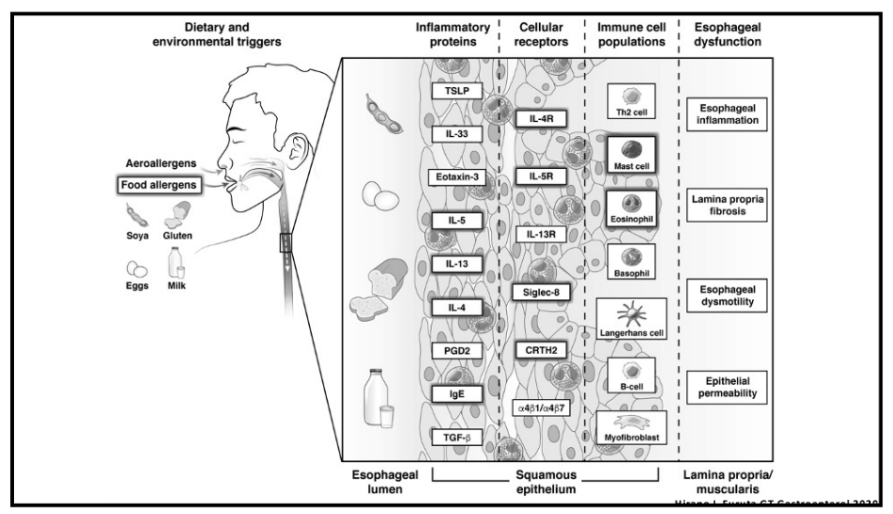
M Chehade et al. NEJM 2024;390:2239-2251 Dupilumab for Eosinophilic Esophagitis in Patients 1 to 11 Years of Age
This study provides published data that has been referenced previously at time of FDA approval and prior meetings (see posts: Dupixent Approved in Younger Children (15 kg+), Dupixent for Eosinophilic Esophagitis (1-11 yrs) and Clinical Diagnosis of Rumination from DDW Tweets).
Methods:
- Part A -In this phase 3 trial, we randomly assigned, in a 2:2:1:1 ratio, patients 1 to 11 years of age (n=102) with active eosinophilic esophagitis who had had no response to proton-pump inhibitors to 16 weeks of a higher-exposure or lower-exposure subcutaneous dupilumab regimen or to placebo (two groups)
- Part B- At the end of Part A, eligible patients in each dupilumab group continued the same regimen and those in the placebo groups were assigned to higher-exposure or lower-exposure dupilumab for 36 weeks
Key findings:
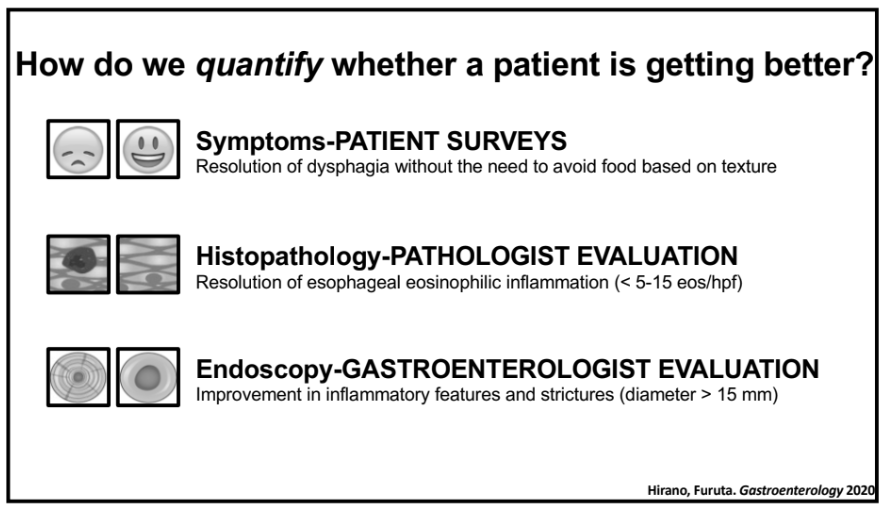
- In Part A, histologic remission occurred in 25 of the 37 patients (68%) in the higher-exposure group, in 18 of the 31 patients (58%) in the lower-exposure group, and in 1 of the 34 patients (3%) in the placebo group
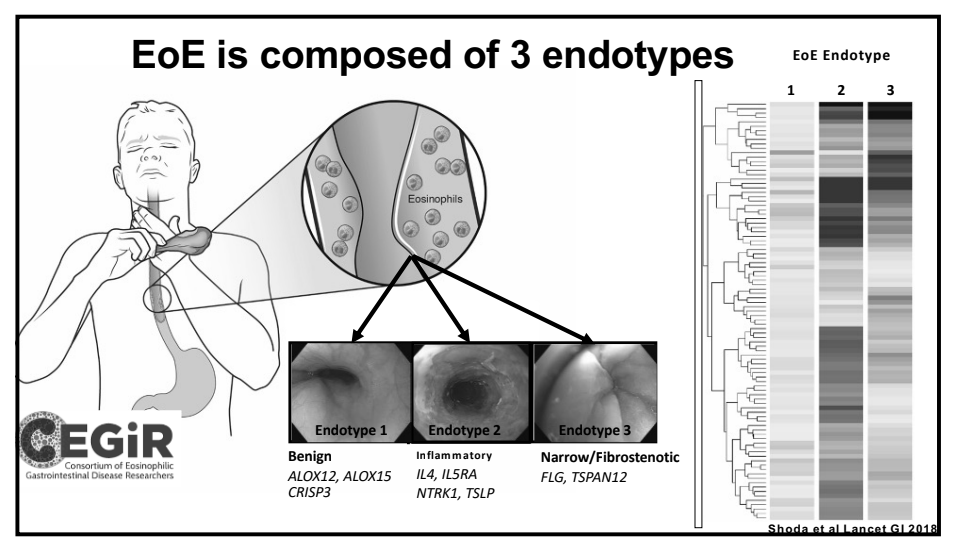
- The higher-exposure dupilumab regimen led to significant improvements in histologic, endoscopic, and transcriptomic measures as compared with placebo
- The improvements in histologic, endoscopic, and transcriptomic measures between baseline and week 52 in all the patients were generally similar to the improvements between baseline and week 16 in the patients who received dupilumab in Part A
- Similar adverse effects were noted across all groups. There was an increased rate (at least 10%) of COVID infections in participants receiving dupilumab whereas the incidence of vomiting was at least 10 percentage points lower among patients who received dupilumab (either group) than among those who received placebo
My take: Dupilumab is an effective option for eosinophilic esophagitis.
Related blog posts:
- Dupixent Approved in Younger Children (15 kg+)
- “Real-World” Dupilumab for Eosinophilic Esophagitis
- Practical Tips for Eosinophilic Esophagitis
- Dupilumab: FDA Approval for Eosinophilic Esophagitis
- “Tug” Sign For Eosinophilic Esophagitis and EoE Bowel Sounds Tips
- When to Use Dupilumab for Eosinophilic Esophagitis: Multispecialty Guidelines
- According to the study which you would never qualify for… (2023)
- Landmark Dupilumab Study for Eosinophilic Esophagitis