Methods: A longitudinal cohort study was conducted among healthy children 0-10 years of age participating in The Applied Research Group for Kids study between June 2008 and August 2019 in Toronto, Canada.
Key findings:
Of 8943 children included, the mean (SD) age of infant cereal introduction was 5.7 (2.1) months
Children who were introduced to infant cereal at 4 vs 6 months had 0.17 greater body mass index z score (95% CI 0.06-0.28; P = .002) and greater odds of obesity (OR 1.82; 95% CI 1.18-2.80; P = .006) at 10 years of age.
Earlier cereal introduction was associated with a less-favorable eating behavior score at 18 months to 5 years of age (0.18 units higher; 95% CI 0.07-0.29; P = .001).
Limitation: This study did not randomize children into early vs late cereal introduction; thus, there may be unidentified confounders that contribute to weight gain in children offered cereal at a younger age.
My take: This study indicates that introduction of cereal at 6 months of age, rather than 4 months of age, may be beneficial in limiting excess weight gain.
Key points from this review of more than 200 relevant meta-analyses and individual studies:
“A weight-neutral approach to treating obesity-related health conditions may be as, or more, effective than a weight-loss-centered approach, and could avoid pitfalls associated with repeated weight loss failure… Epidemiological studies show that CRF (cardiorespiratory fitness) and PA (physical activity) significantly attenuate, and sometimes eliminate, the increased mortality risk associated with obesity. More importantly, increasing PA or CRF is consistently associated with greater reduction in risk of all-cause and CVD mortality than intentional weight loss.”
“The increased prevalence of weight loss attempts in the United States has coincided with the increased prevalence of obesity. Thus, a weight-centric approach to obesity treatment and prevention has been largely ineffective. It is unlikely that continued focus on weight loss as the primary metric for success will reverse the trends in obesity prevalence or result in sustainable weight loss. In fact, chronic weight cycling is the norm for millions of adults and is likely to remain so for as long as weight loss persists as the cornerstone of obesity treatment. Weight cycling is associated with health risks that are very similar to those associated with obesity, including higher all-cause mortality risk, and may contribute to weight gain.”
Figure 2 from article: “Joint associations between cardiorespiratory fitness (CRF), body mass index (BMI), and all-cause (top) and cardiovascular disease (CVD) (bottom) mortality. Hazard ratios reflect the pooled data from the meta-analyses of Barry et al. for all-cause mortality (Barry et al., 2014) and cardiovascular disease mortality (Barry et al., 2018). For all-cause mortality, the meta-analysis included 6 cohorts of men only, 2 cohorts of women only, and 2 cohorts of both men (~80%) and women. For CVD mortality, the meta-analysis included 8 cohorts of men only and 1 cohort of both men (89%) and women”
This study examined population risks for esophageal squamous cell carcinoma (ESCC), esophageal adenocarcinoma (EAC), gastric cardia adenocarcinoma (GCA), and gastric noncardia adenocarcinoma (GNCA).
“We prospectively examined the associations for risk factors and these cancers in 490,605 people in the National Institutes of Health-the American Association of Retired Persons Diet and Health cohort Diet and Health Study cohort from 1995 to 2011.”
Key findings:
My take: Tobacco, Obesity and Alcohol are associated with increased risk for a large proportion of esophageal and gastric cancers in the United States
The IPTW (inverse probability of treatment weighting)-adjusted risk of any cancer and obesity-related cancer was reduced by 18% (hazard ratio, 0.82; 95% CI, 0.76–0.89) and 25% (hazard ratio, 0.65; 95% CI, 0.56–0.75), respectively, in patients with versus without bariatric surgery.
In cancer-specific models, bariatric surgery was associated with significant risk reductions for colorectal, pancreatic, endometrial, thyroid cancers, hepatocellular carcinoma, and multiple myeloma.
Methods: Data from 6 ustekinumab phase 2/3 CD and UC studies were pooled, and safety was evaluated through 1 year; this included 2574 patients (1733 patient-years of follow-up)
Key Safety findings –Events per 100 patient years -placebo vs ustekinumab respectively:
Major cardiovascular events were rare with 2 in placebo group 0.34 and 2 in the ustekinumab group 0.12
Morekey findings:
No cases of progressive multifocal leukoencephalopathy or reversible posterior leukoencephalopathy
Antibodies to ustekinumab were identified in 3.6% of patients
My take: This study showed similar safety between ustekinumab and placebo, but is limited by short followup. The authors note that 5-year data from ustekinumab’s use with psoriasis has found no safety signals for malignancy.
“The U.S. Food and Drug Administration approved Wegovy (semaglutide) injection (2.4 mg once weekly) for chronic weight management in adults with obesity or overweight with at least one weight-related condition (such as high blood pressure, type 2 diabetes, or high cholesterol), for use in addition to a reduced calorie diet and increased physical activity…The drug is indicated for chronic weight management in patients with a body mass index (BMI) of 27 kg/m2 or greater who have at least one weight-related ailment or in patients with a BMI of 30 kg/m2 or greater… The largest placebo-controlled trial enrolled adults without diabetes. Individuals who received Wegovy lost an average of 12.4% of their initial body weight compared to individuals who received placebo”
In the 1990s, the combination of fenfluramine/phentermine was popularized as a treatment for obesity. Fenfluarmine, though, was shown to cause potentially fatal pulmonary hypertension and heart valve problems, which eventually led to its withdrawal and legal damages of over $13 billion (per Wikipedia: fenfluramine/phentermine).
Now, glucagon-like peptide-1 (GLP-1) receptor agonists, like liraglutide, are showing promise as agents to promote weight loss, primarily by inhibiting appetite. JR Lundrgen et al (NEJM 2021; 384: 1719-1730. Healthy Weight Loss Maintenance with Exercise, Liraglutide, or Both Combined) show that liraglutide can promote weight loss, especially if combined with exercise.
Methods: After an 8-week low-calorie diet, participants were randomly assigned for 1 year to one of four strategies: a moderate-to-vigorous–intensity exercise program plus placebo (exercise group); treatment with liraglutide (3.0 mg per day-SC injection) plus usual activity (liraglutide group); exercise program plus liraglutide therapy (combination group); or placebo plus usual activity (placebo group)
Key findings:
After the 8-week low-calorie diet, 195 participants had a mean decrease in body weight of 13.1 kg.
At 1 year, all the active-treatment strategies led to greater weight loss than placebo: difference in the exercise group, −4.1 kg (95% confidence interval [CI], −7.8 to −0.4; P=0.03); in the liraglutide group, −6.8 kg (95% CI, −10.4 to −3.1; P<0.001); and in the combination group, −9.5 kg (95% CI, −13.1 to −5.9; P<0.001). The combination strategy led to greater weight loss than exercise (difference, −5.4 kg; 95% CI, −9.0 to −1.7; P=0.004) but not significantly more than monotherapy with liraglutide (−2.7 kg; 95% CI, −6.3 to 0.8; P=0.13)
The side effects of decreased appetite, dizziness, increased heart rate and palpitations were more common in those receiving liraglutide; palpitations were evident in 12% of the liraglutide monotherapy group and 4% of the combination (with exercise) group.
The details of the exercise program are detailed in the methods section; all participants were assigned an instructor and expected to do a minimum of 150 minutes per week of moderate-intensity aerobic physical activity or 75 minutes per week of vigorous-intensity aerobic physical activity.
These results are similar to the 15% weight loss noted at 68 weeks with the GLP-1 receptor agonist semaglutide.
My take: GLP-1 receptor agonists help individuals lose weight. However, we’ve seen the promise of medical therapy before so we will have to see how the story ends.
Briefly noted: YY Gibbens et al. American Journal of Gastroenterology 2021 April 22. Effects of Central Obesity on Esophageal Epithelial Barrier Function. Key finding: Obesity+/GER- group demonstrated increased intercellular space, reduced desmosome density, and increased fluorescein leak compared with control subjects. Thus, obesity may worsen esophageal disease by impairing the structural and functional integrity of the esophageal barrier independent of GER. (Thanks to Mike Hart for this reference)
In The Shawshank Redemption, Andy Dufresne (Tim Robbins) manages to escape prison by crawling through 500 yards of a filthy sewage pipe. It seems like a similar effort will be needed to find out how to benefit from fecal transplantation when given for problems like irritable bowel syndrome and metabolic disease/obesity. Some recent studies and associated editorials are noted below.
Key finding: At week 12, 56% of patients given donor stool reported improvement in both primary endpoints compared with 26% of patients given placebo (P = .03).
This editorial stresses that trials of FMT in IBS have had inconsistent results and risks are unclear. “How many clinicians inform patients receiving FMT that the donor microbiota might include components that increase (or decrease) one’s risk of colorectal cancer?” Part of the problem is “due, in part, because a normal microbiome has not been defined.”
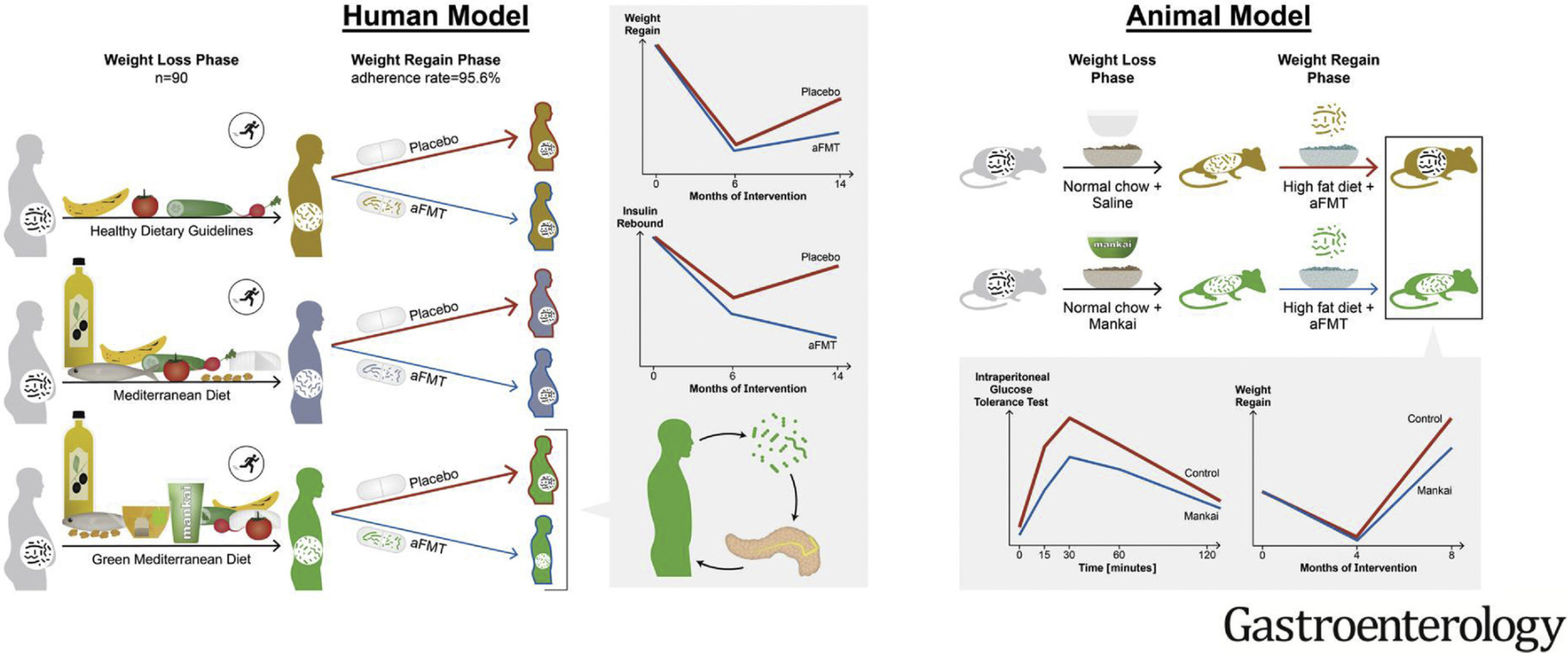
In this randomized controlled trial with 90 participants, autologous FMT (aFMT) significantly attenuated weight regain in the green-Mediterranean group (aFMT, 17.1%, vs placebo, 50%; P = .02) and improved insulin resistance: insulin rebound (aFMT, –1.46 ± 3.6 μIU/mL vs placebo, 1.64 ± 4.7 μIU/mL; P = .04) (Graphical abstract below)
In mice, Mankai-modulated aFMT in the weight-loss phase compared with control diet aFMT, significantly prevented weight regain and resulted in better glucose tolerance during a high-fat diet–induced regain phase (all, P < .05).
“These findings add support to the current body of evidence that the gut microbiota have a role in weight gain and metabolism. However, many questions remain. Indeed, although studies have shown varying degrees of effectiveness of FMT in the improvement of metabolic parameters in human participants, there has been no evidence yet that FMT can induce weight loss in obese patients.”
“The finding that maintenance of weight loss was only seen in the one dietary group consuming the Mediterranean diet plus green tea and Mankai supplement who received autologous FMT, would suggest that specific microbial profiles may be involved and that weight loss per se may not result in the required microbial profiles.”
Figure 1 from editorial: Challenges associated with the use of fecal microbial transplantation (FMT) as treatment
My take: Both of these studies show that modulation of the fecal microbiome may be helpful under the right set of circumstances to help with both irritable bowel syndrome and metabolic syndrome. However, ‘hundreds of yards’ of more research is needed to determine if this is really feasible and to assure that the benefits outweigh the potential risks.
Methods: Single course of oral encapsulated fecal microbiome from 4 healthy lean donors or saline placebo.
Key findings:
In this randomized, double-masked, placebo-controlled trial of 87 adolescents with obesity, FMT alone did not lead to weight loss at 6 weeks.
There were no observed effects on insulin sensitivity, liver function, lipid profile, inflammatory markers, blood pressure, total body fat percentage, gut health, and health-related quality of life
In post-hoc exploratory analyses among participants with metabolic syndrome at baseline, FMT led to greater resolution of this condition (18 to 4) compared with placebo (13 to 10) by 26 weeks (adjusted odds ratio, 0.06; 95% CI, 0.01-0.45; P = .007)