Roughly 15 million people — six percent of adults in the United States — have metabolic dysfunction-associated steatohepatitis, known as MASH. Rates of the disease are rising…
Wegovy, which is a weekly injection, is now approved for adults with MASH and moderate-to-advanced levels of fibrosis, or excessive scar tissue in the liver. The drug is not intended for people with cirrhosis…
Wegovy will be a welcome addition to the options doctors can prescribe — as long as their patients can access them. The drug carries a list price of over $1,300 a month, although most people do not pay that full amount. Many people have lost insurance coverage for weight-loss drugs, as plans struggle to keep up with the costs.
Related review article:G Targher et al. NEJM 2025; 393: 683-698. Metabolic Dysfunction–Associated Steatotic Liver Disease. This review article succinctly covers the epidemiology, manifestations, disease progression and pivotal pharmacologic advances.
Methods: In this phase 3, multicenter, randomized, double-blind, placebo-controlled trial, the authors assigned 1197 patients with biopsy-defined MASH and fibrosis stage 2 or 3 in a 2:1 ratio to receive once-weekly subcutaneous semaglutide at a dose of 2.4 mg or placebo for 240 weeks
Key findings:
Resolution of steatohepatitis without worsening of fibrosis occurred in 62.9% of the 534 patients in the semaglutide group and in 34.3% of the 266 patients in the placebo group (P<0.001)
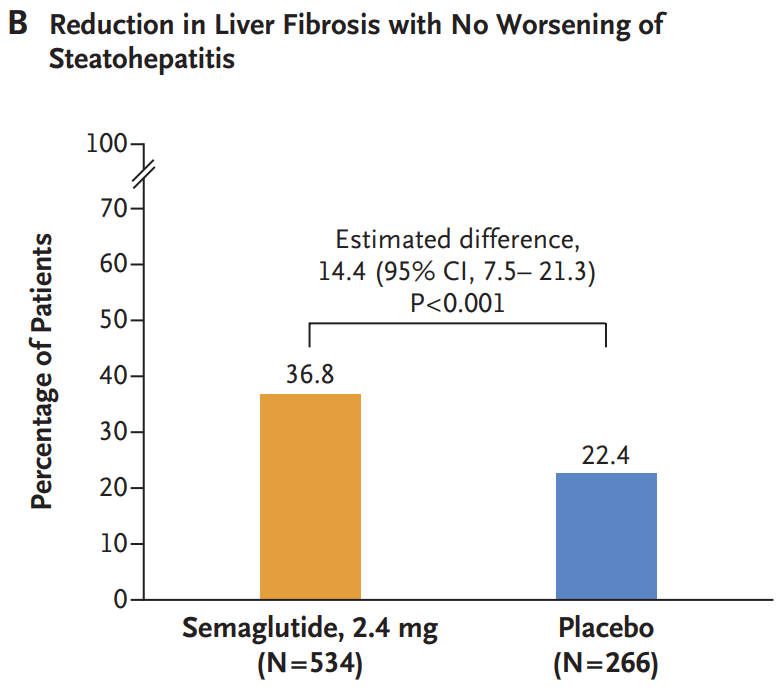
A reduction in liver fibrosis without worsening of steatohepatitis was reported in 36.8% of the patients in the semaglutide group and in 22.4% of those in the placebo group (P<0.001).
The mean change in body weight was −10.5% with semaglutide and −2.0% with placebo (P<0.001)
Gastrointestinal adverse events were more common in the semaglutide group. The incidence of acute pancreatitis was similar in the two groups: Nausea 290/800 (36.2%) vs. 52/395 (13.2%), Diarrhea 215/800 (26.9%) vs. 48/395 (12.2%), Constipation 178/800 (22.2%) vs. 33/395 (8.4%) and Vomiting 149/800 (18.6%) vs. 22/395 (5.6%)
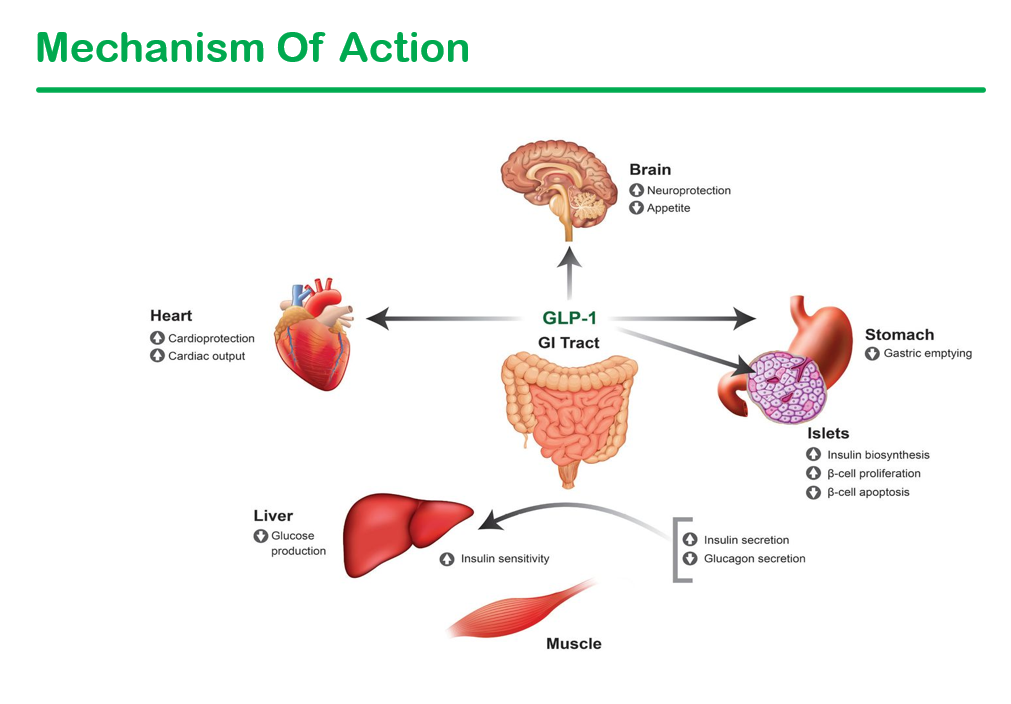
Semaglutide improved multiple cardiometabolic features, including glycemic control and insulin resistance. “These findings are important because metabolic dysfunction is an upstream event driving hepatic lipotoxicity and, subsequently, steatohepatitis and fibrogenesis. Thus, semaglutide treatment addressed the primary pathogenic driver of MASH”
Side effects leading to people dropping out of the trial were 2.6% for the semaglutide group and 3.3% for the placebo group
Discussion notes that “although semaglutide can be safely used in patients with cirrhosis, its efficacy in this population has not been established.”
My take: Semaglutide appears to be effective in patients with MASH.with stage 2 or 3 fibrosis.
“Let food be thy medicine” is a well-known phrase usually attributed to Hippocrates (though it is unclear if he said this). Regardless, this study indicates that added curcumin in the diet could be beneficial for steatotic liver disease.
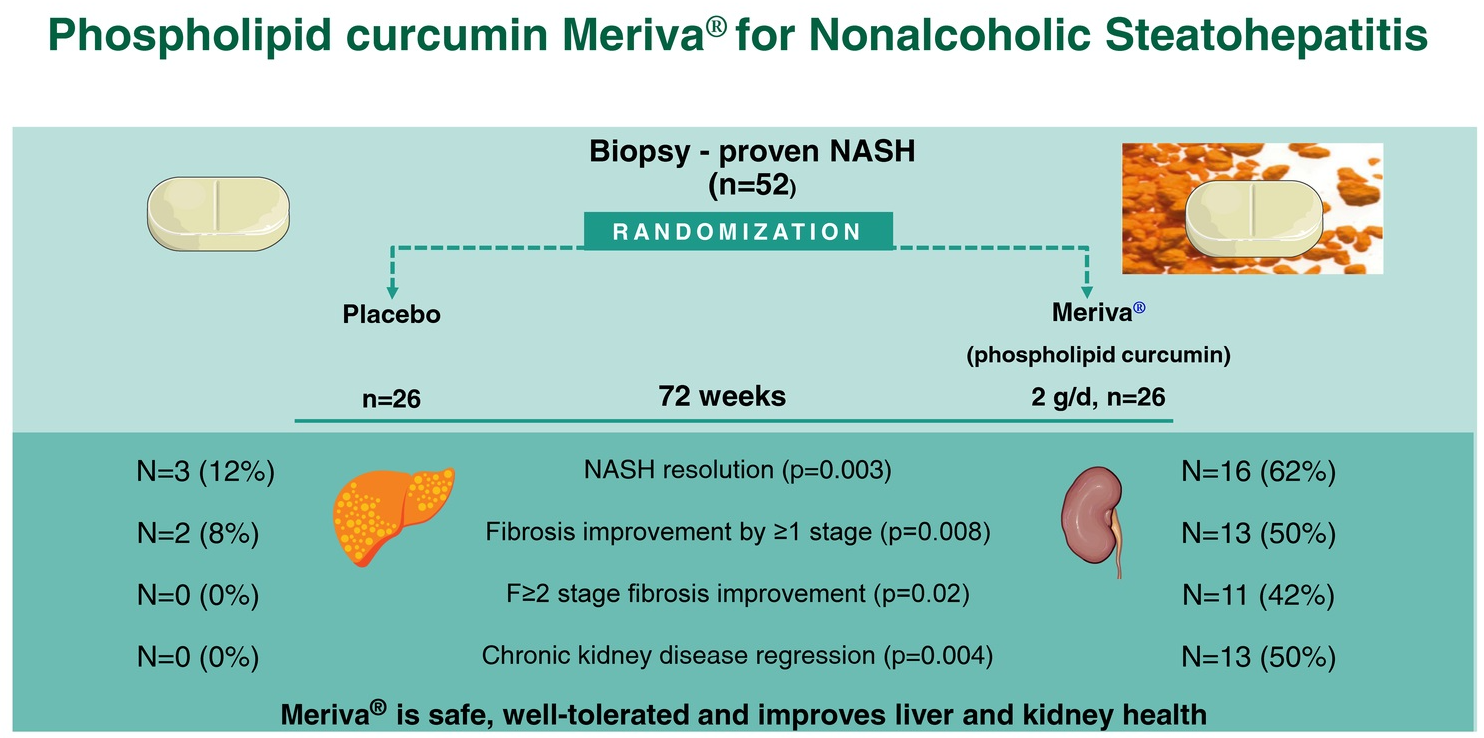
Methods: In this double-blind trial, 52 patients with biopsy-proven NASH (71% with stage ≥F2 fibrosis, 58% with stage A2-G2/A2-G3a chronic kidney disease) were randomized 1:1 to receive Meriva 2 g/d (1 g BID) or placebo for 72 weeks. Meriva is a formulation of curcumin extract with phospholipids that has improved oral bioavailability of curcumin metabolites.
Key findings:
Sixteen (62%) patients on Meriva (curcumin) versus 3 (12%) patients on placebo had NASH resolution (RR = 5.33)
hirteen (50%) patients on Meriva versus 2 (8%) patients on placebo had ≥1 stage fibrosis improvement (RR = 6.50)
Eleven (42%) patients on Meriva versus 0 (0%) on placebo had regression of significant liver fibrosis (RR = 18.01)
Thirteen (50%) patients on Meriva versus 0 (0%) on placebo had chronic kidney disease regression (RR = 10.71)
Compared with placebo, Meriva improved eGFR (difference in adjusted eGFR change: +3.59 [2.96–4.11] mL/min/1.73 m2/y, p = 0.009), fasting glucose(−17 mg/dL; 95% CI = −22, −12), HbA1c (−0.62%; 95% CI = −0.87%, −0.37%), LDL-C (−39 mg/dL; 95% CI = −45, −33), triglycerides (−36 mg/dL, 95% CI = −46, −26), HDL-C (+10 mg/dL; 95% CI = +8, +11), and inflammatory markers
The observed benefits were associated with downregulation of hepatic NF-kB which is a proinflammatory transcription factor and a known curcumin target
My take: A larger multicenter study is needed to confirm these promising results. This study shows that dietary changes and lifestyle modification remain important tools in treating MASH (aka NASH).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
GI and Hepatology News, Open Access: Watershed Moment’: Semaglutide Shown to Be Effective in MASH (November 2024): “At 72 weeks, a 2.4-mg once-weekly subcutaneous dose of semaglutide demonstrated superiority, compared with placebo, for the two primary endpoints: Resolution of steatohepatitis with no worsening of fibrosis and improvement in liver fibrosis with no worsening of steatohepatitis.”
“ESSENCE (NCT04822181) is an ongoing multicenter, phase 3 randomized, double-blind, placebo-controlled outcome trial studying semaglutide for the potential treatment of MASH.” Cohort: N=1200, biopsy-defined MASH and fibrosis, stages F2 and F3…”After initiation, the semaglutide dosage was increased every 4 weeks up to 16 weeks when the full dose (2.4 mg) was reached.”
Key findings:
62.9% of those in the semaglutide group and 34.1% of those in the placebo group reached resolution of steatohepatitis with no worsening of fibrosis.
37% of those in the semaglutide group and 22.5% of those in the placebo group had improvement in liver fibrosis with no worsening of steatohepatitis
Weight loss was also significant, with a 10.5% reduction in the semaglutide group compared with a 2% reduction in the placebo group
No new safety signals were identified
Cardiometabolic risk factors improved as well, with changes in blood pressure measurements, hemoglobin A1c scores, and cholesterol values.
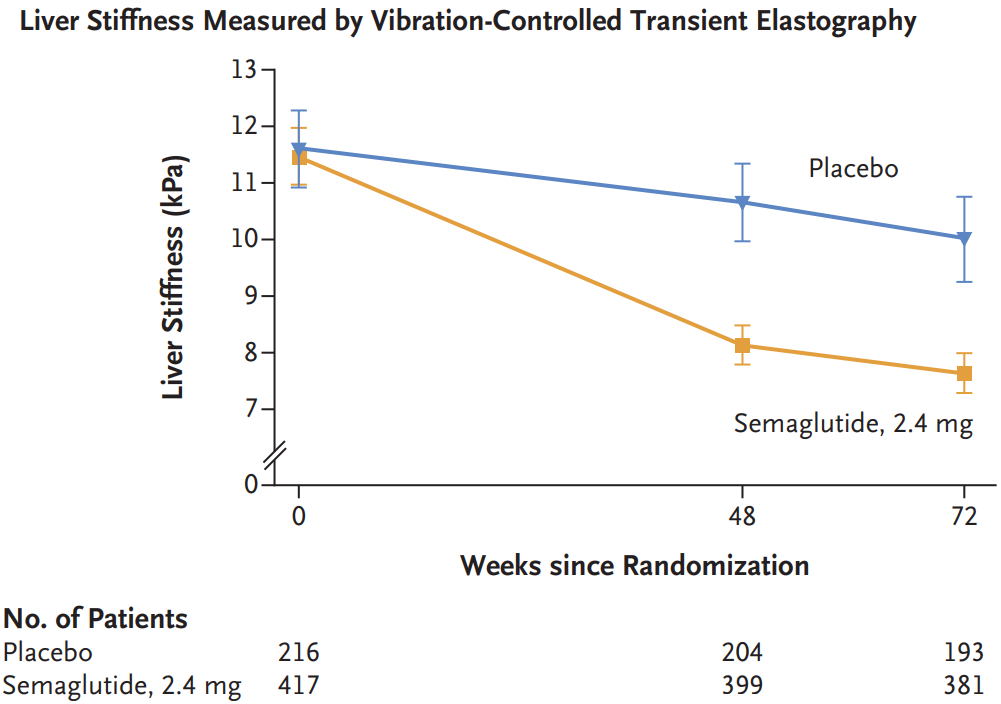
20%-40% improvements in liver enzymes and noninvasive fibrosis markers, such as ELF and vibration-controlled transient elastography liver stiffness.
My take: This expected finding indicates that more GLP-1 agents are likely to be approved for MASH treatment. Survodutide received “U.S. FDA Breakthrough Therapy” in October 2024.
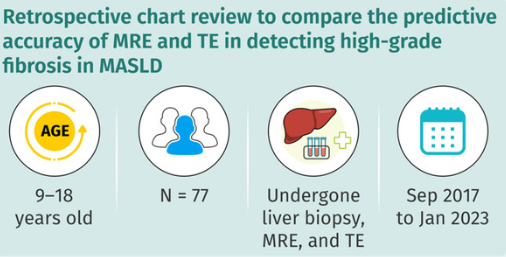
TE and MRE did not have high correlation with liver biopsy in the detection of high-grade fibrosis
Fibrosis was identified in 90% of liver biopsies with bridging fibrosis in 15 (19%) and cirrhosis in 1 (1%)
AUROC curves of MRE and TE for detection of high-grade fibrosis were 0.817 and 0.750, respectively, and not significantly different.
The authors note that previous adults studies suggest that MRE is more accurate in the identification of liver fibrosis than TE (MRE detected ≥ F1 fibrosis with an AUROC of 0.82, while TE detected fibrosis with an AUROC of 0.67).20
My take: Trying to identify accurate non-invasive testing is crucial to help identify patients most in need of treatment and for limiting costs.
“At 12 months, liver biopsies showed that a greater proportion of subjects who were treated with Rezdiffra achieved NASH resolution or an improvement in liver scarring as compared with those who received the placebo. A total of 26% to 27% of subjects who received 80 milligrams of Rezdiffra and 24% to 36% of subjects who received 100 milligrams of Rezdiffra experienced NASH resolution and no worsening of liver scarring, compared to 9% to 13% of those who received placebo and counseling on diet and exercise…n addition, a total of 23% of subjects who received 80 milligrams of Rezdiffra and 24% to 28% of subjects who received 100 milligrams of Rezdiffra experienced an improvement in liver scarring and no worsening of NASH, compared to 13% to 15% of those who received placebo, depending on each pathologist’s readings.”
“The most common side effects of Rezdiffra included diarrhea and nausea. Rezdiffra comes with certain warnings and precautions, such as drug-induced liver toxicity and gallbladder-related side effects. Use of Rezdiffra should be avoided in patients with decompensated cirrhosis.”
My take: It is good to finally have an FDA-approved medication for MASH (in adults). My speculation is that medications which achieve persistent weight loss will have a more pronounced effect on liver health and overall health.
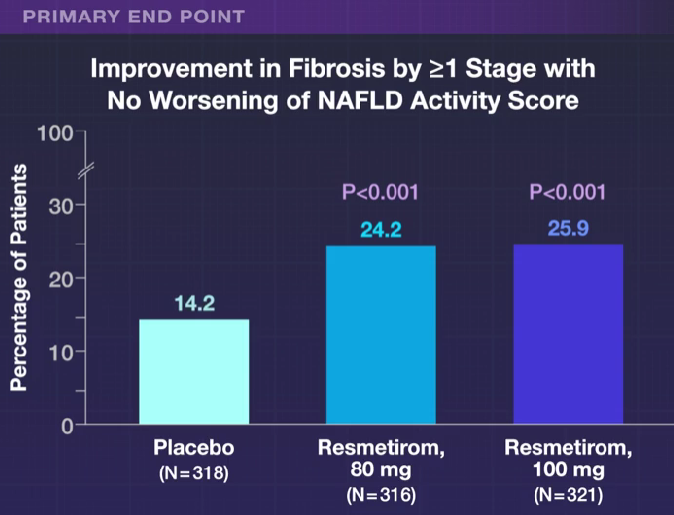
SA Harrison et al. NEJM 2024; 390: 497-509. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis
This “MAESTRO-NASH” study enrolled 966 adult patients biopsy-confirmed NASH (now termed MASH) and a fibrosis stage of F1B, F2, or F3. Approximately 60% of each arm had F3 fibrosis. Patients were randomly assigned in a 1:1:1 ratio to receive once-daily d resmetirom at a dose of 80 mg or 100 mg or placebo; Resmetirom is an oral, liver-directed, thyroid hormone receptor beta–selective agonist.
Key findings:
MASH “resolution with no worsening of fibrosis was achieved in 25.9% of the patients in the 80-mg resmetirom group and 29.9% of those in the 100-mg resmetirom group, as compared with 9.7% of those in the placebo group (P<0.001)”
“Fibrosis improvement by at least one stage with no worsening of the NAFLD activity score was achieved in 24.2% of the patients in the 80-mg resmetirom group and 25.9% of those in the 100-mg resmetirom group, as compared with 14.2% of those in the placebo group (P<0.001)”
“Levels of a broad range of atherogenic lipids and lipoproteins, including LDL cholesterol, non-HDL cholesterol, triglycerides, apolipoprotein B, and lipoprotein(a), appeared to be reduced by resmetirom relative to placebo, findings consistent with those of earlier studies.18,19“
Diarrhea and nausea were more frequent in the resmetirom group compared to placebo, though there were no differences in serious adverse effects. Patients in the 100 mg group were more likely to discontinue treatment (~7%) compared to 2% in the other two groups.
“In this trial, achievement of a 30% reduction in hepatic fat (MRI-PDFF) or a 120% increase in the sex hormone–binding globulin level appeared to be associated with biopsy responses.”
In their discussion, the authors note that “Noninvasive testing to identify patients with NASH for treatment and to monitor treatment response will be important in clinical practice in which liver biopsy is infrequently used.”
The associated editorial by Kenneth Cusi (pg 559-561) notes the following:
Resmetirom had neutral effects on body weight and insulin resistance.
“Treatment affected the pituitary–thyroid hormone axis, with prohormone free T4 levels decreasing by approximately 17 to 21% and mean thyrotropin levels also decreasing.” It is unclear if this has any long-term significance (long-term data needed). ”Careful surveillance to detect early endocrine disease that is related to potential thyroid, gonadal, or bone disease appears warranted to avoid any potential risks from long-term treatment.”
When subtracting the placebo effect, he notes that “approximately 2 of 10 patients treated will have NASH resolution and approximately 1 of 10 patients treated will have fibrosis improvement.” Thus, combination therapy may be needed.
My take: This study brings us a step closer to having a medication which can improve MASH as currently there are no FDA-approved medications. My speculation is that medications which achieve persistent weight loss will have a more pronounced effect on liver health and overall health.
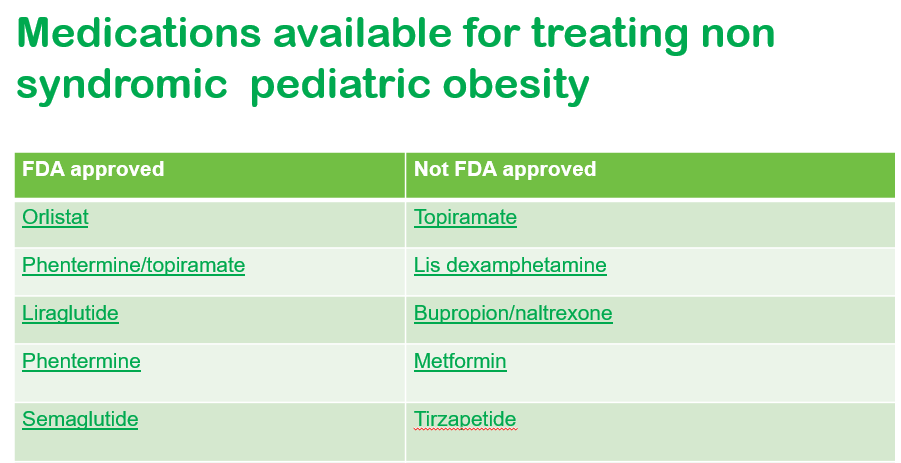
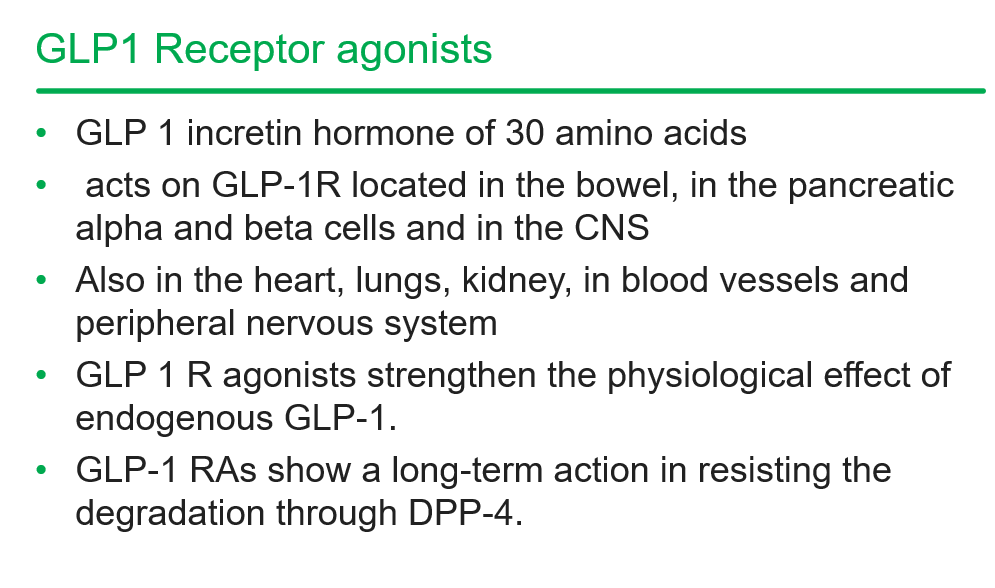
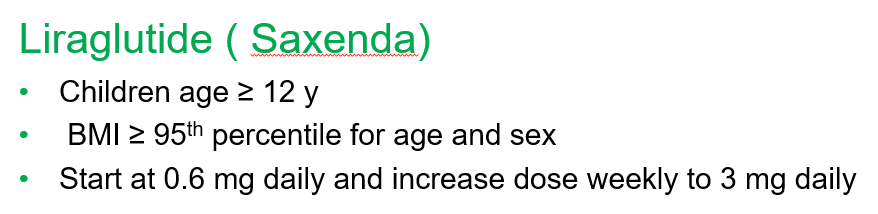
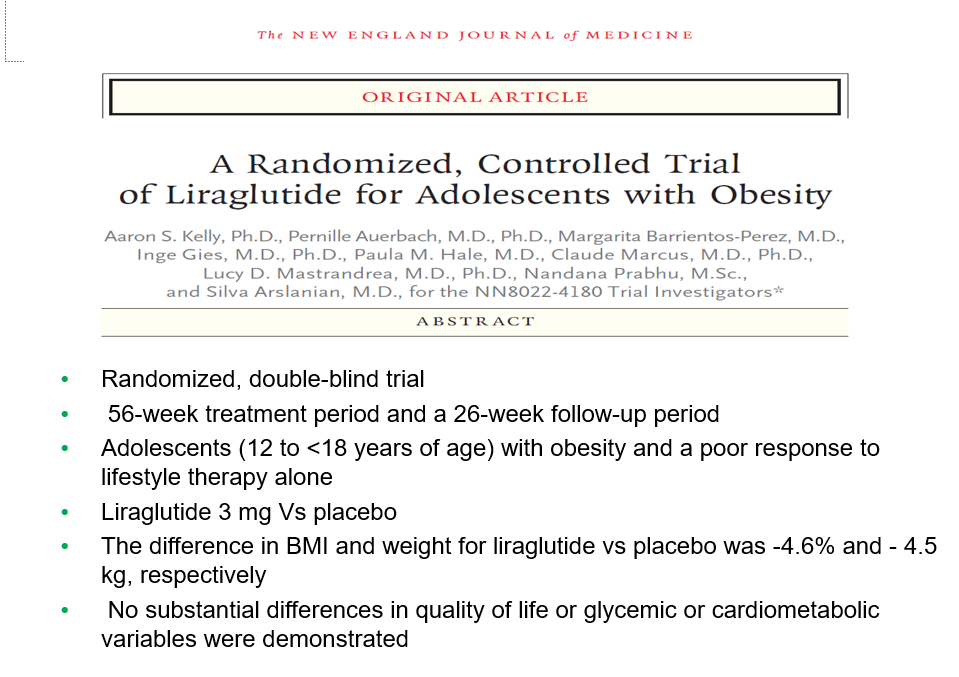
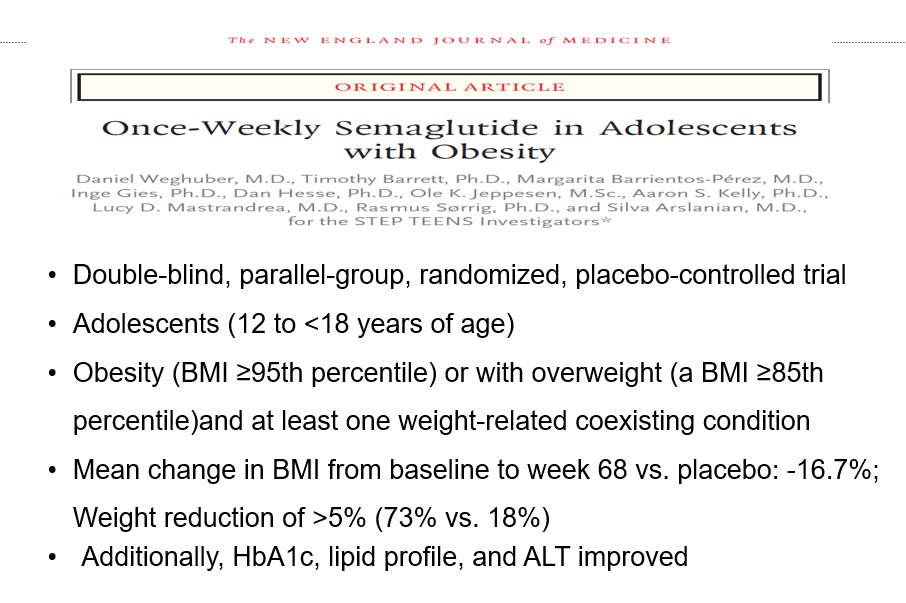
Recently, Dr. Shruthi Arora, an Emory Pediatric Endocrinologist and part of CHOA’s Strong4Life team, provided a terrific review of pediatric obesity pharmacology for our group.
Here are a few slides from Dr. Arora’s lecture:
General points from this lecture:
GLP-1 agents are a huge advance but currently limited by affordability (frequently there is a lack of insurance coverage if there is not T2DM) and availability. In addition, most individuals will regain weight loss when these agents are stopped.
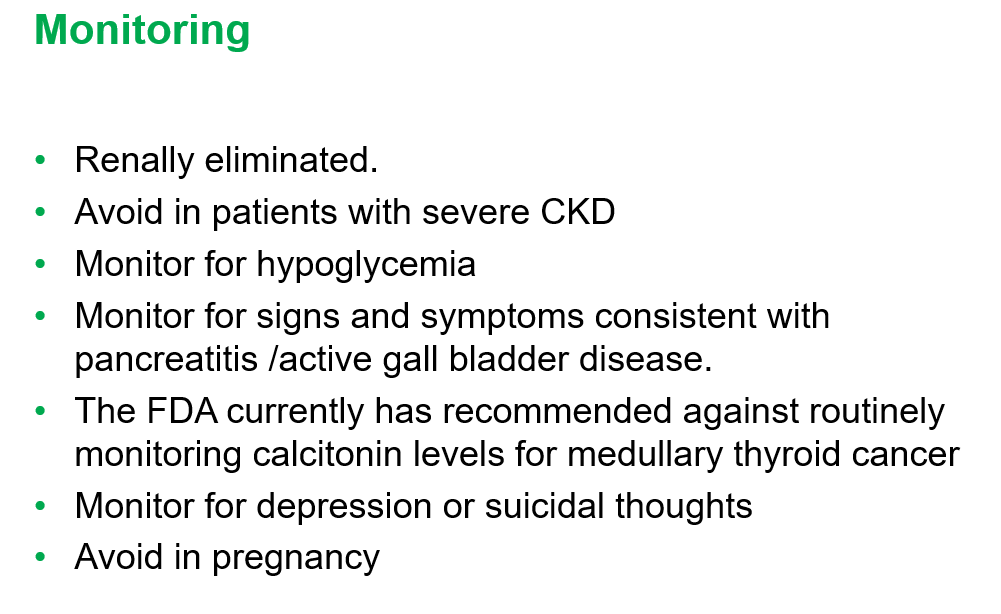
GLP-1 agents are not recommended in the following: patients with gastroparesis, and patients with a personal or family history significant for MEN 2 A /MEN 2 B/ Medullary thyroid cancer
Long-term data is still needed. These agents have been associated with muscle and bone loss; thus, working to assure a good diet is still very important
——————————————————————————
NASPGHAN has a good review/webinar on this topic as well: Pediatric MASLD in the Current Era of Pharmacological and Surgical Obesity Treatment Options. For members, after sign in, you can register and login to this webinar (look under clinical practice tab). This webinar made a lot of useful points (many covered by Dr. Arora too).
For GLP-1 agents, due to effects on gastric emptying, they are generally held prior to anesthesia. If they are given weekly, then hold 1 week prior to anesthesia. If it is a daily medication, hold for 1 day prior to anesthesia.
Surgery definitely helps improve MASH -though variable responses in patients. SLEEVE gastrectomy is currently the most frequent bariatric surgery
There is trouble getting GLP-1 medications.
Limited knowledge regarding long-term effects of cycling of GLP-1 agents.
Obesity is a long-term disease –>anticipate long-term treatment
The Wall Street Journal recently published a personal account of using the newer obesity medications. Bradley Olson, 1/12/24: A Weight-Loss Drug Changed My Life. Will It Solve My Problem? (behind a paywall). This article discusses the dramatic improvement experienced by the writer along with his concerns about the cost of the medication and potential for rebound when he can no longer afford it. Two of the figures:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
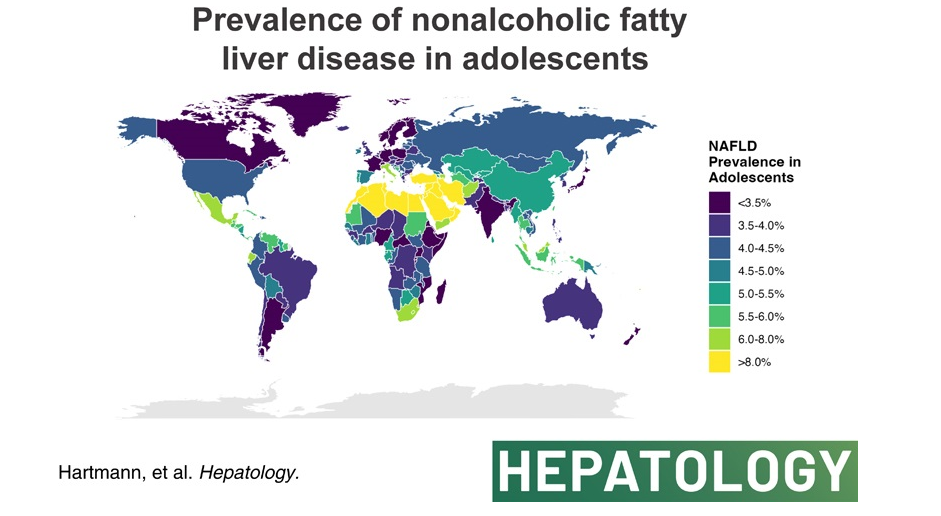
The authors analyzed data from the Global Burden of Disease Study 2019 to compare global, continental, and national prevalence rates of adolescent (15-19 yrs of age) NAFLD.
Key finding:
The global NAFLD prevalence in adolescents increased from 3.73% in 1990 to 4.71% in 2019 (a relative increase of 26.27%). NAFLD is now termed metabolic dysfunction-associated steatotic liver disease (MASLD).
High body mass index and not type 2 diabetes mellitus correlated with NAFLD prevalence in adolescents globally.
In the associated editorial (S Xanthakos, Hepatology78(4):p 1017-1019, October 2023, Rising tide of NAFLD in youth: A warning bell and call to action), some of the key points:
“The Global Burden of Disease (GBD) Study is the most comprehensive and long-standing effort to systematically and scientifically collate data on hundreds of diseases and injuries across the globe, including related clinical outcomes. Beginning in 1990, the GBD Study initially collected data on 106 conditions and 10 risk factors, across 5 age groups.1 Over time, the GBD Study has expanded through serial iterations to involve >9000 international researchers collecting data on 369 diseases and injuries across 204 countries and territories in the most recent 2019 report.1“
” From the GBD Study, we learned that NAFLD is the most rapidly rising cause of chronic liver disease in adolescents and adults,2 and the fastest-growing contributor to cirrhosis, liver cancer, and liver-related deaths globally.”
“The global prevalence of NAFLD in adolescents shows no sign of abating, rather has continued to increase steadily from 3.7% in 1990 to 4.7% in 2019.”
“As with all epidemiological research, the GBD study faces the primary limitation of relying on data sources that employ varying and less accurate measures of NAFLD prevalence (alanine aminotransferase and/or ultrasound primarily). However, the rigorous methodological approach employed by the GBD including frequent assessment of face validity, and the tremendous input of data sources (>80,000 in 2019) nonetheless results in the most comprehensive global data set available.”
My take (borrowed from editorial): Without intervention, “the increase in adolescent NAFLD certainly portends a future increase in NAFLD-related cirrhosis and liver-related deaths in young adults in the coming decades, and a likely escalation in cardiovascular and diabetes-related morbidity.
This article offers best practice advice -here are two of them:
#2: A Fibrosis 4 Index score <1.3 is associated with strong negative predictive value for advanced hepatic fibrosis and may be useful for exclusion of advanced hepatic fibrosis in patients with NAFLD.
#8 Patients with NAFLD and NITs (noninvasive tests) results suggestive of advanced fibrosis (F3) or cirrhosis (F4) should be considered for surveillance of liver complications (eg, hepatocellular carcinoma screening and variceal screening per Baveno criteria). Patients with NAFLD and NITs suggestive of advanced hepatic fibrosis (F3) or (F4), should be monitored with serial liver stiffness measurement; vibration controlled transient elastography; or magnetic resonance elastography, given its correlation with clinically significant portal hypertension and clinical decompensation.
In this study from U.S., patients (n=2523) were divided into three categories based on FIB-4 scores: (A) Fibrosis-4 (FIB-4) <1.3 and/or liver-stiffness measurement (LSM) measured by Fibroscan <8 kp, (B) FIB-4 1.31‒2.6 and/or LSM 8.1-12.5 kp, and (C) FIB-4 >2.6 and/or LSM >12.5 kp. However, those in class A with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3, or class B with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3 were upstaged by one class. The data were reviewed retrospectively from a prospective longitudinal cohort (TARGET-NASH)
Key findings: All adverse outcomes including liver and cardiovascular (see below) were correlated with FIB-4 staging.
Key findings: The prevalence of steatosis, severe steatosis, advanced fibrosis, and cirrhosis was 44.39%, 10.57%, 2.85%, and 0.87%, respectively in Chinese adults
Limitation: This data was derived from a health checkup cohort which could give different results than a random population sampling. Patients at health checkups may be more health conscious and/or be aware of underlying health concerns.
Prevalence of different grades of liver fibrosis in different age groups.
My take: Steatotic liver disease is a huge worldwide problem. The growing prevalence is going to result in extensive health issues.
—————
This year’s pumpkin 910/31/23):
It does not look like I will become a professional pumpkin artist anytime soon!