This blog entry has abbreviated/summarized these presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Here is a link to postgraduate course syllabus: NASPGHAN PG Syllabus – 2017
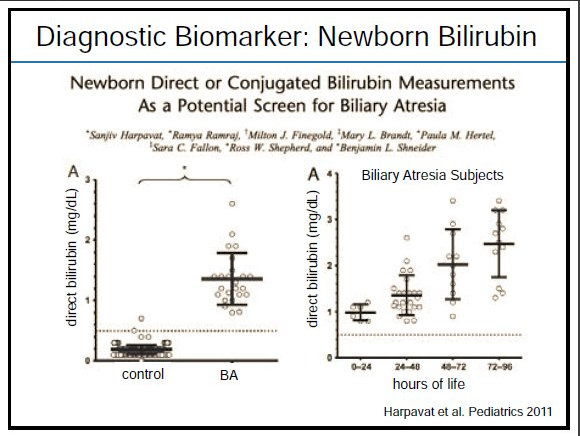
Biliary Atresia: Update on diagnostic and prognostic biomarkers and therapeutic interventions
Cara Mack Children’s Hospital of Colorado
Key points:
- 84% of biliary atresia is isolated; 16% are syndromic with other defects
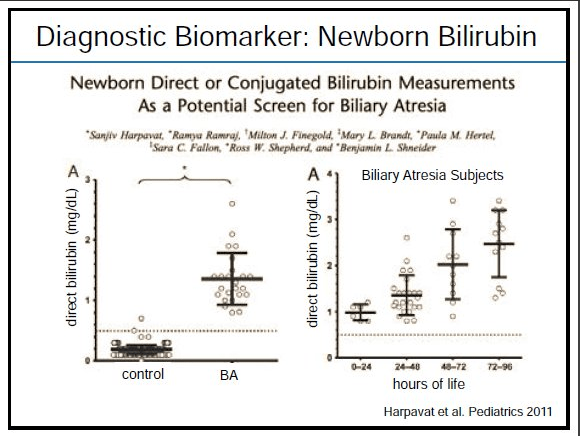
- Direct bilirubin is (mildly) elevated at birth in patients with biliary atresia
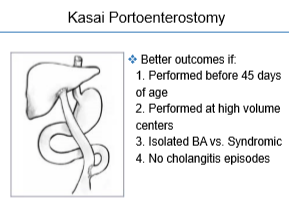
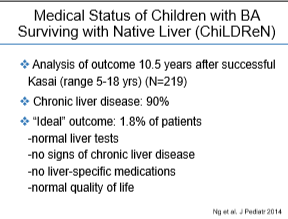
- Total bilirubin 3 months after Kasai predicts outcome. If <2 mg/dL, then unlikely to need a transplant in the first 2 years of life.
- Reviewed biomarkers including Th1, Autotaxin, IL-8

Therapeutic interventions:
- Nutritional support. Better nutrition improves outcomes after liver transplantation.
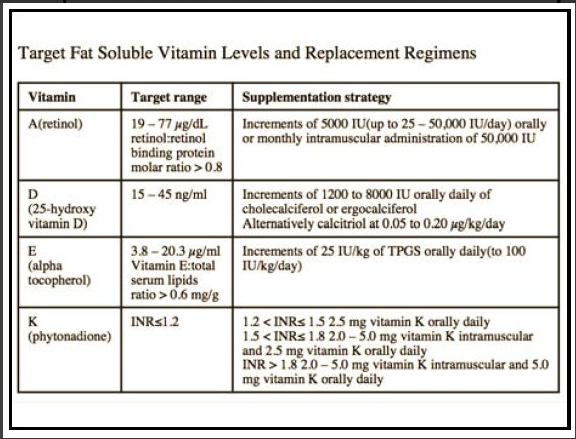
- Fat soluble vitamin supplementation
- Cholangitis prevention. Some studies have shown that prophylactic antibiotics may reduce incidence of cholangitis.
- No therapeutic interventions that delay progression of this disease

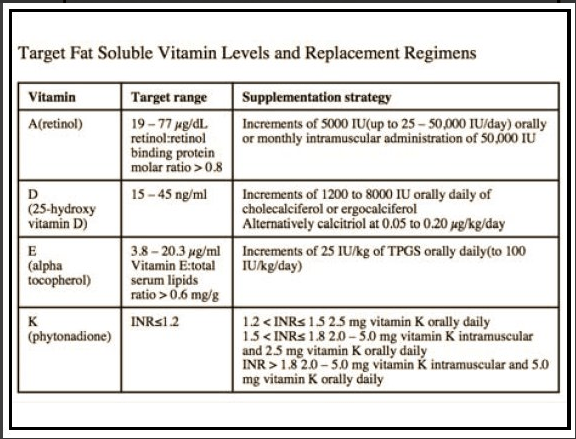
CHILDREN Cohort Mgt of Vitamin Supplementation
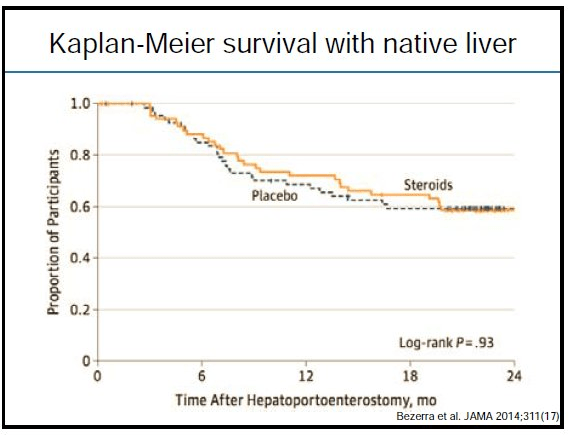
Steroids are not helpful after Kasai procedure
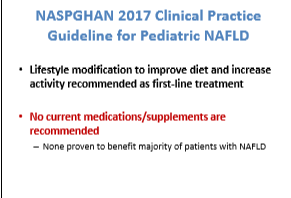
Diagnosis and Management of Pediatric NAFLD 2017
Stavra Xanthokos Cincinnati Children’s Hospital Medical Center
Key points:
- NAFLD is #2 cause of liver transplantation in adults and on its way to becoming #1
- ALT is still the best screening tool; NASPGHAN guidelines recommends screening overweight/obese children 9-11 years of age
- Ultrasound has poor sensitivity and specificity for NAFLD; it is helpful for detecting gallbladder disease
- Bariatric surgery has been effective for NAFLD



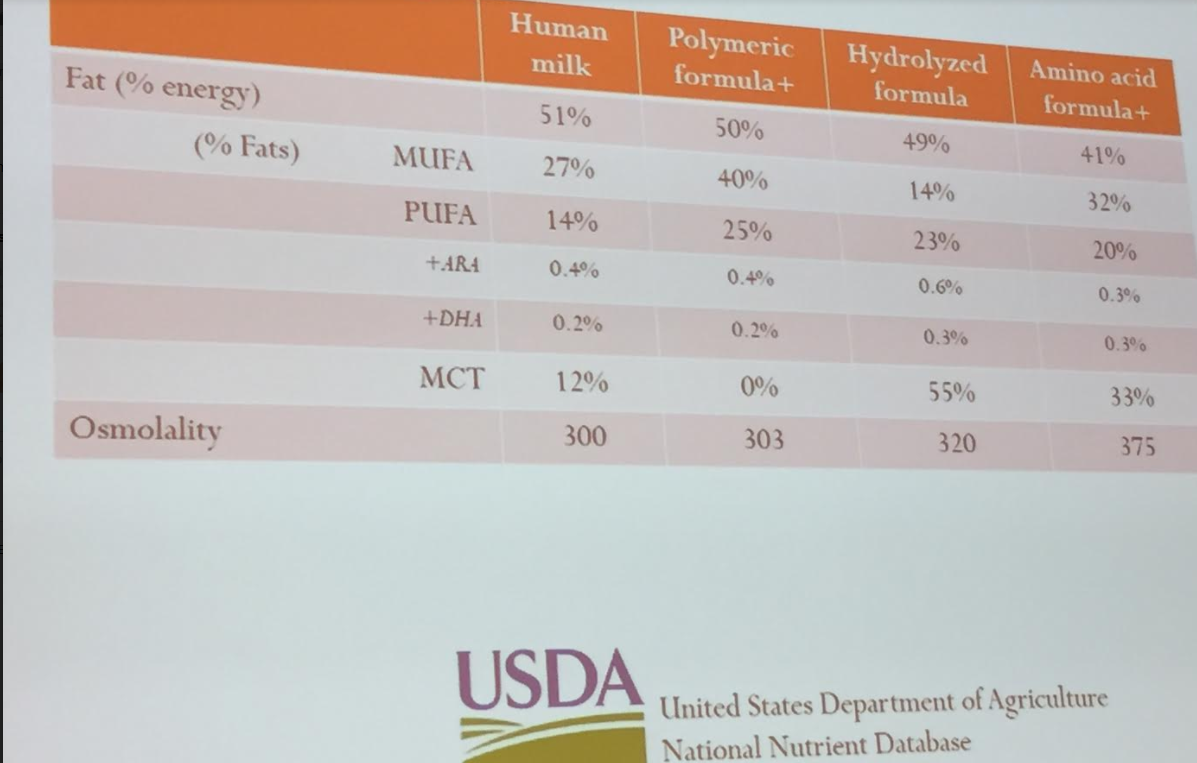
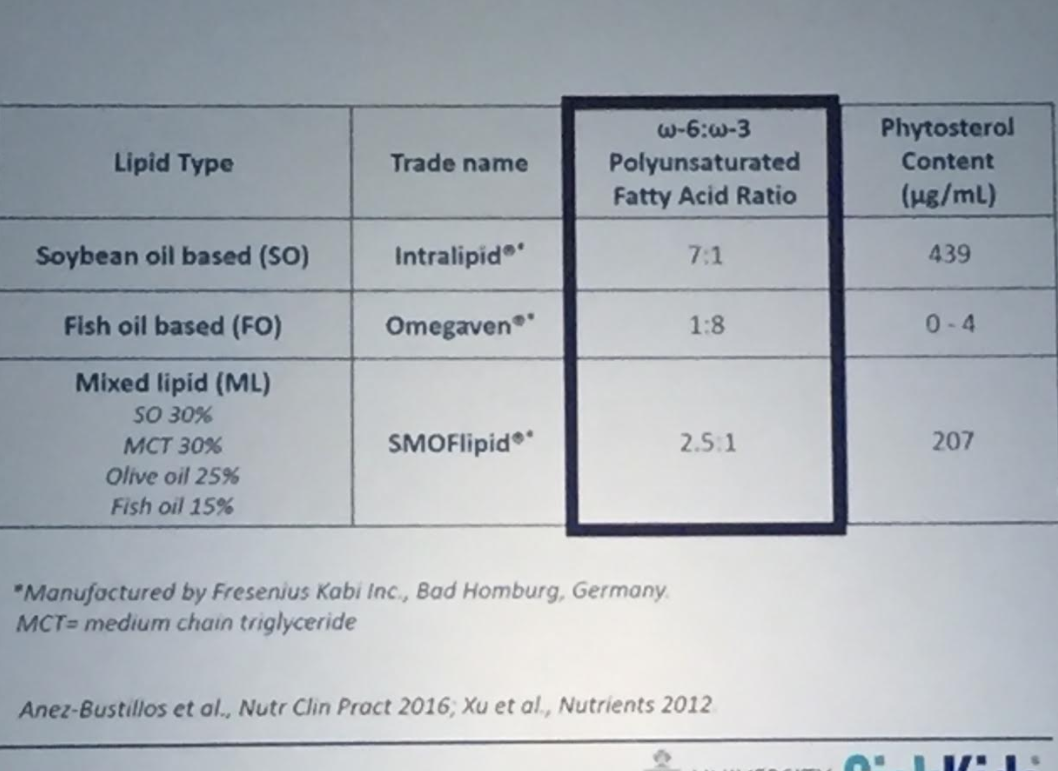
SMOFlipid and the Pediatric Patient
Peter Wales Hospital for Sick Children (Toronto)
Slides are not available in syllabus
Key points:
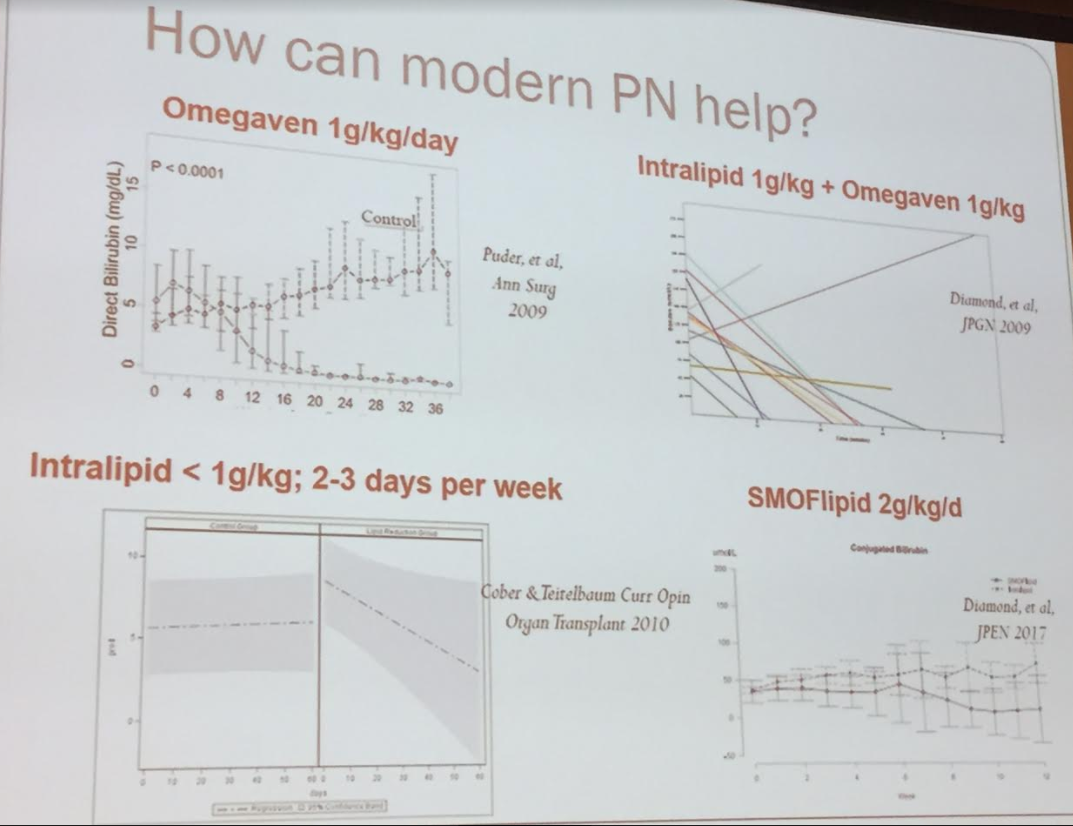
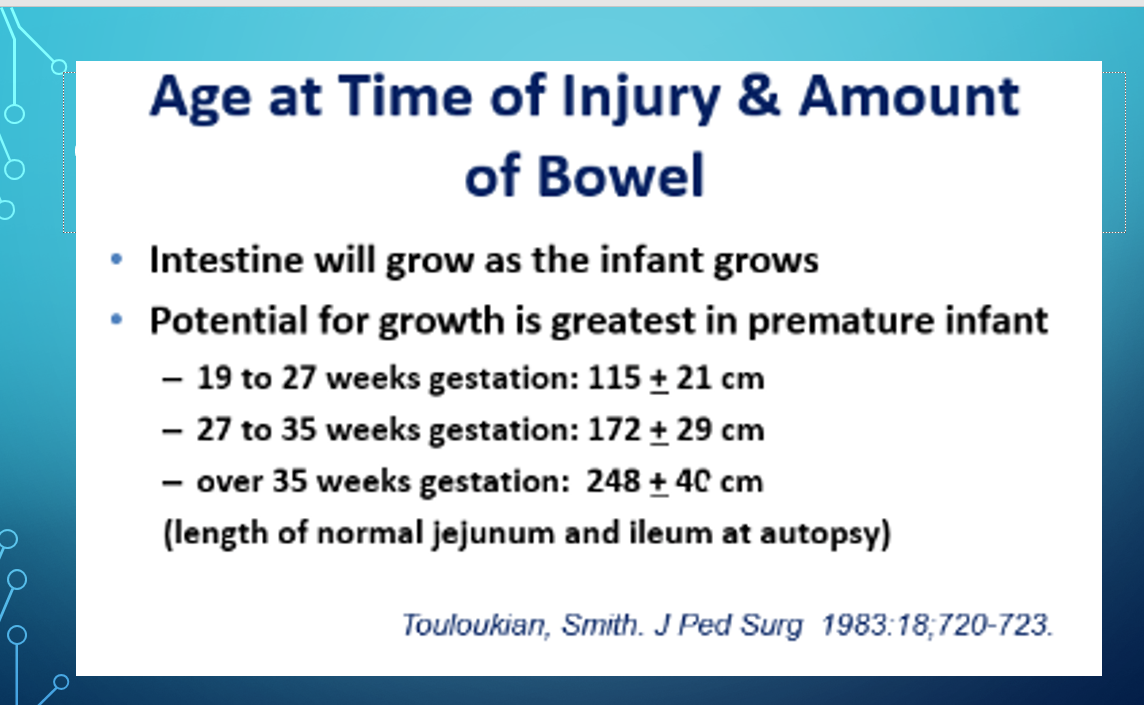
- Improving outcomes noted in the intestinal failure population
- Dr. Wales reviewed proposed improvements with Omega-3 lipids -less cholestasis, less hepatitis, and less fibrosis
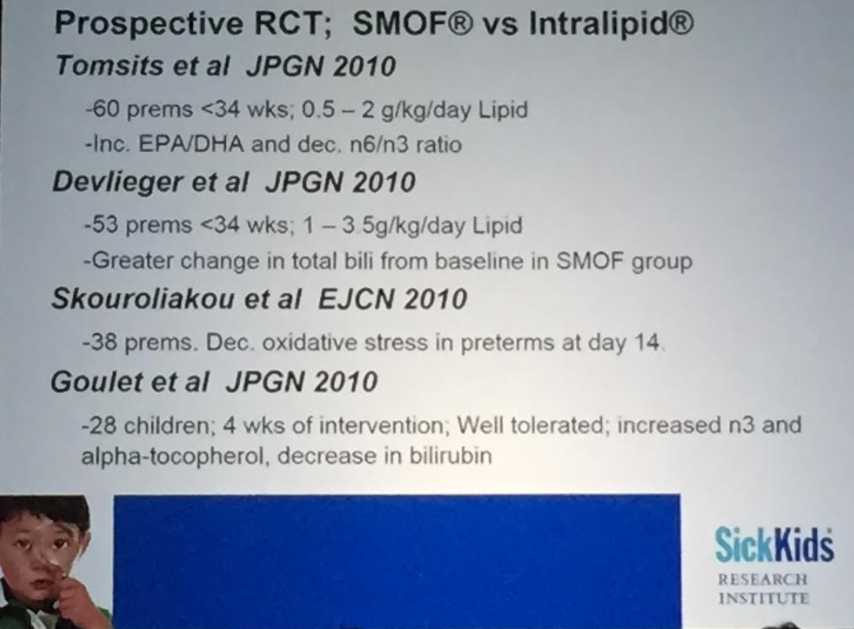
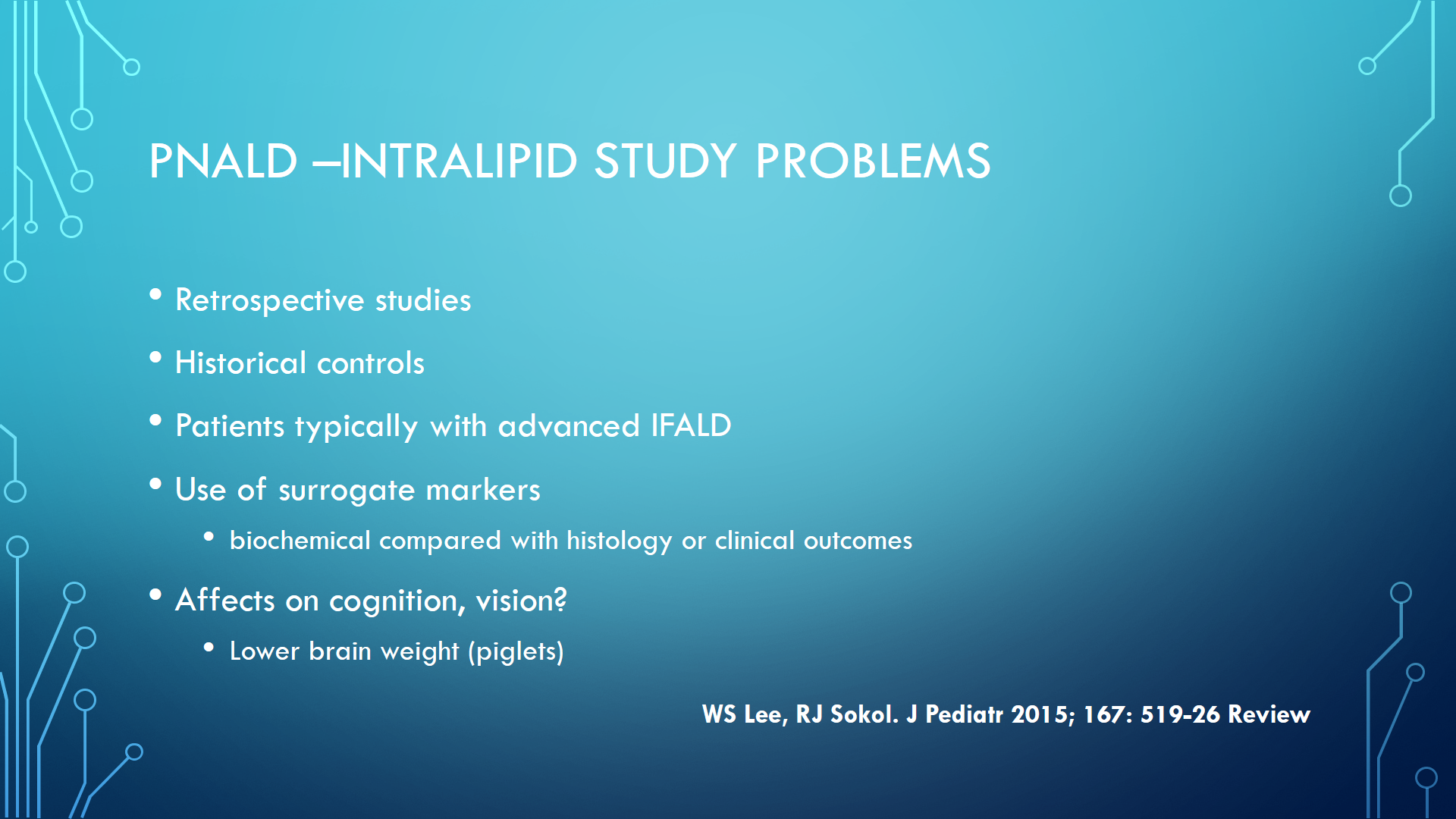
- Compared improvements with lipid minimization (1 g/kg/day) compared to newer agents: omegaven and SMOFlipid. Additional studies are needed due to limitations of previous studies
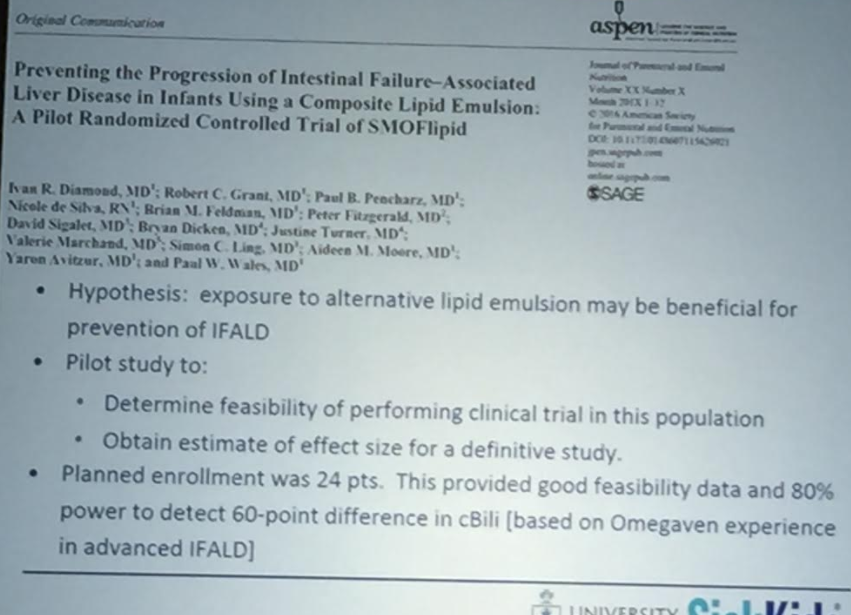
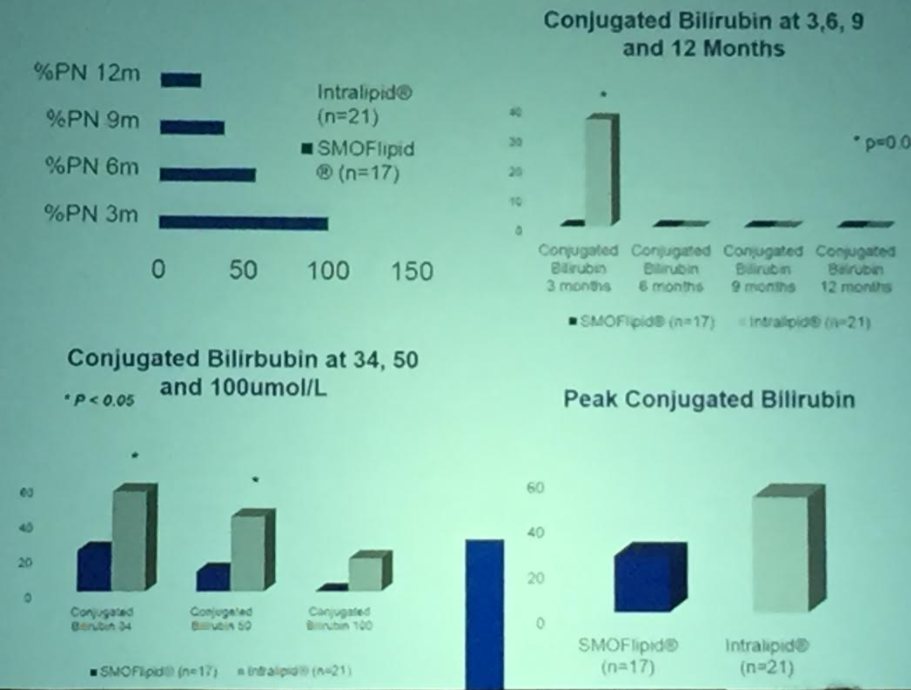
- Discussed SMOFlipid vs. Intralipid trial at 5 centers in Canada. N=24.
- At SickKids: SMOFlipid for all preterms at admission & for term infants after 2 weeks of PN. Dosing 2-2.5 g/kg & now accounts for 85% of lipid usage at institution
- None of the lipid products were designed for preterm infants. Intralipid has a pediatric indication and other products are used off label
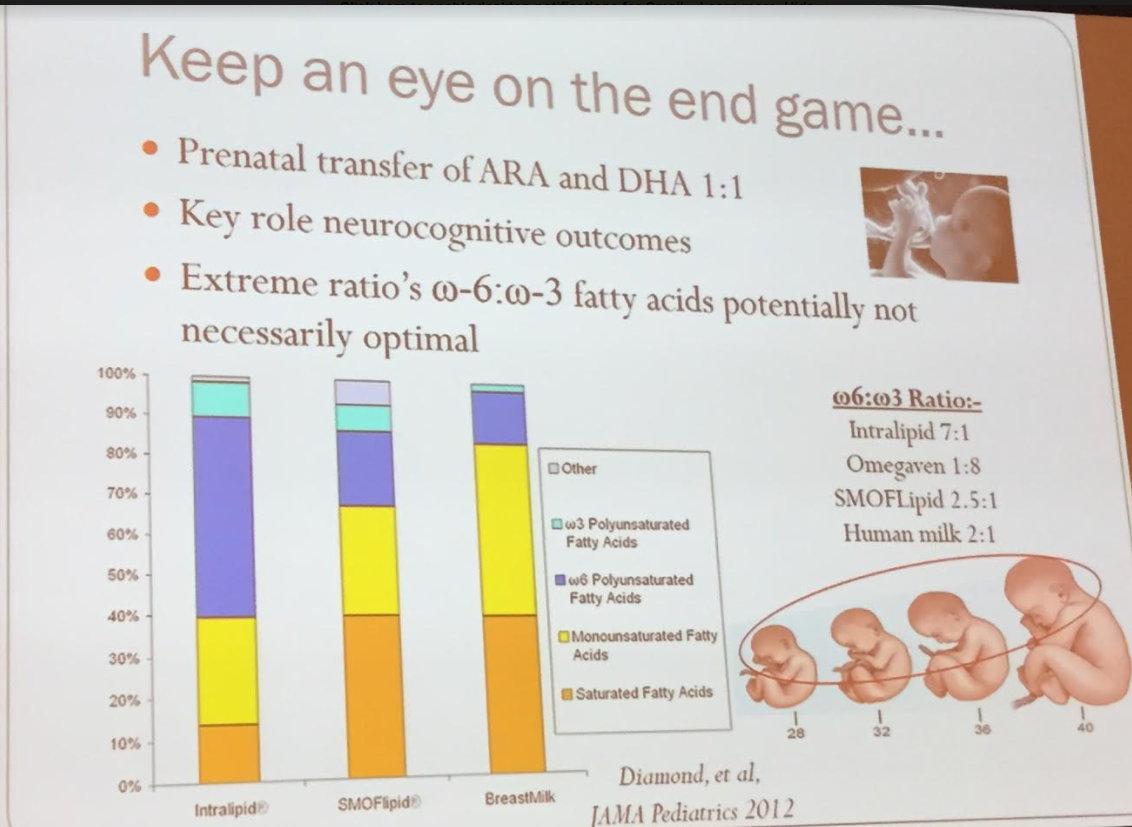
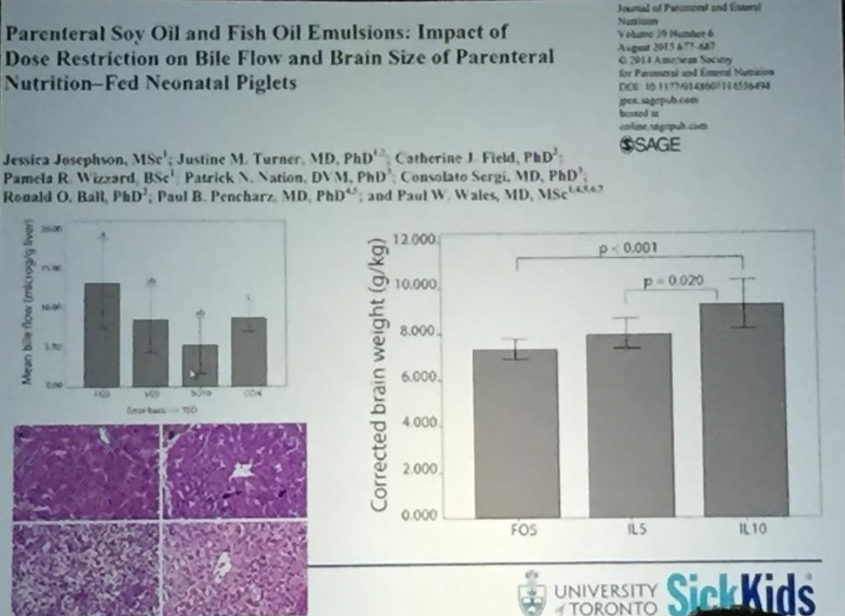
- Lipid restriction probably affects brain size/development; thus, a lipid agent that allows for higher doses likely will be beneficial for developmental outcomes. The retina can be used as a biomarker of the brain affects of lipids.










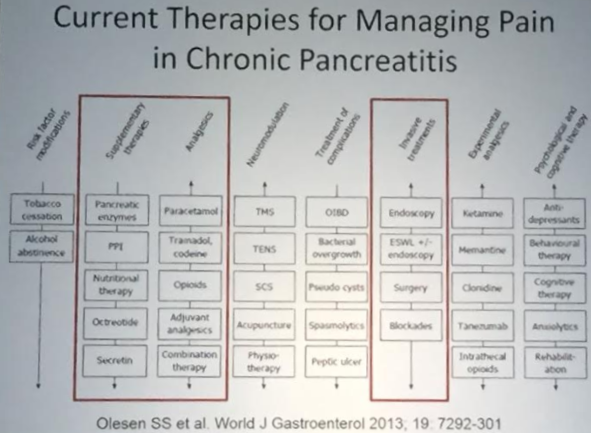
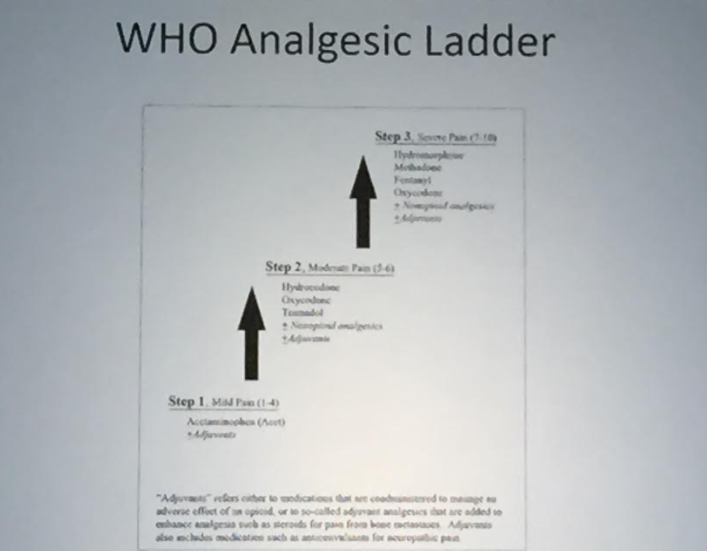
Painful Chronic Pancreatitis: Management/therapeutic interventions
Vikesh Singh Johns Hopkins University School of Medicine
Slides are not available in syllabus