A Almallouhi et al. J Pediatr Gastroenterol Nutr. 2025 DOI: 10.1002/jpn3.70316. Clinical outcome of constipation as the presenting symptom in children with celiac disease
Background: “It is not clear if CeD prevalence is higher in children with refractory and chronic constipation or not.11–15 The current guidelines from the American Gastroenterological Association (AGA) and the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) do not consider constipation an indication for CeD testing in the absence of suggestive family history, growth, or developmental delay.”
Methods: This was a retrospective study (1994-2024) of children (<18 years) who presented with constipation and then diagnosed with celiac disease (CeD). There were 248 children with CeD, 177 (71%) had biopsy-confirmed CeD, and 56 (23%) were diagnosed with serology-only criteria
Key findings:
My take:
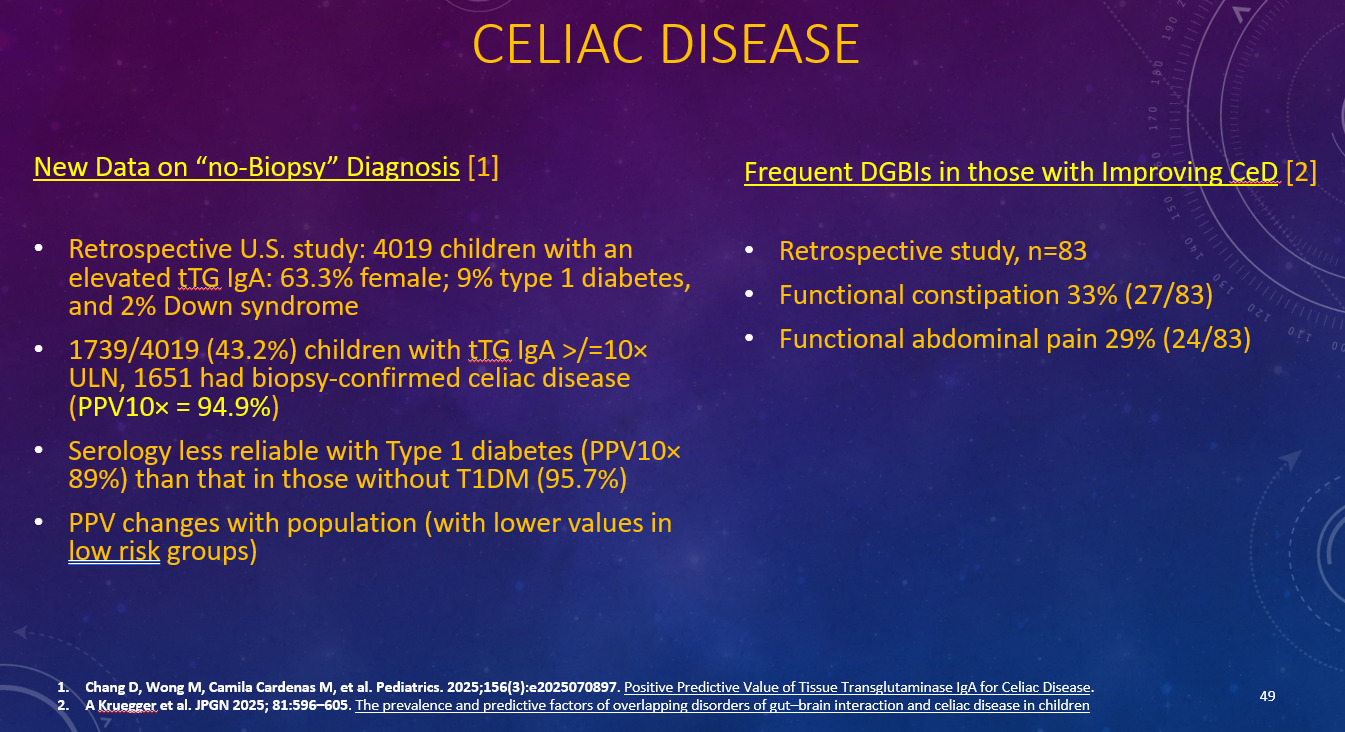
It is unclear if having constipation increases the risk of celiac disease
Many children with celiac disease also have functional disorders like irritable bowel and constipation that often continue despite a gluten-free diet
RM Califf et al. N Engl J Med 2026;394:4-6. A Threat to Evidence-Based Vaccine Policy and Public Health Security at the FDA
This editorial by 12 former FDA commissioners of both Democratic and Republican administrations is sharply critical of recent policy changes at the FDA which threaten the supply of life-saving vaccines.
Here is an excerpt:
“The existing regulatory model builds public trust by encouraging open information exchange and rigorous, transparent scientific debate. Yet a memo sent last week to FDA staff will upend core policies governing vaccine development and updates…
The memo (available at https://www.biocentury.com/article/657740) was written by Vinay Prasad, director of the FDA’s Center for Biologics Evaluation and Research (CBER), who also serves as the agency’s chief scientific officer, chief medical officer, and acting head of CBER’s office of biostatistics, as well as overseeing the division responsible for vaccine review and approval. His memo characterizes the actions of FDA scientists who express concerns about agency processes or decisions to outside parties as “unethical” and “illegal.” It calls for scientific debates to be kept within the agency “until they are ready to be made public,” and instructs staff members who disagree with the new framework to “submit your resignation letters.”..
If enacted, the framework would impede the ability to update vaccines to keep up with the natural evolution of respiratory viruses or changes in the prevalence of bacterial serotypes…
The new framework rejects the agency’s long-standing reliance on “immunobridging” studies for well-understood vaccines with extensive safety data. Using this approach, once a reliable correlation with effectiveness has been established, a vaccine’s ability to stimulate the immune system to produce protective antibodies can serve as a surrogate for its efficacy in helping patients avoid infections and complications from rapidly evolving viruses such as SARS-CoV-2 and influenza. Because these viruses change frequently, repeating large-scale efficacy trials for every new seasonal strain is not feasible within the time needed to update the vaccines…
Abandoning the existing methods won’t “elevate vaccine science,” as the memo asserts. It will subject vaccines to a substantially higher and more subjective approval bar. The proposed measures will slow the replacement of older products with better ones and will create potentially prohibitive expenses for new market entrants…Moreover, insisting on long, expensive outcomes studies for every updated formulation would delay the arrival of better-matched vaccines when new outbreaks emerge or when additional groups of patients could benefit…
The new approach would also evade public transparency, including long-standing statutory and regulatory mechanisms that enable disagreements about benefit–risk balance, clinical trial end points, trial design, and data analysis to be aired in public…
The benefits and risks of many established vaccines are well understood, and imposing the new approval requirements without meaningful new evidence could make it impossible to keep up with evolving infectious threats.
The memo asserts, incorrectly, that “we do not have reliable data” on the benefits of Covid vaccination in children. Reasonable scientists should engage in open debate about how best to shape recommendations for children at lower risk for Covid-19, but substantial evidence shows that vaccination can reduce the risk of severe disease and hospitalization in many children and adolescents…
Americans’ safety depends on a culture in which evidence is reviewed openly and staff can surface concerns, challenge leadership, and engage with external scientists without fear of reprisal.
In a nearby neighborhood, my wife and I went walking and came across a “free art” stand which looked similar to a “free little library” stand. We picked out this small piece (about 5 inches on each side).
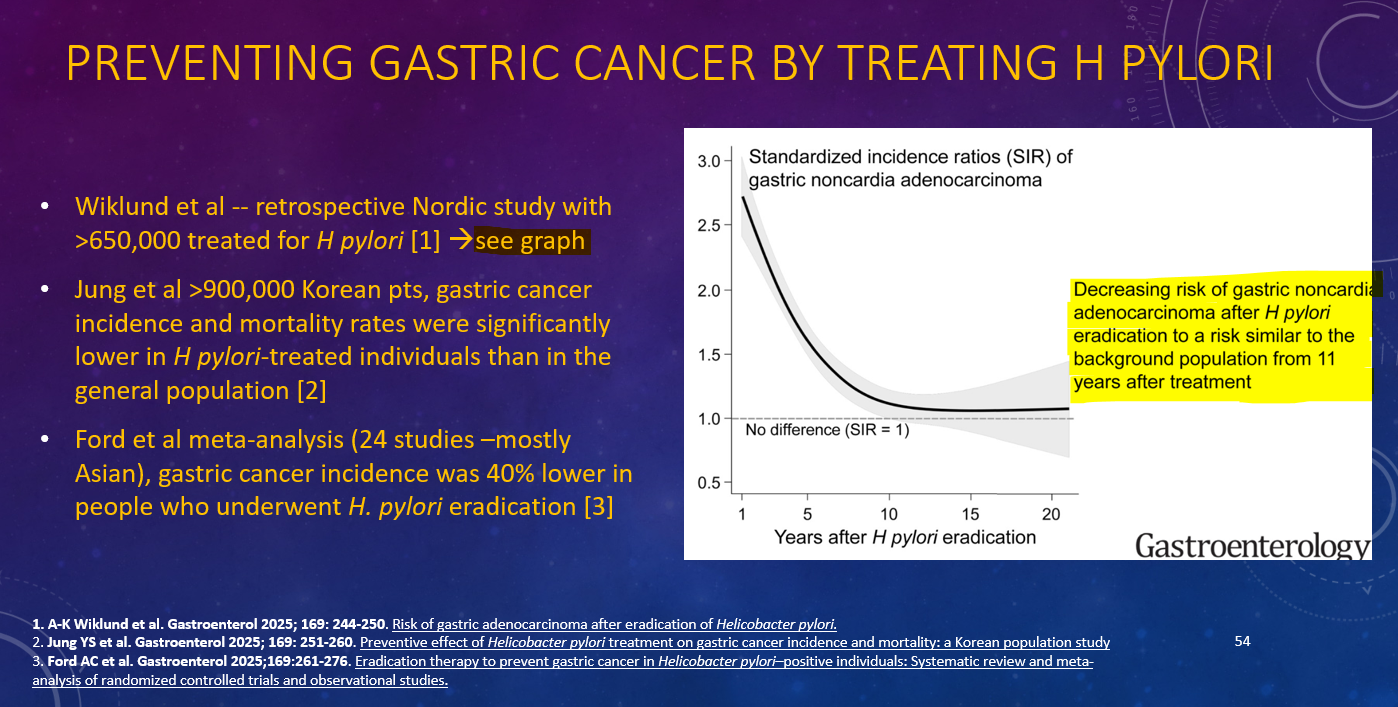
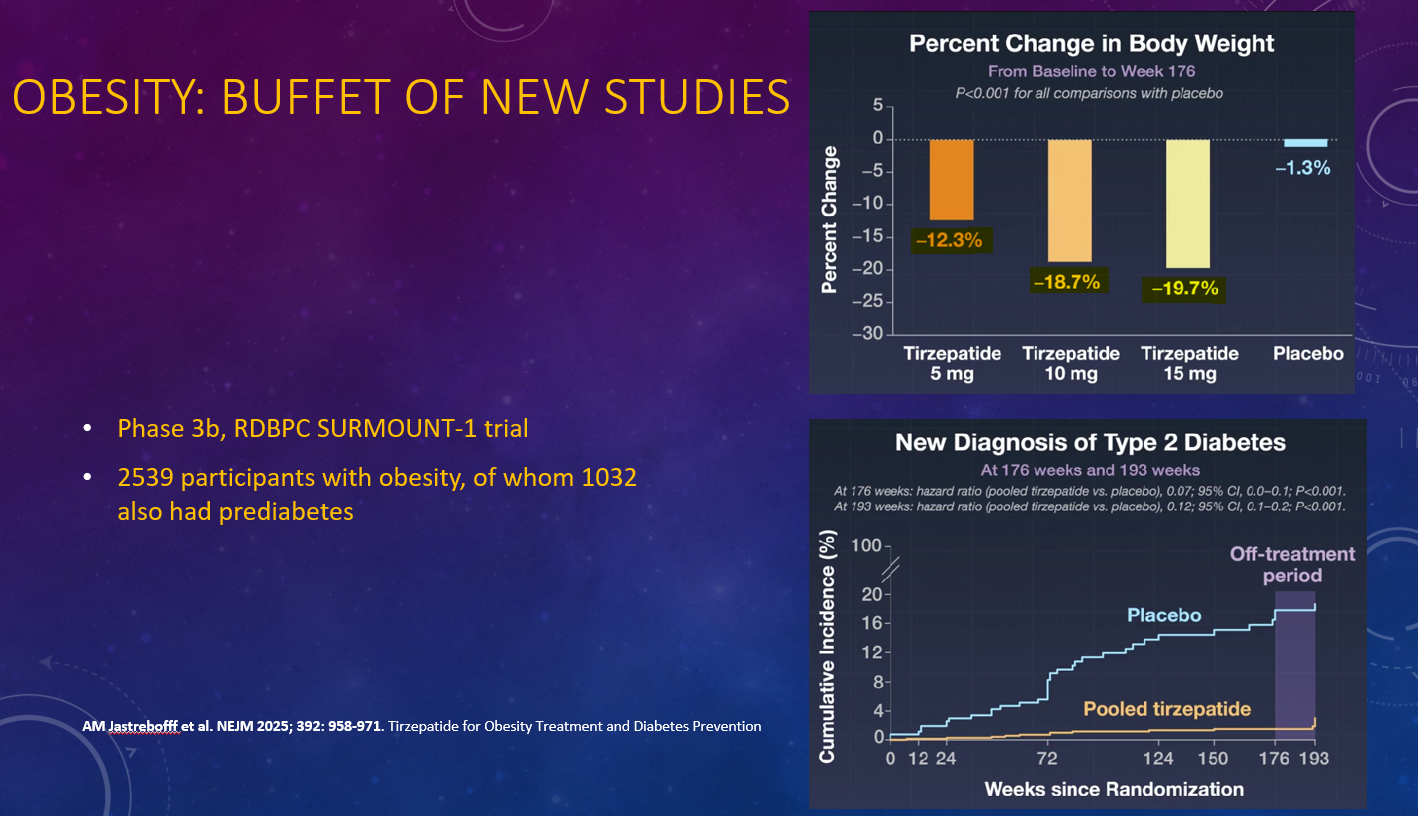
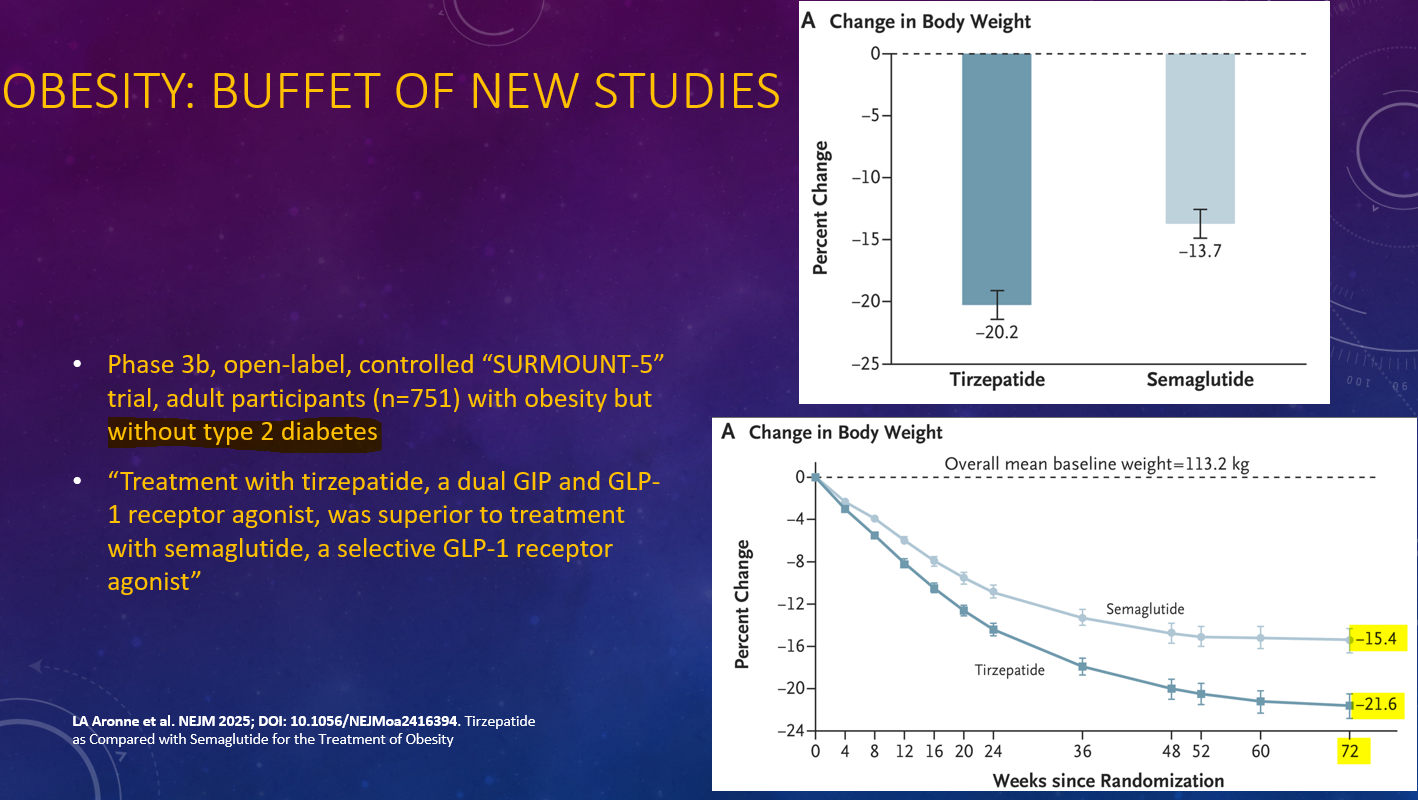
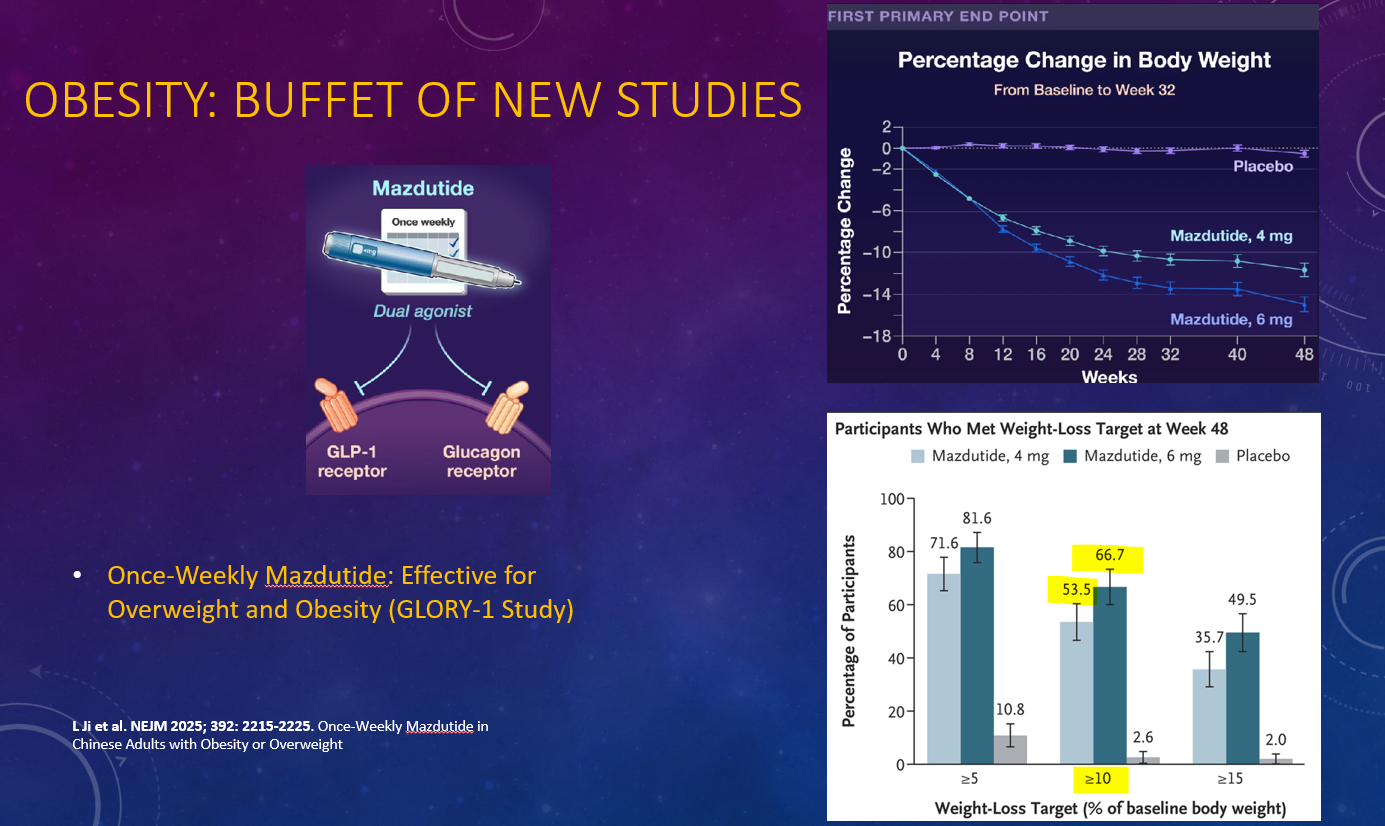
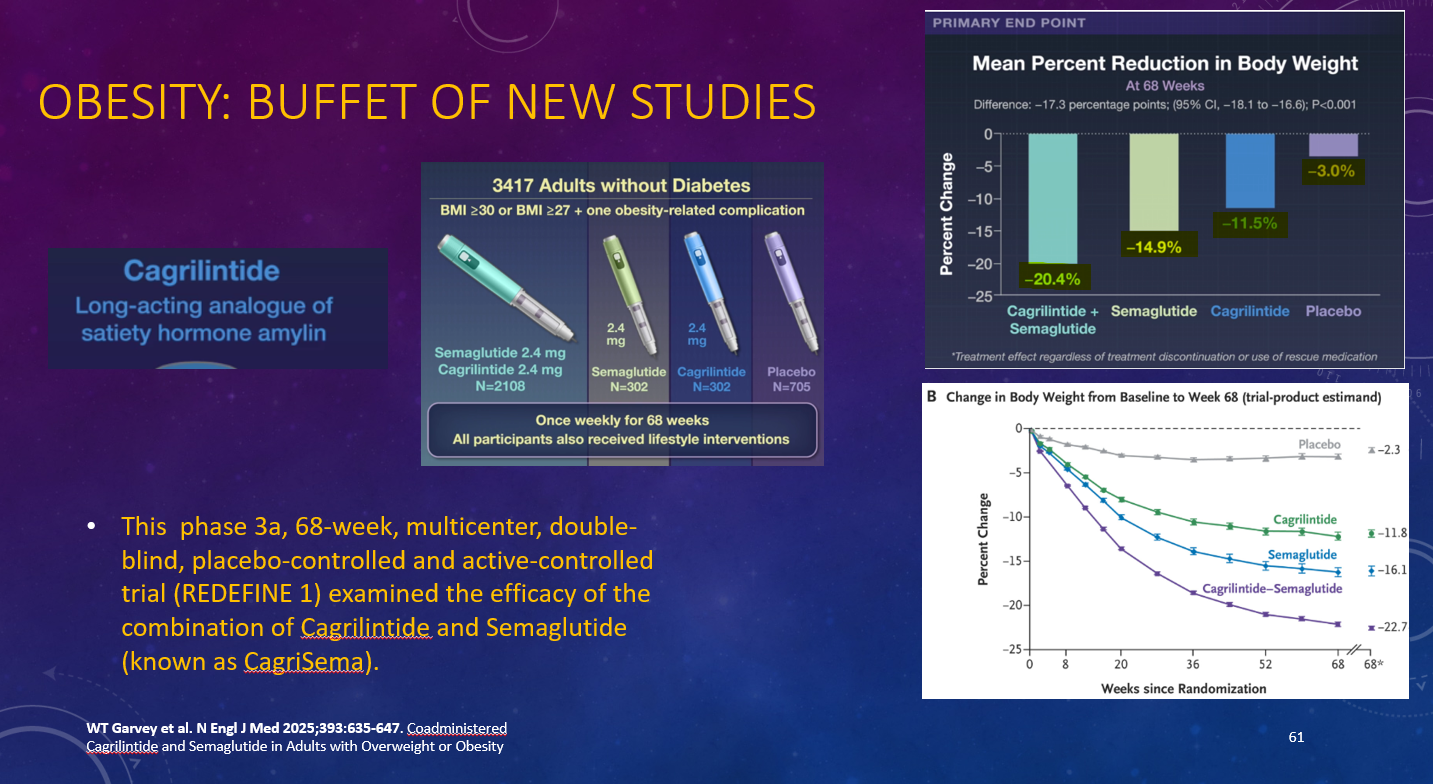
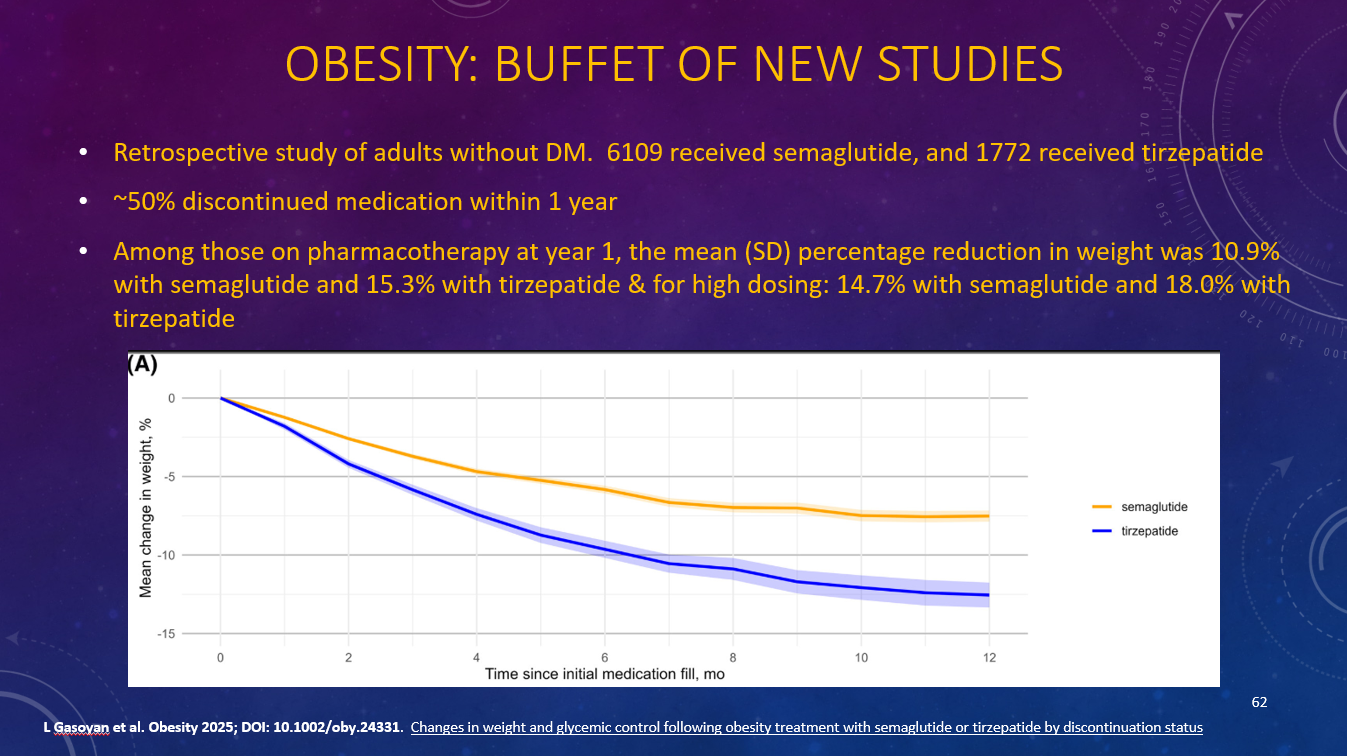
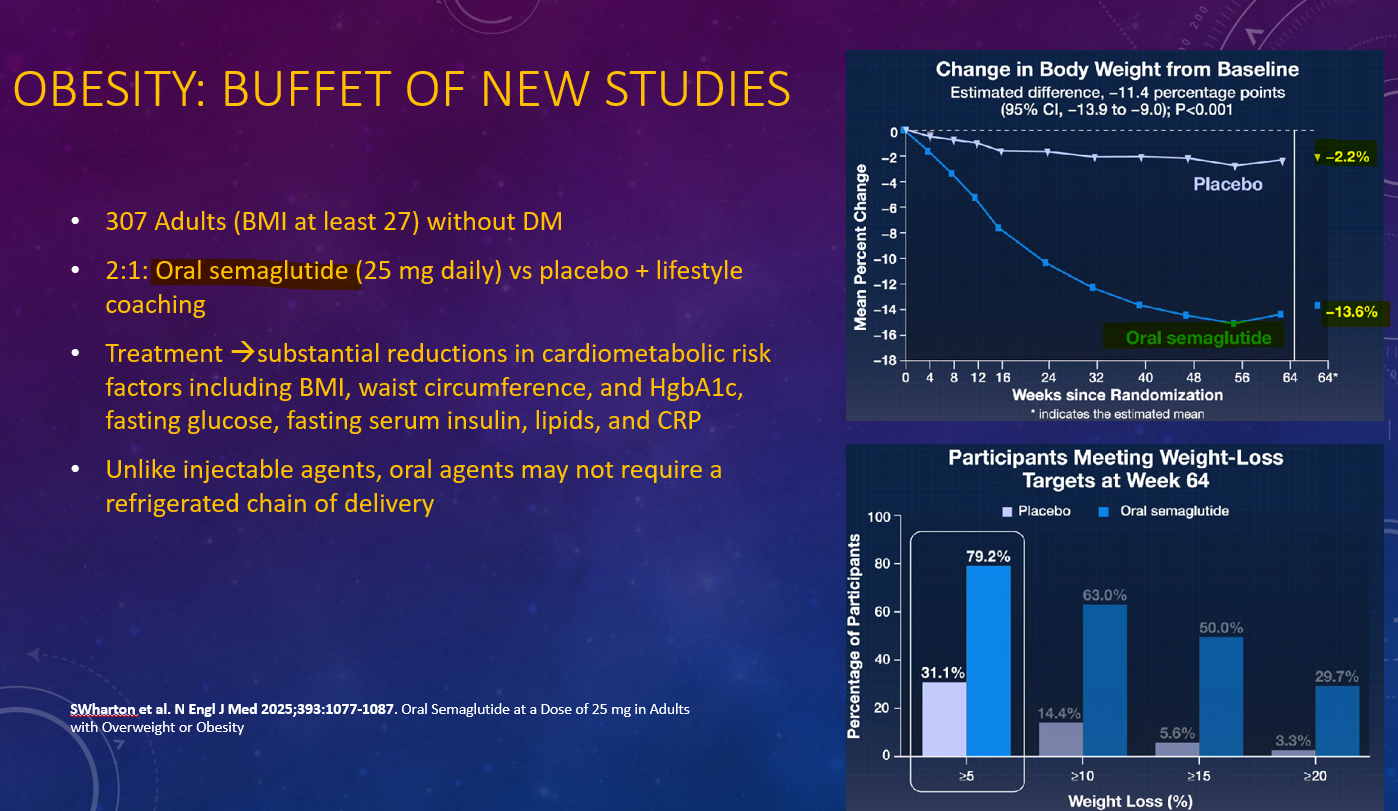
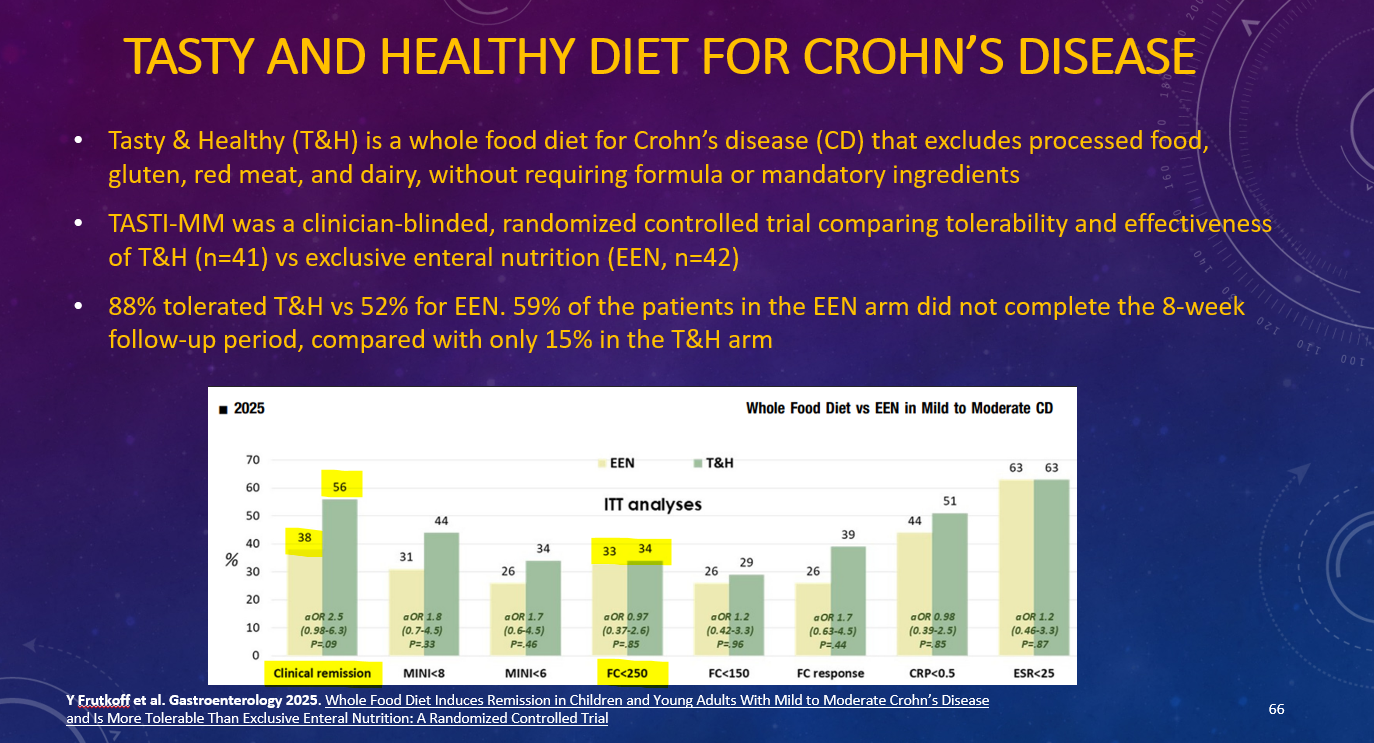
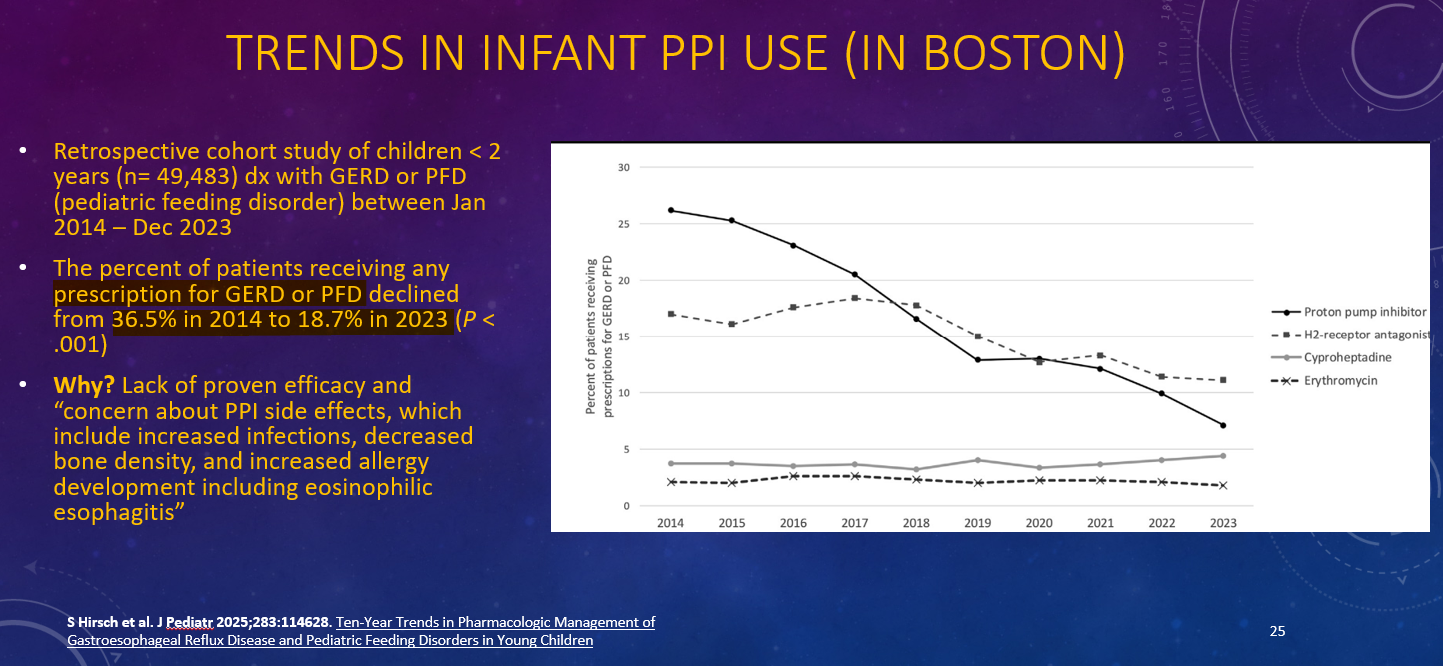
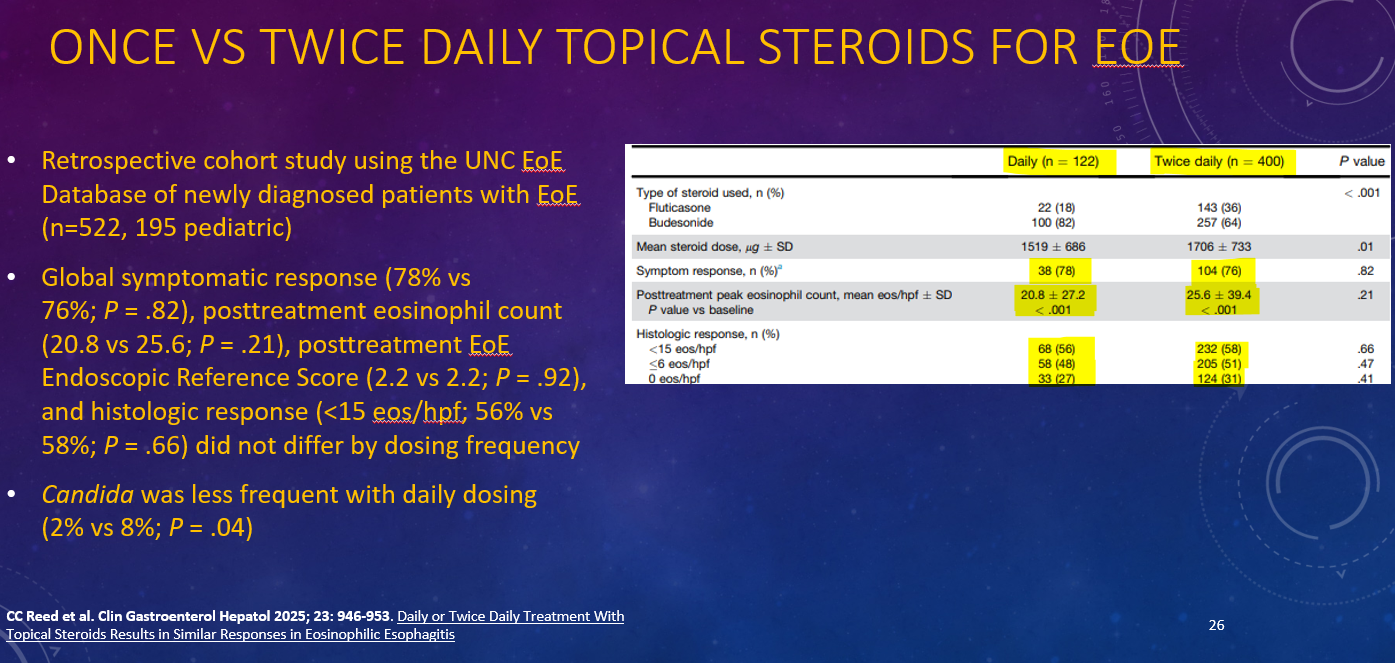
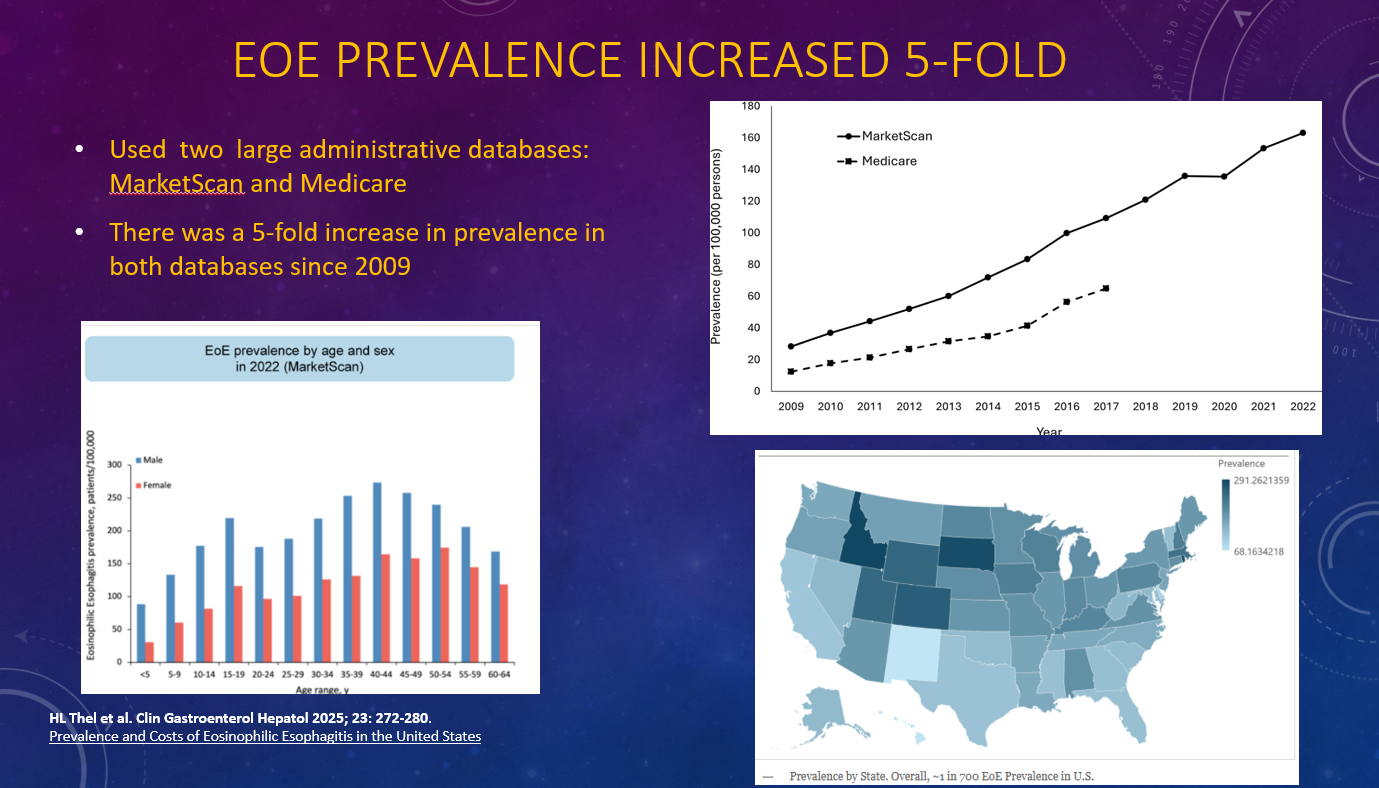
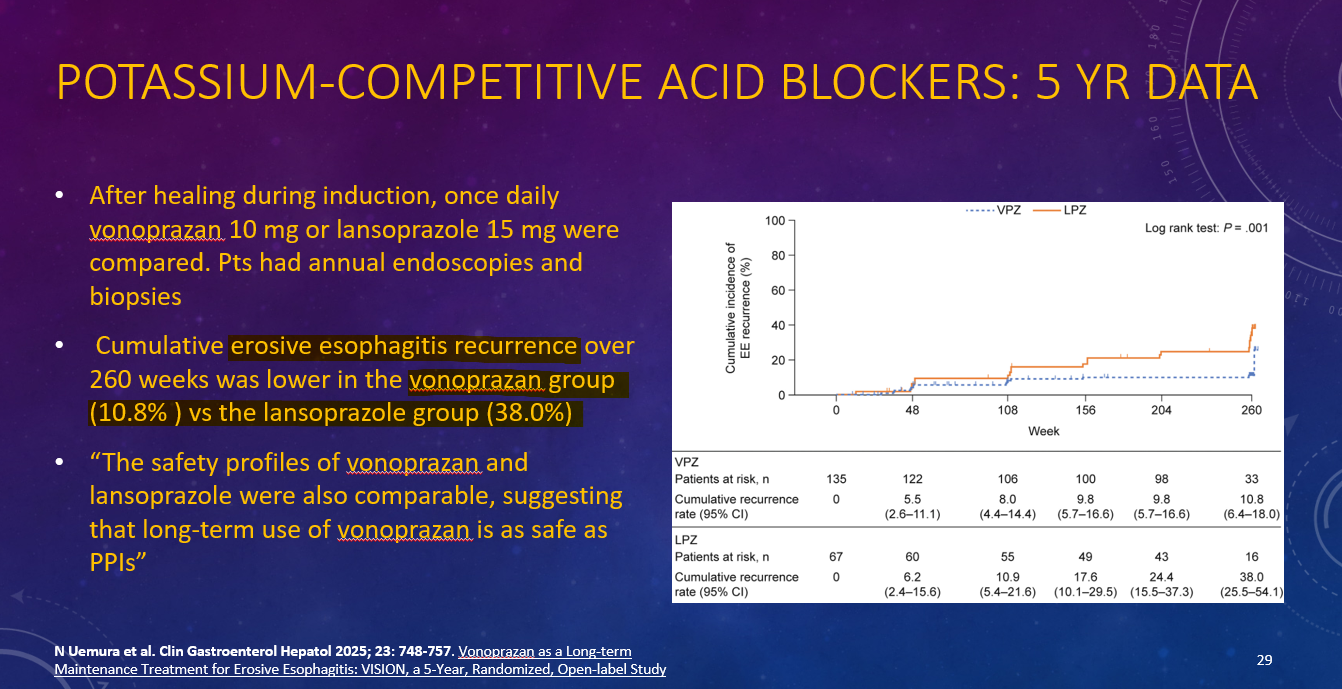
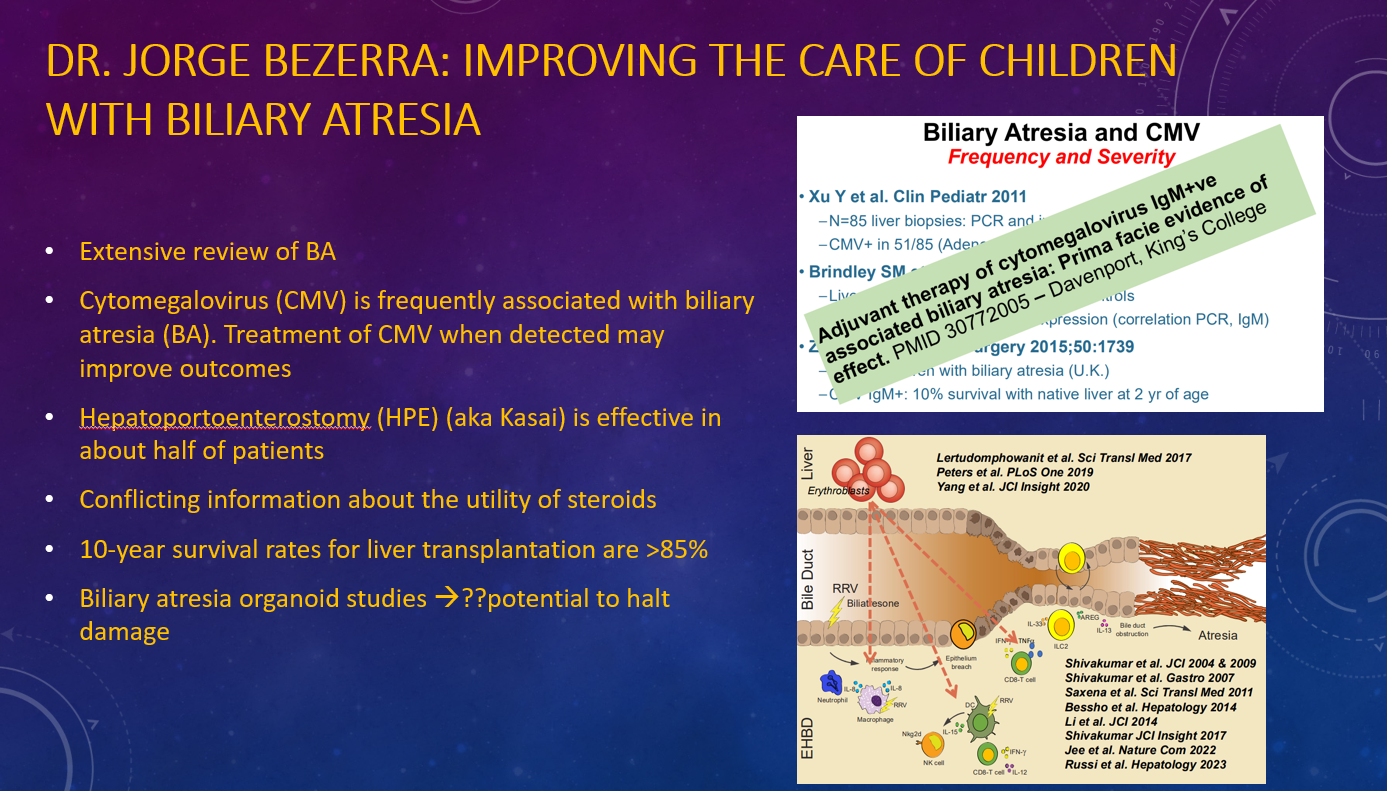
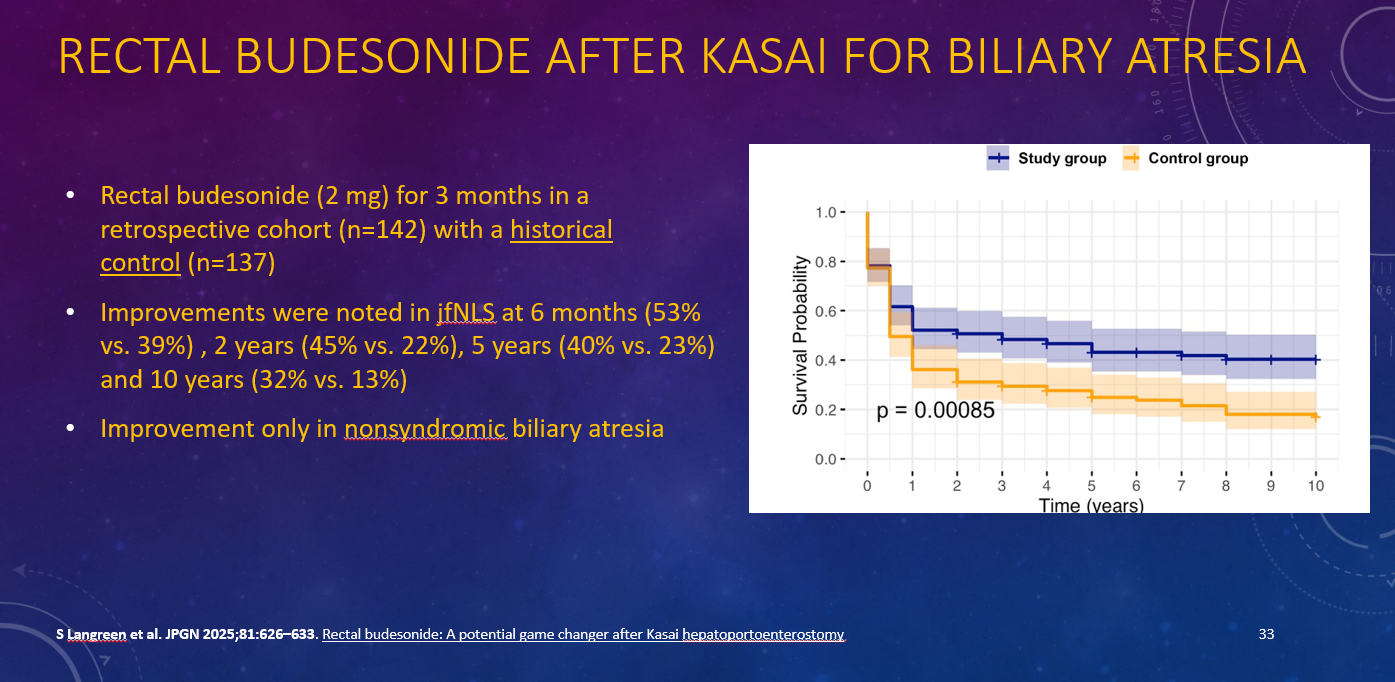
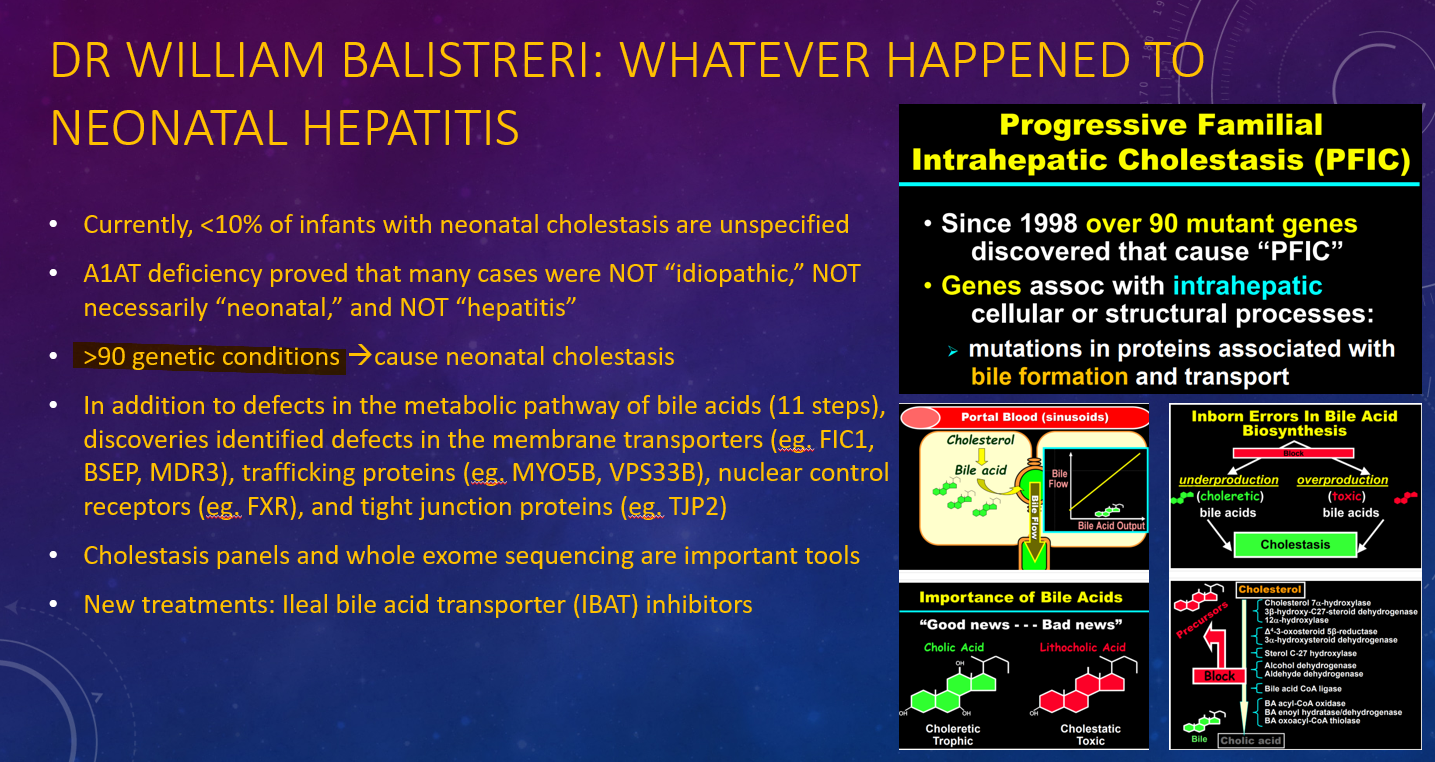
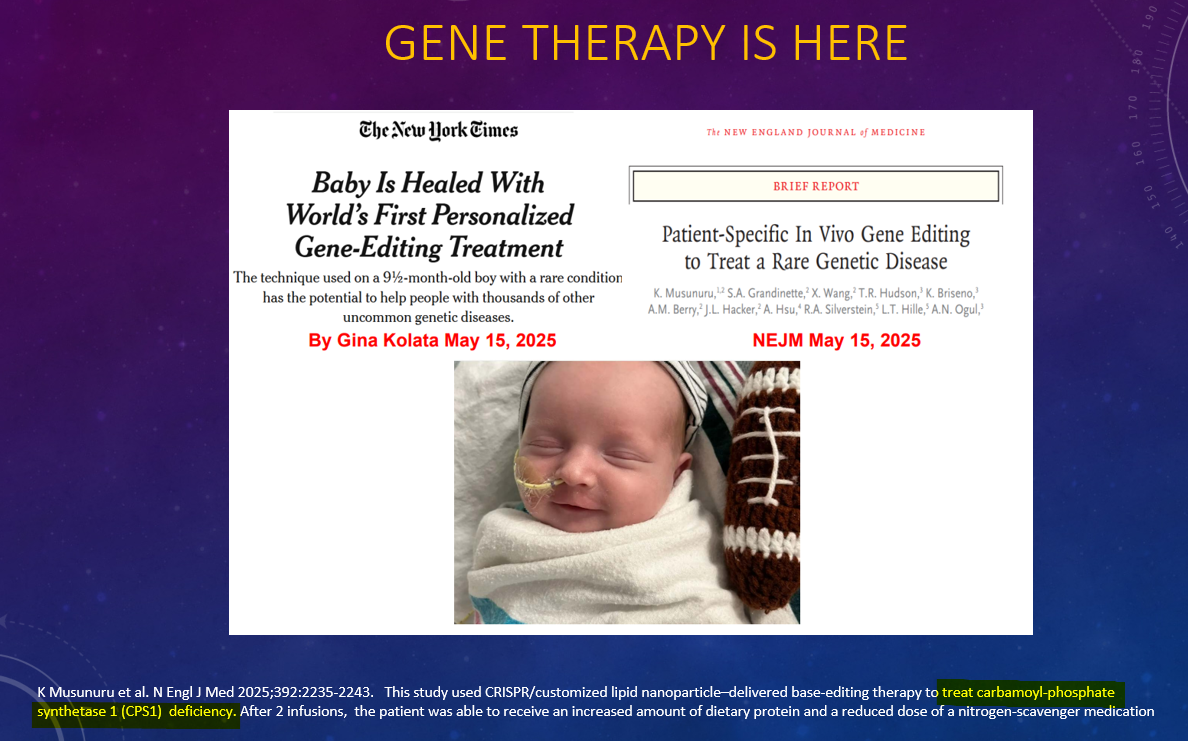
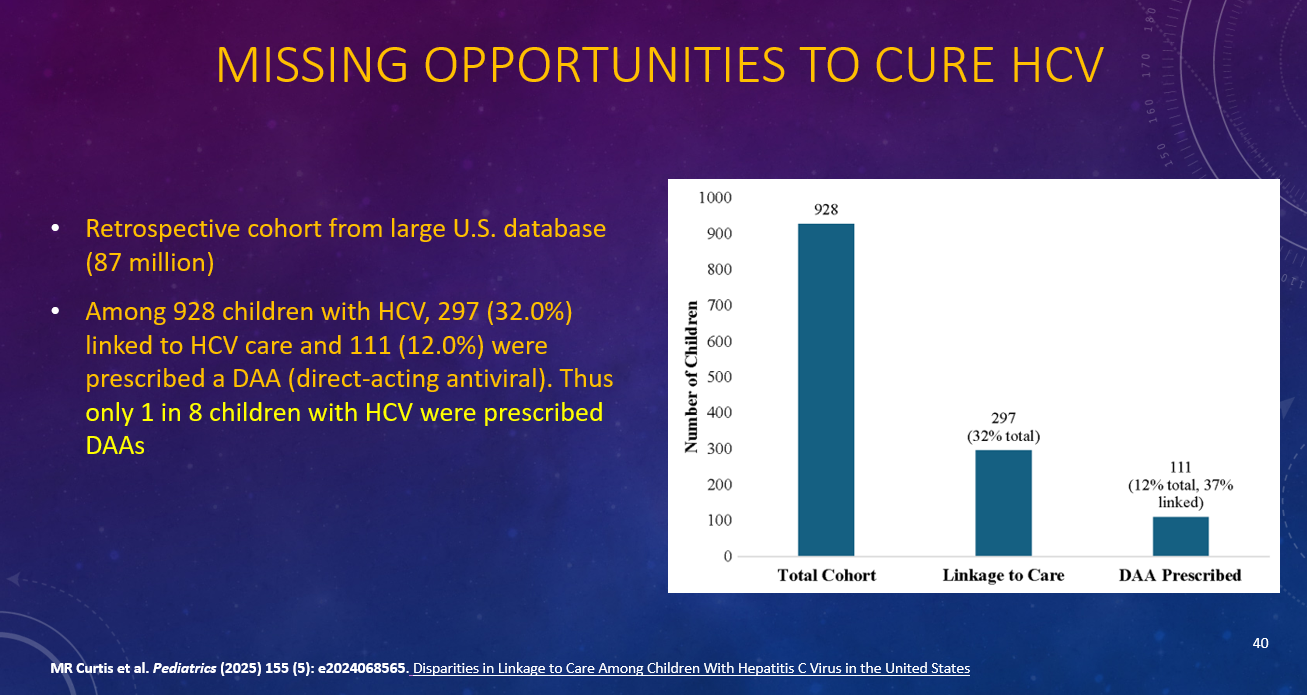
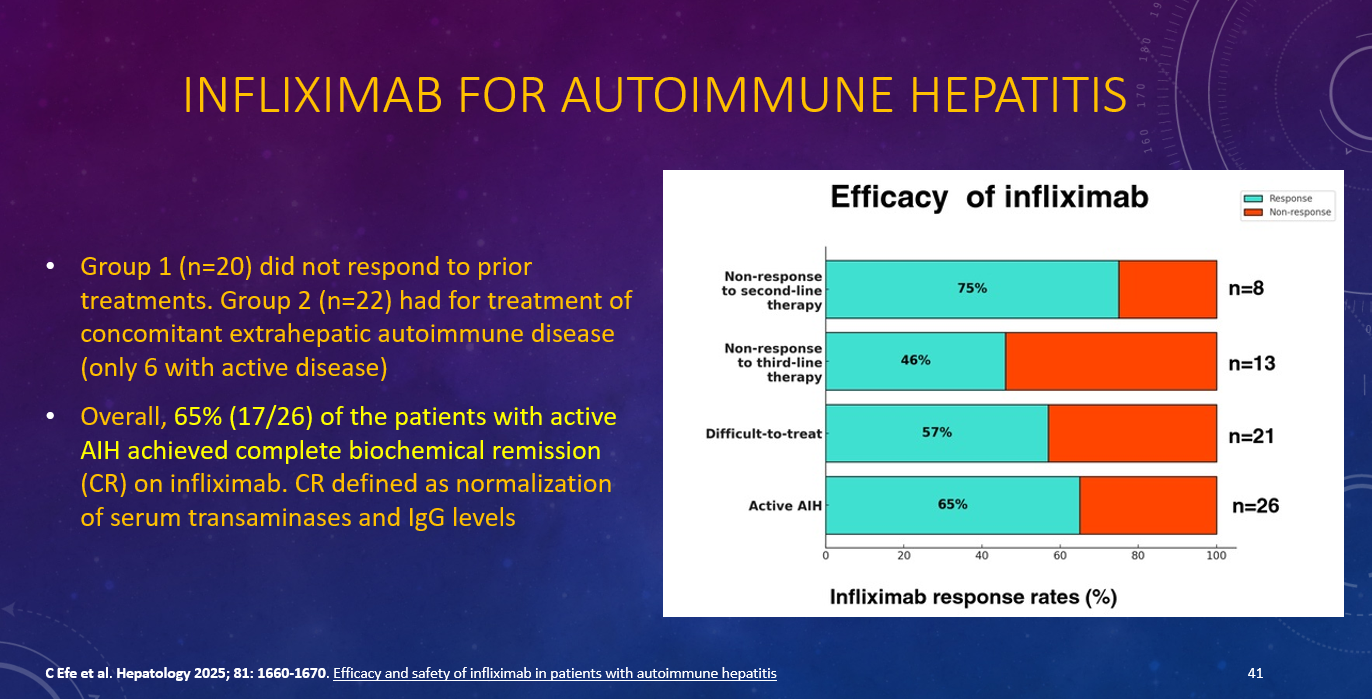
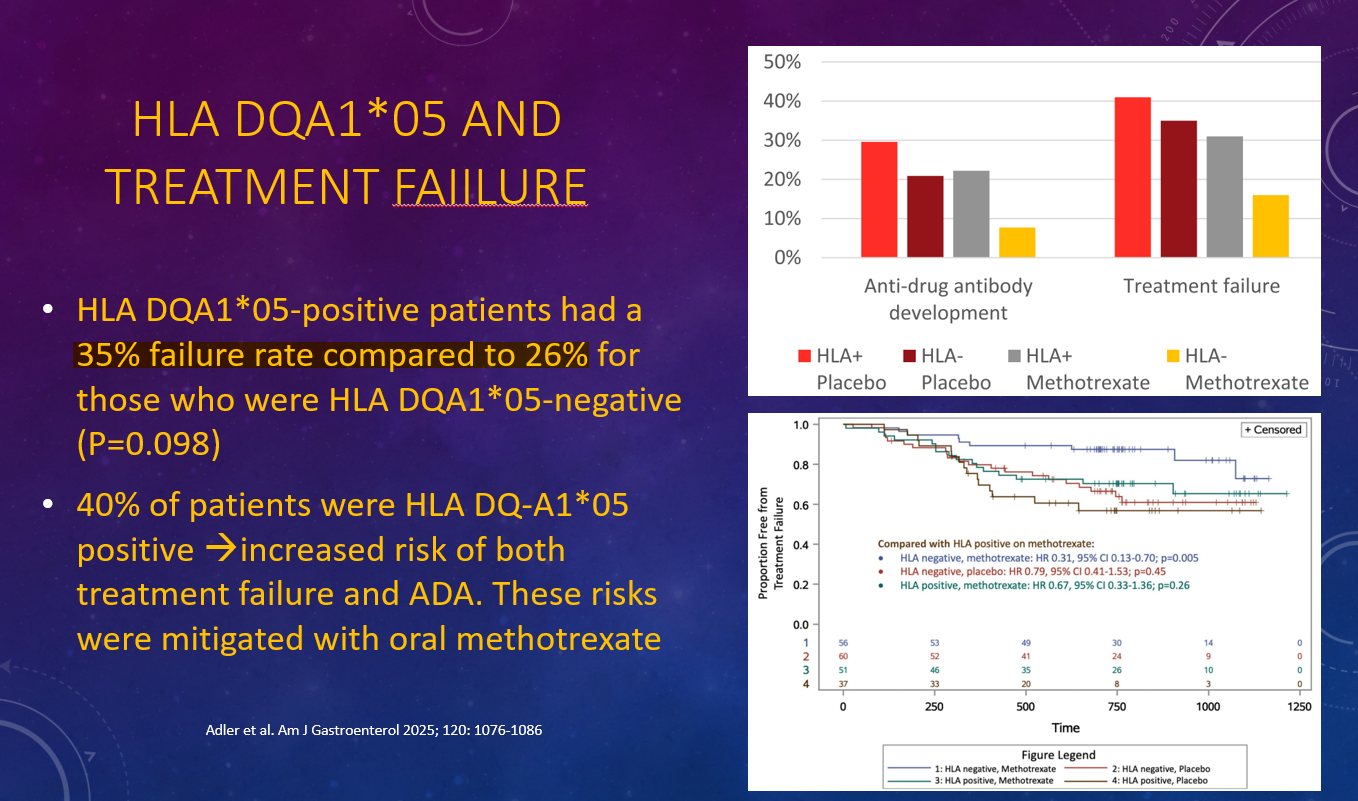
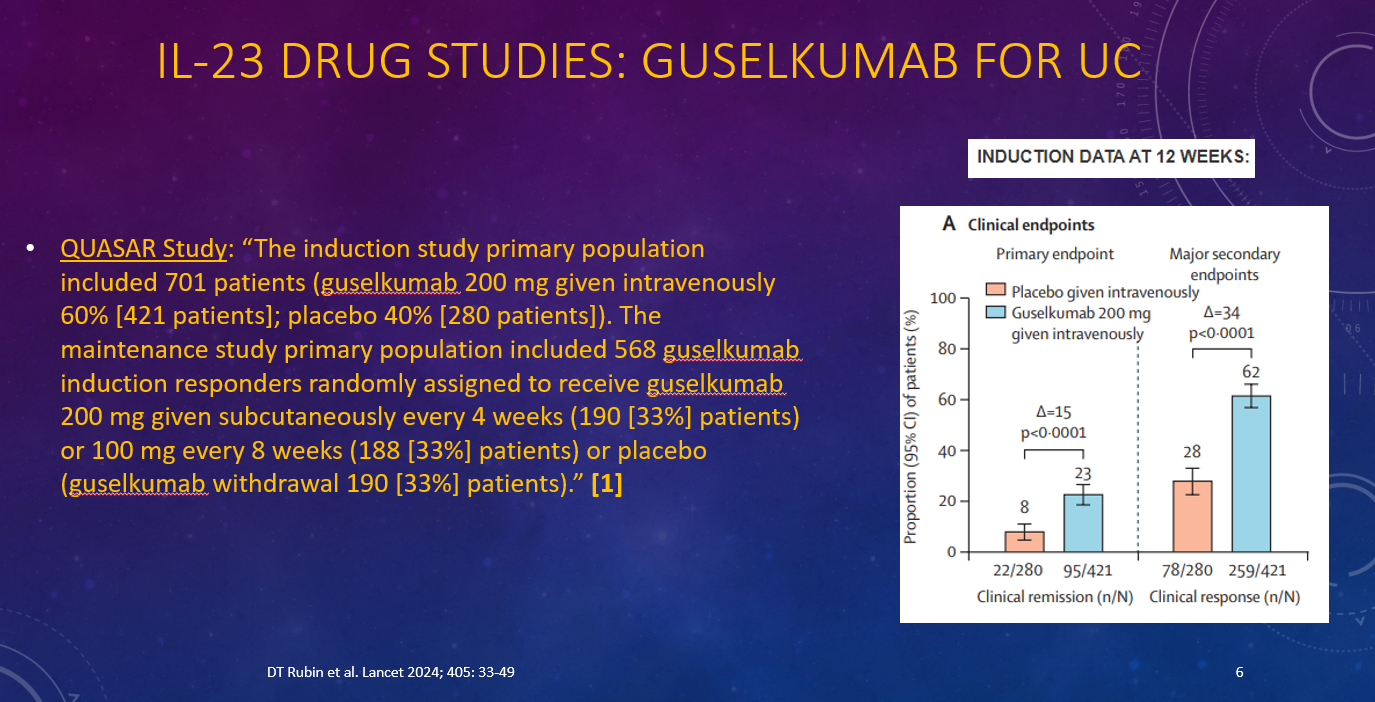
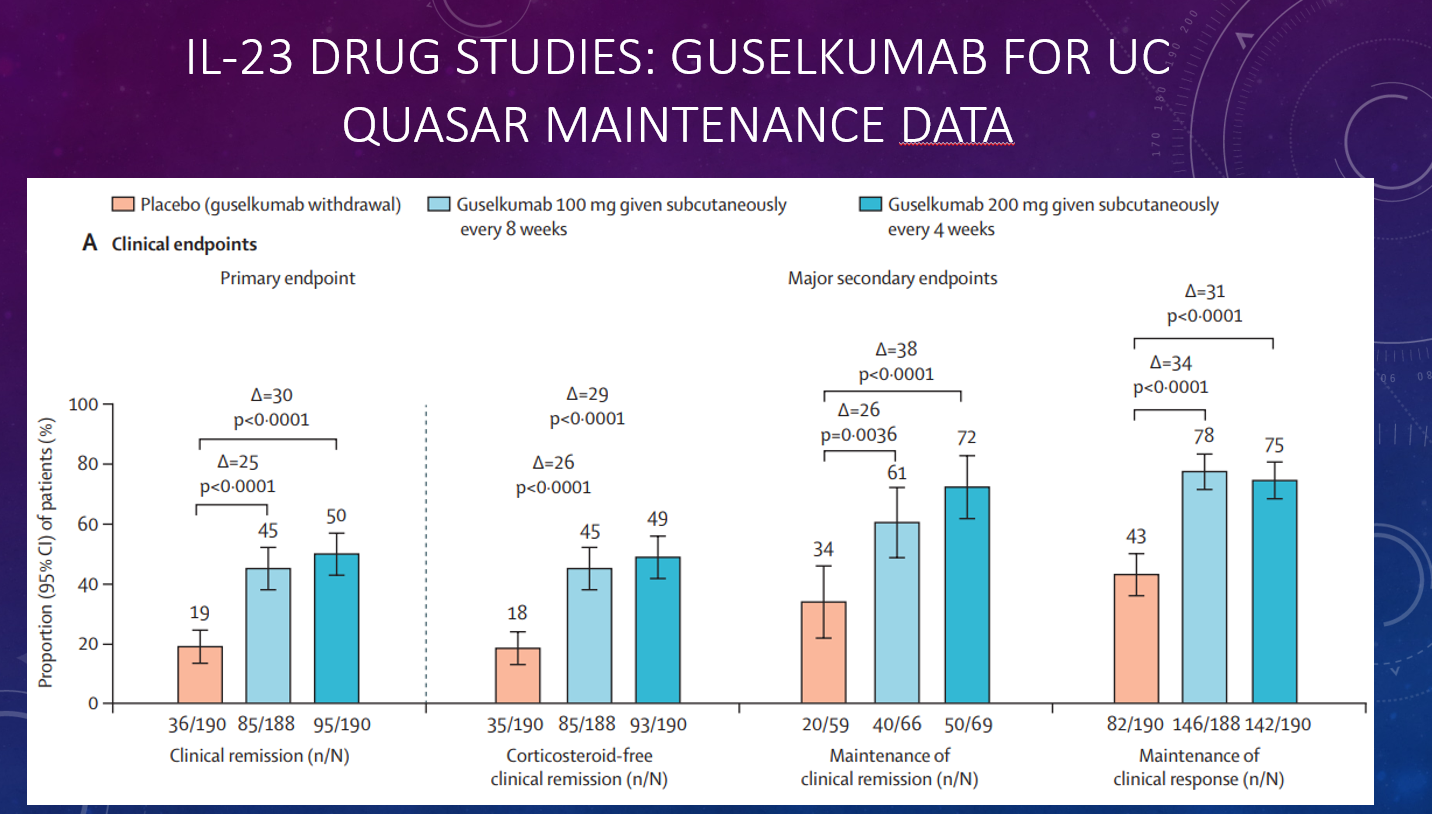
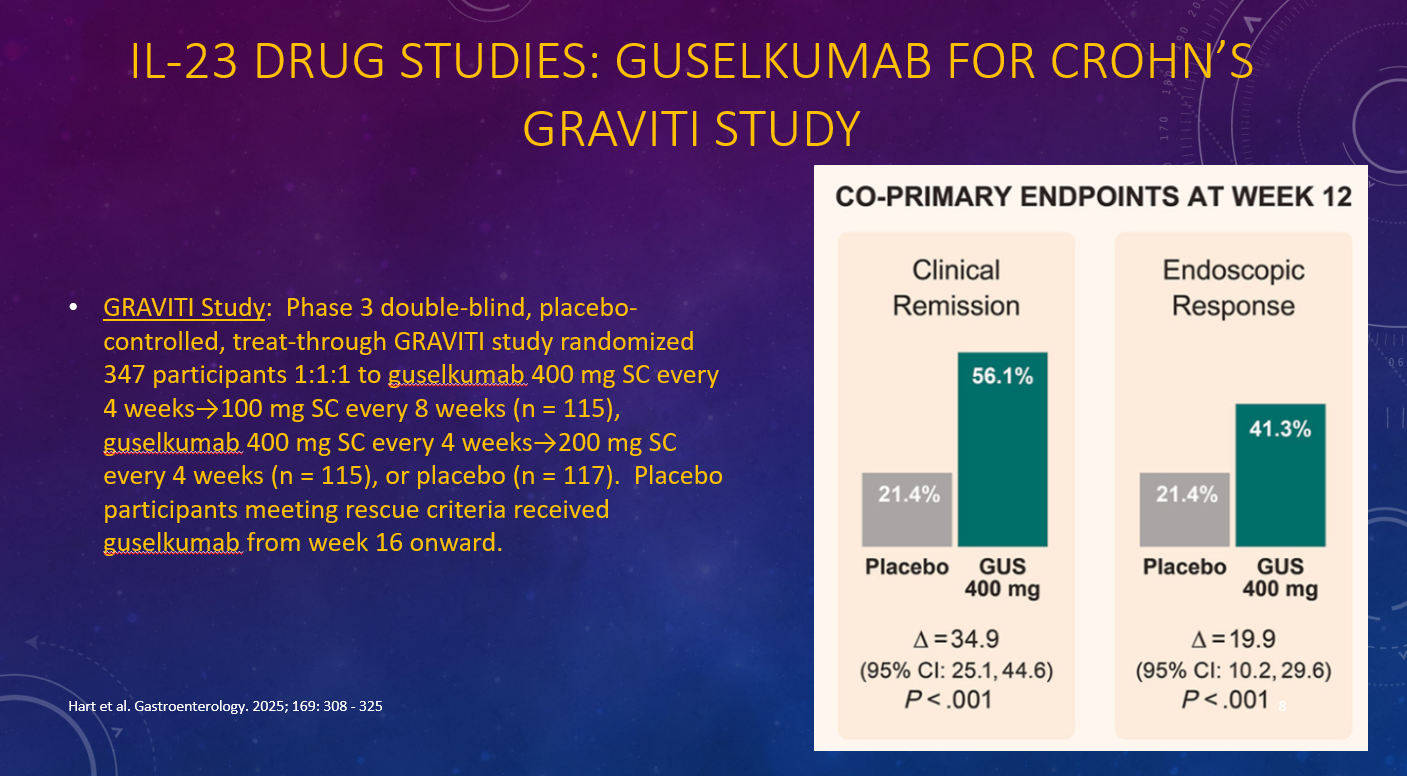
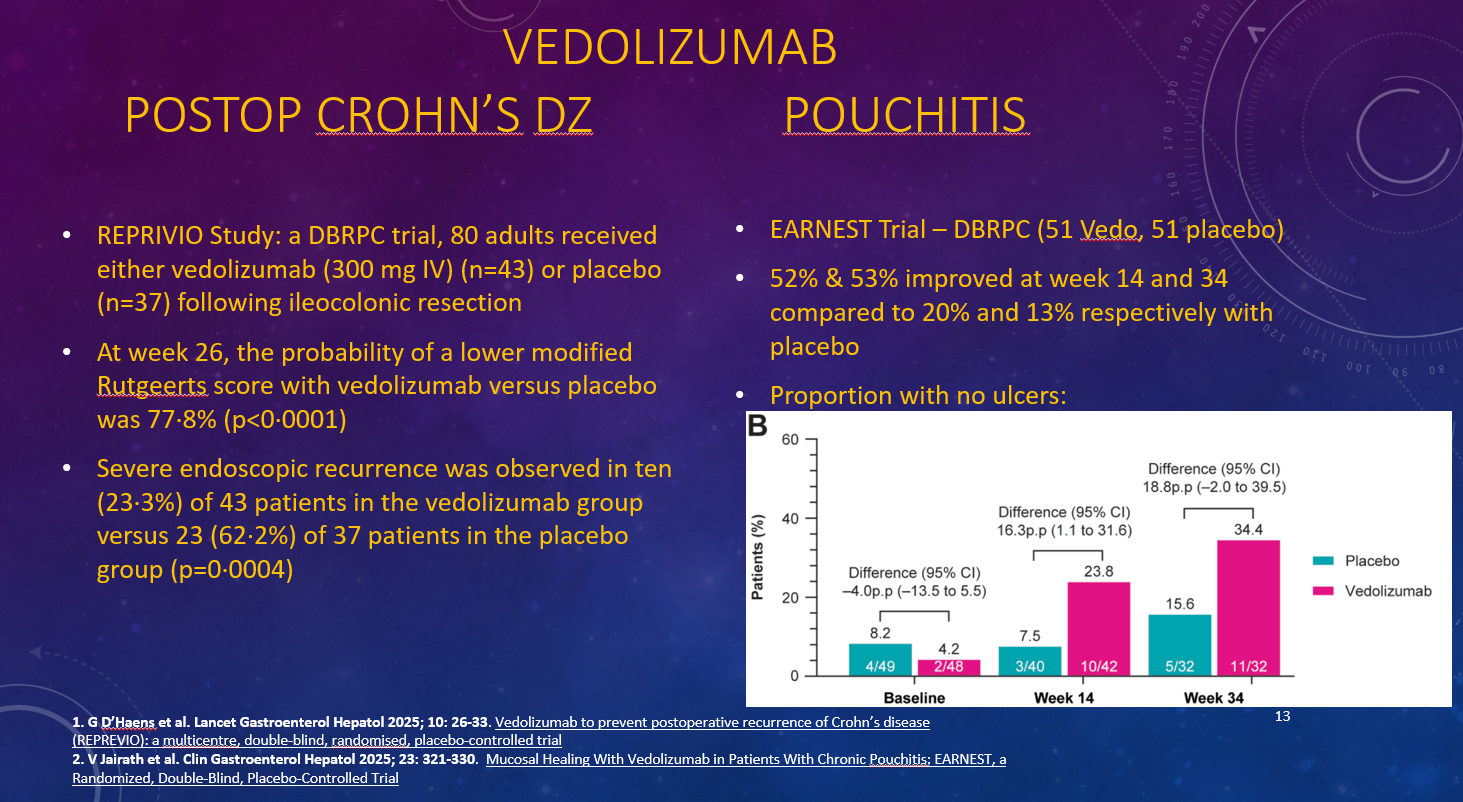
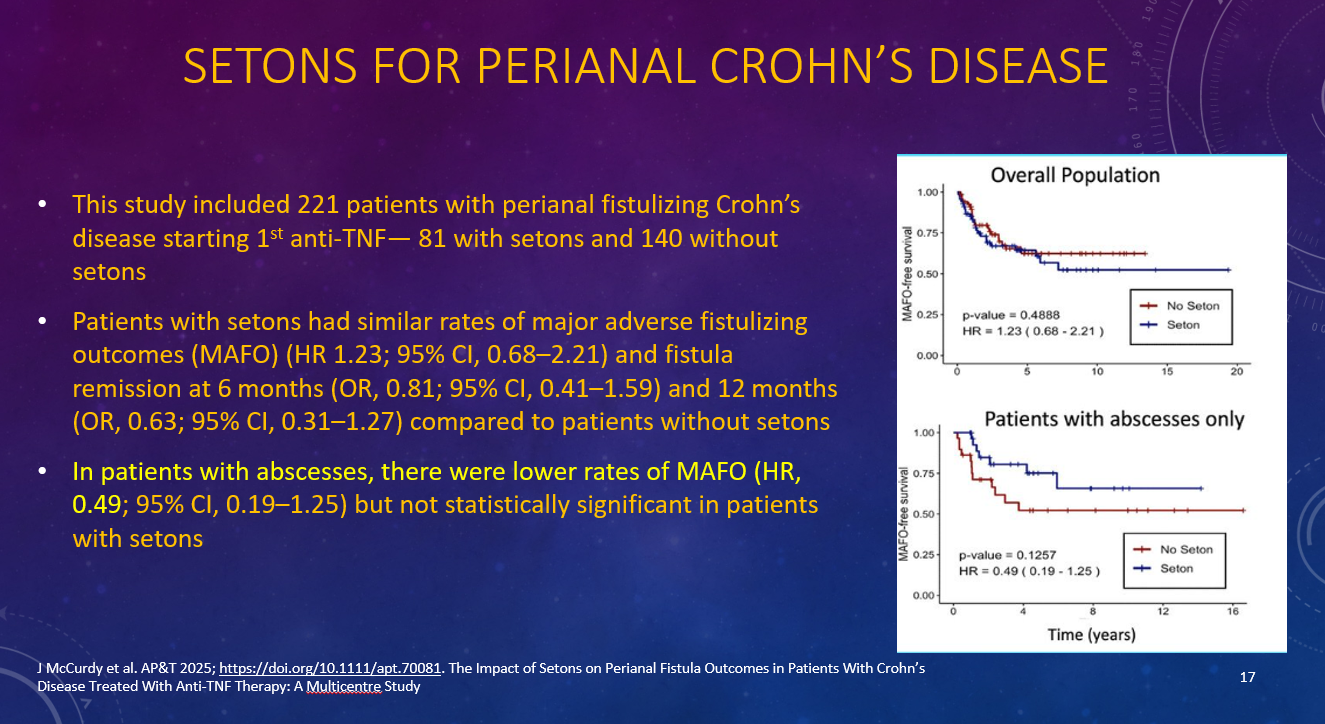
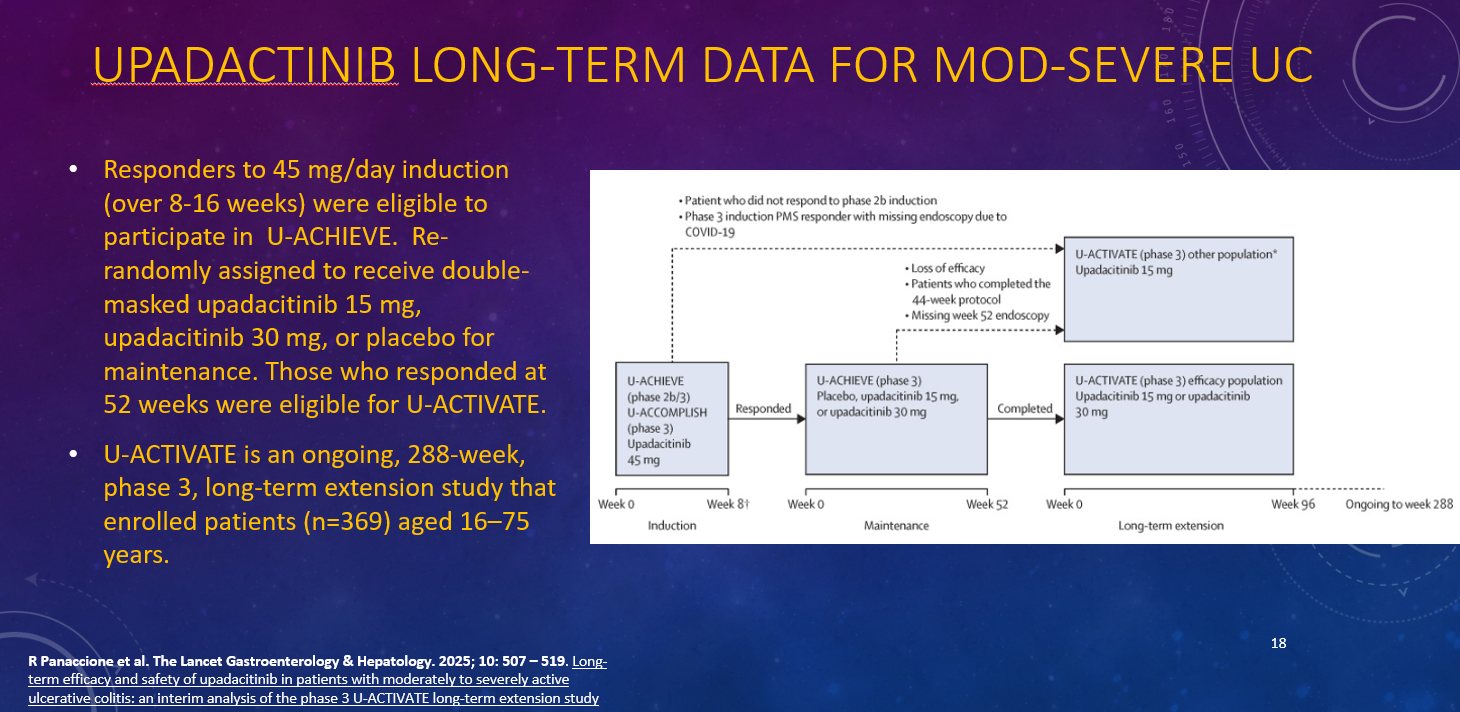
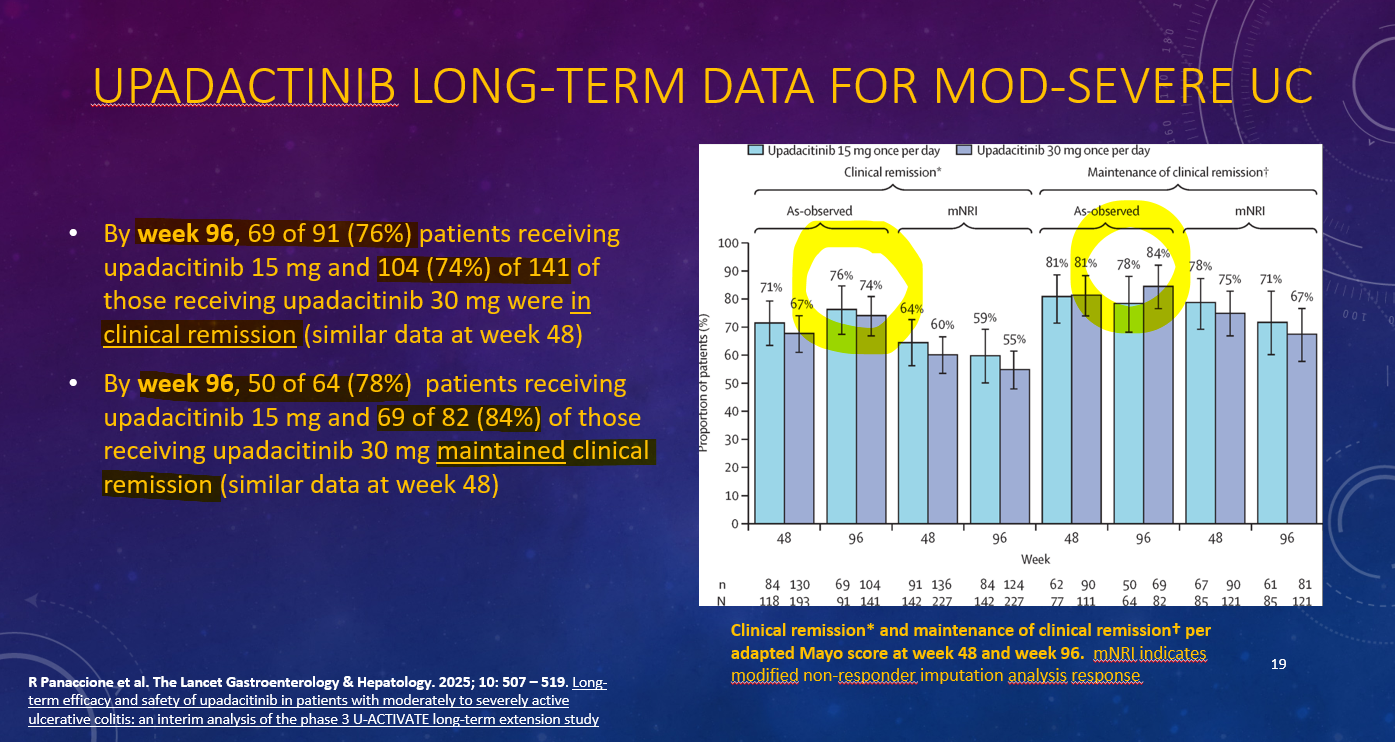
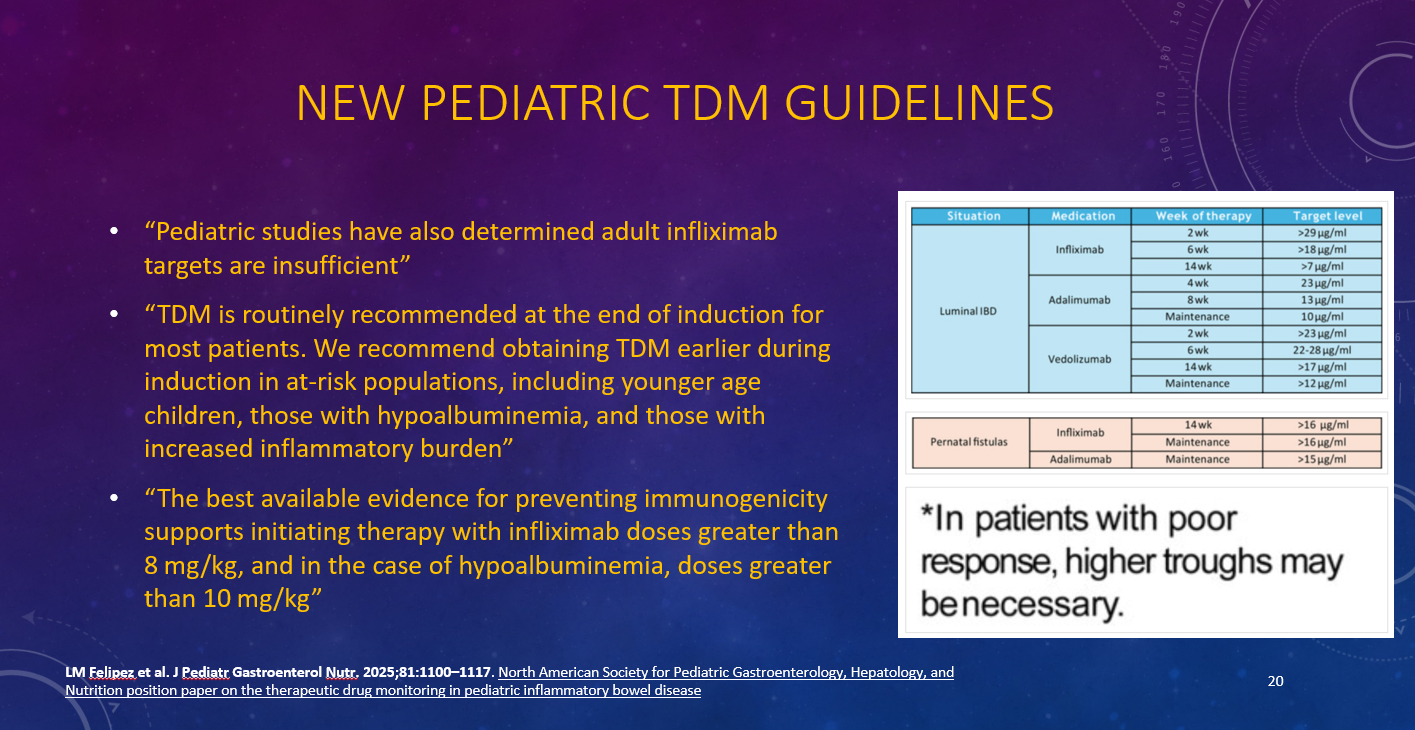
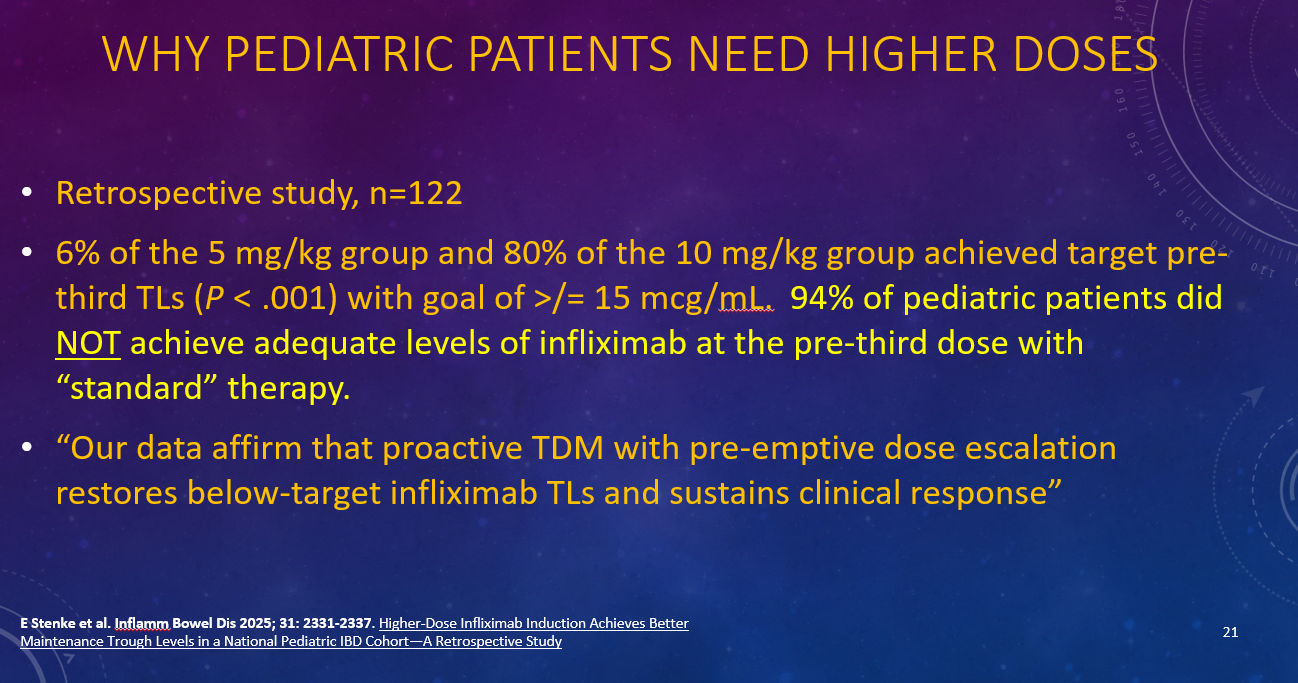
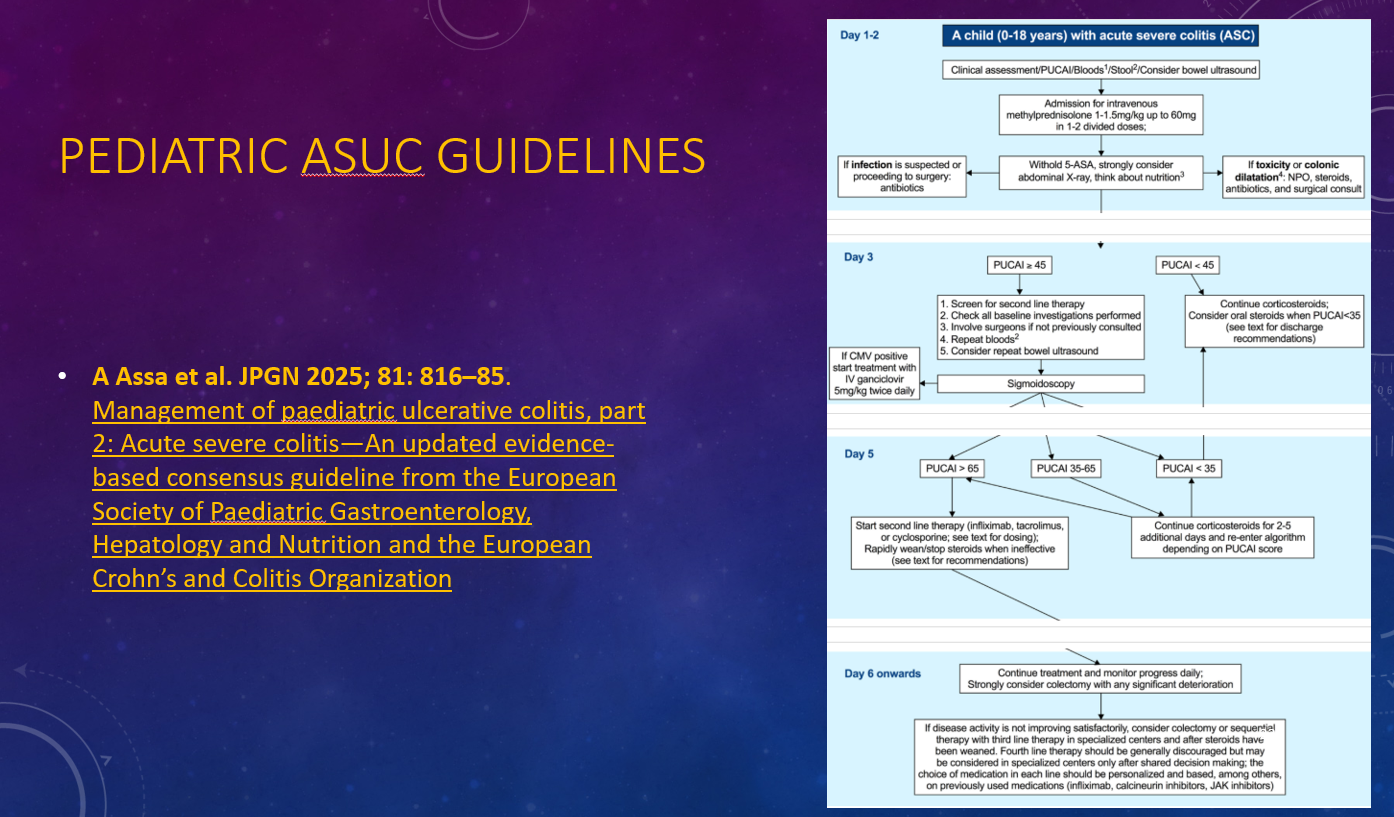
This year was the 2nd year that I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2025. All of the slides are based on studies or lectures that were reviewed on my blog, gutsandgrowth. Here are some of the slides:
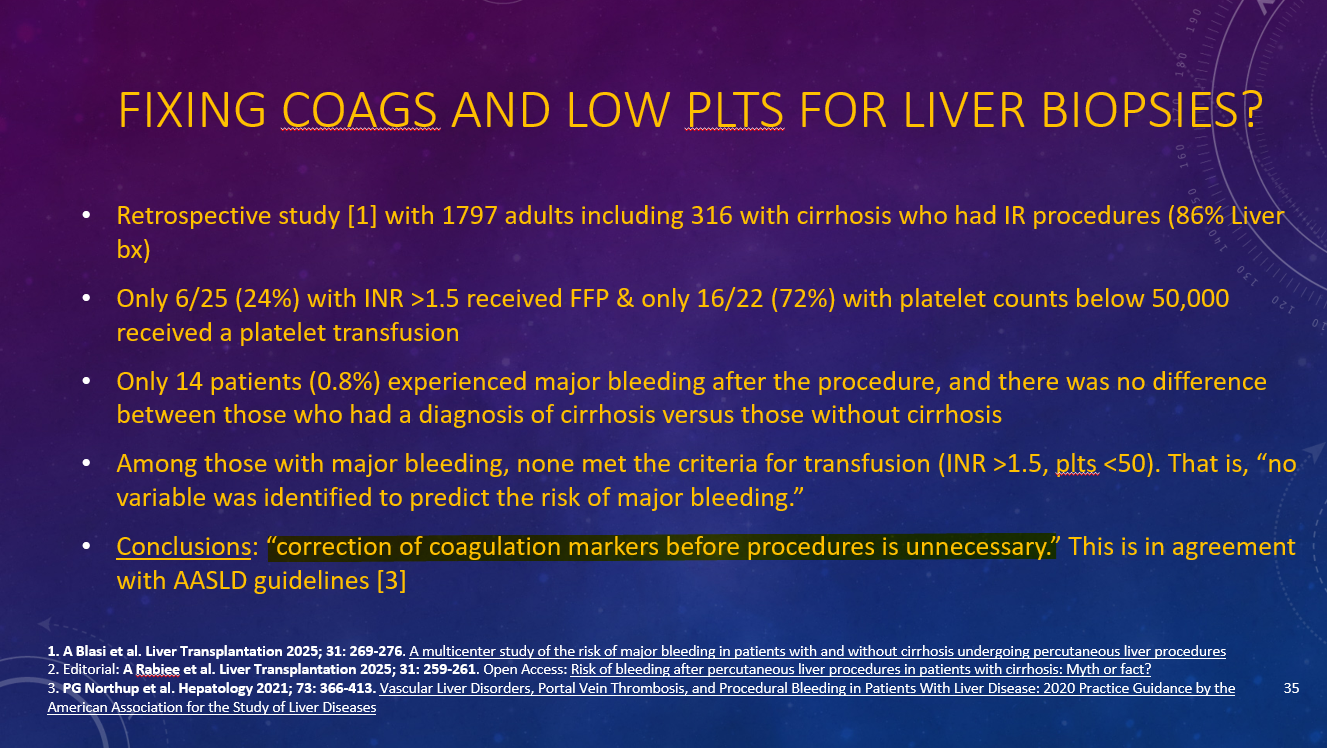
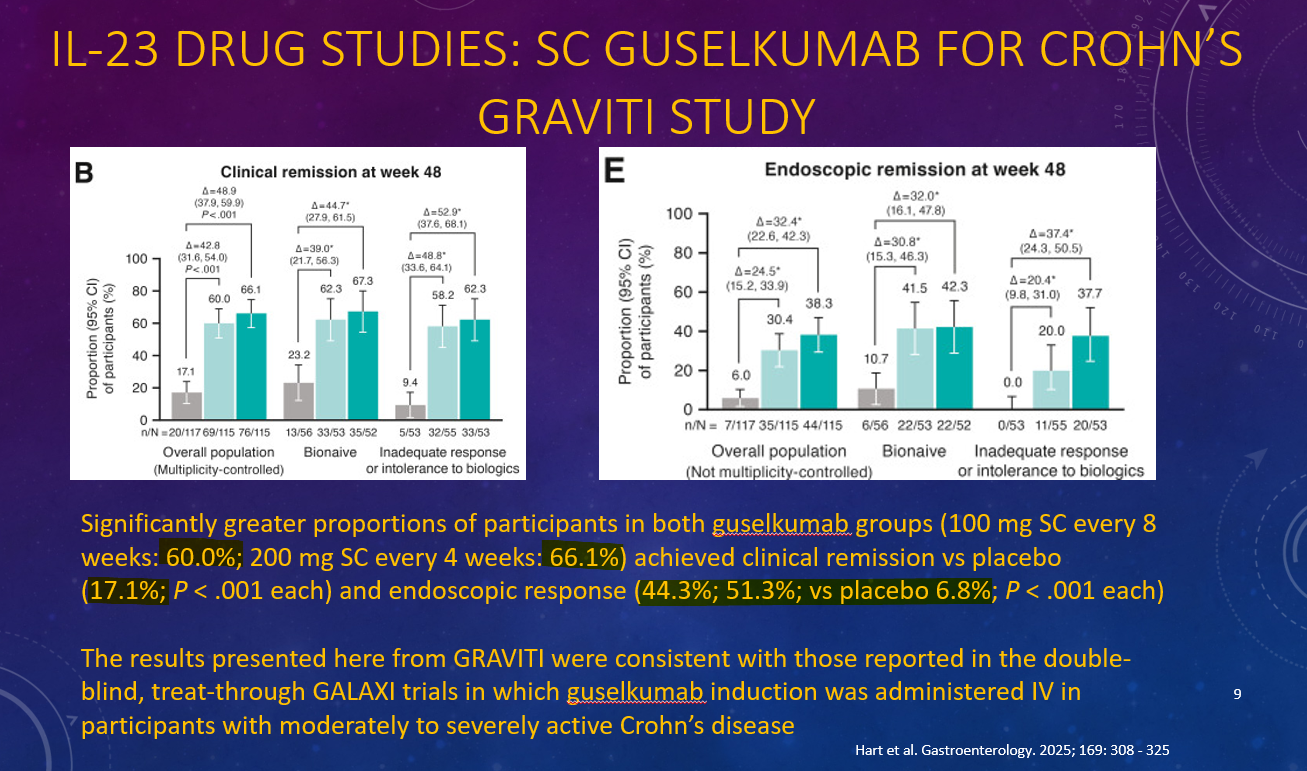
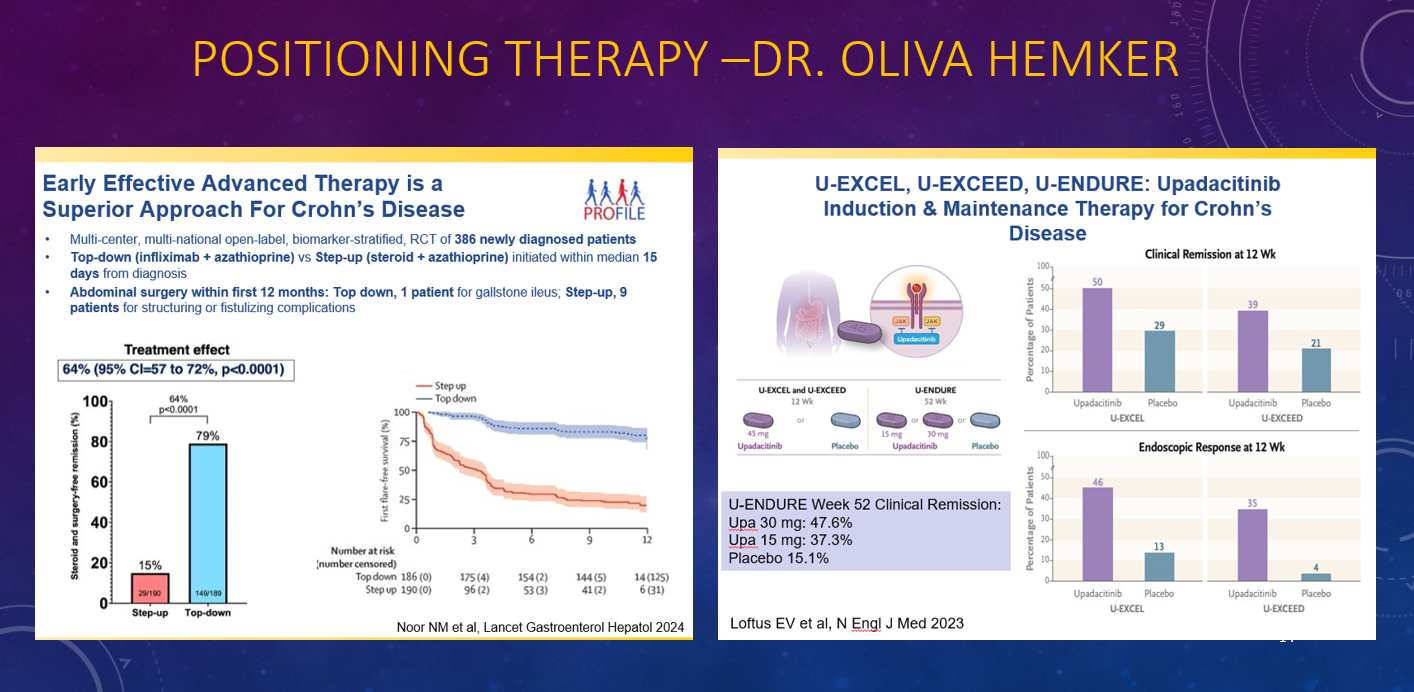
This year was the 2nd year that I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2025. All of the slides are based on studies or lectures that were reviewed on my blog, gutsandgrowth. Here are some of the slides:
It turns out that there has been a DBPC study for parachute use
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
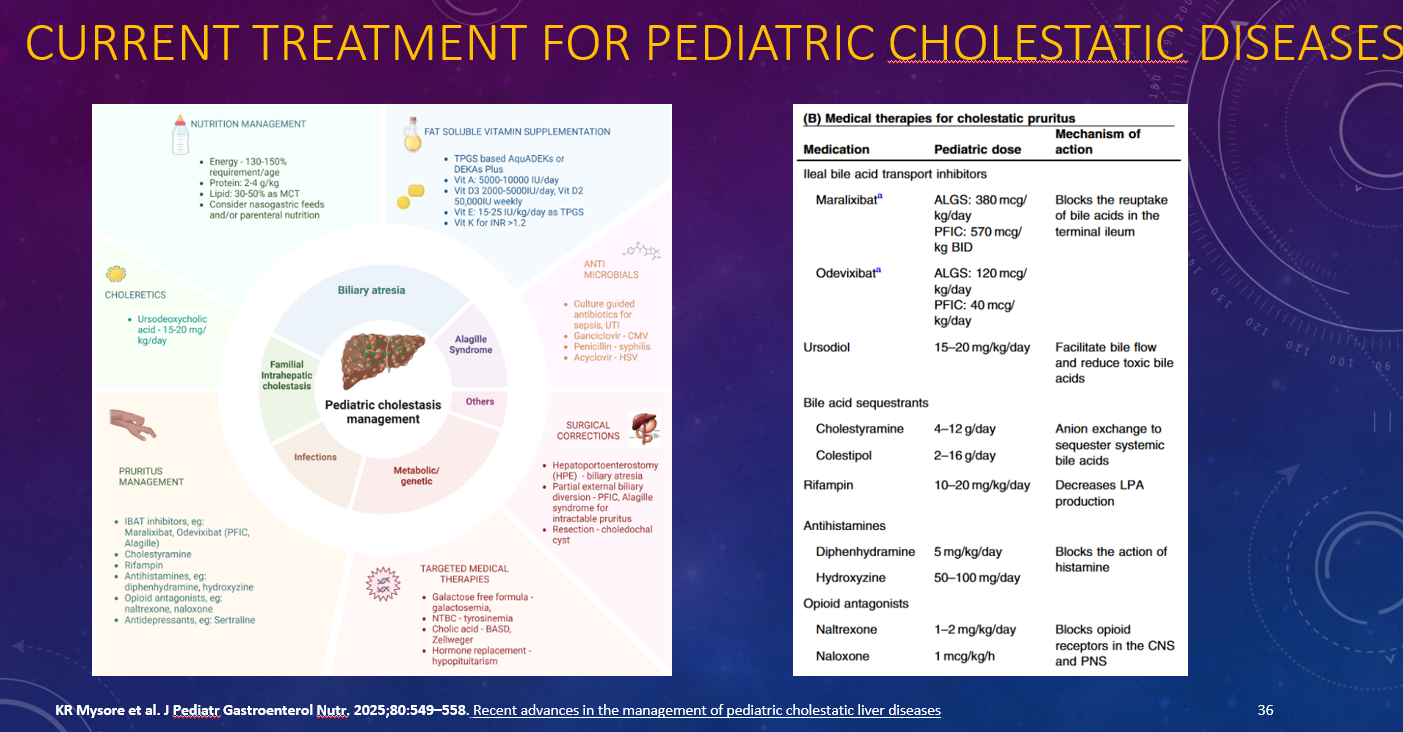
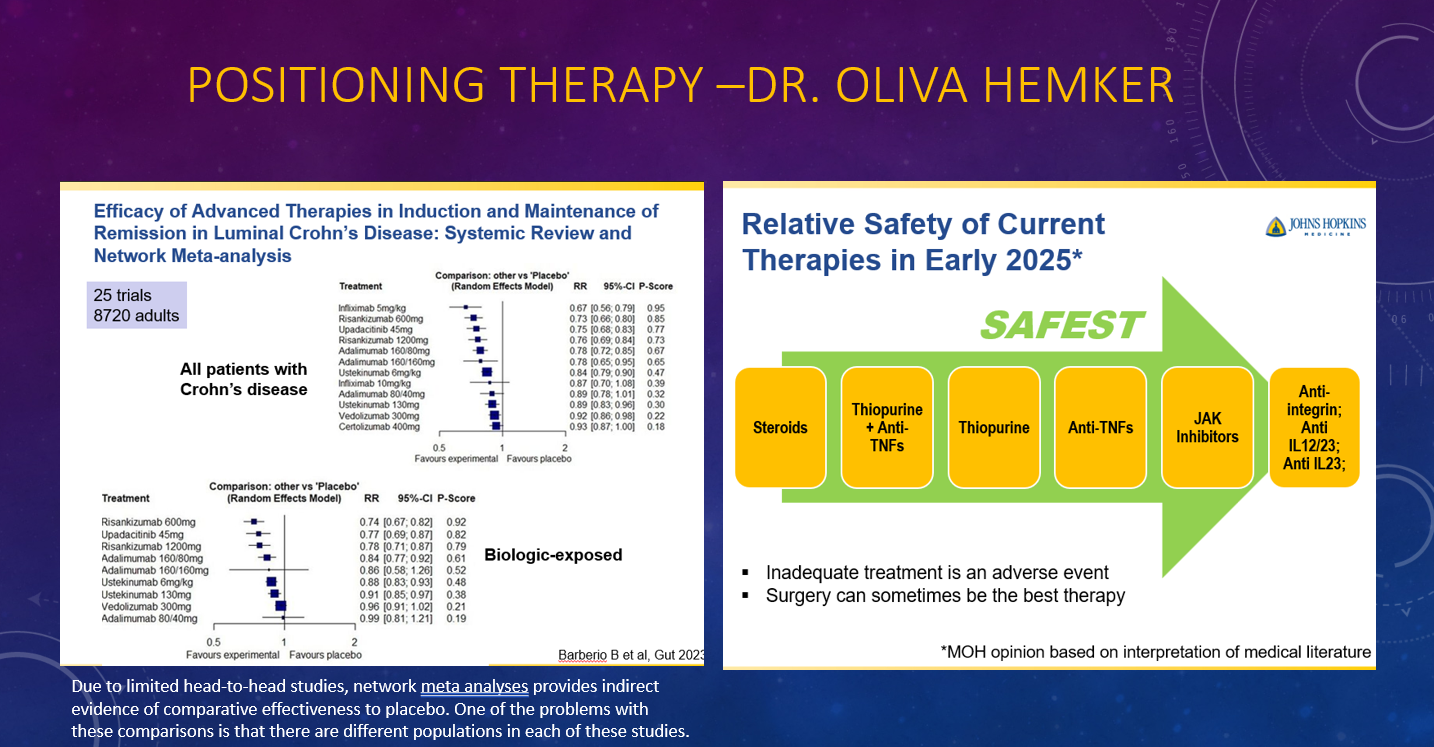
This year was the 2nd year that I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2025. All of the slides are based on studies or lectures that were reviewed on my blog, gutsandgrowth. Here are some of the slides:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
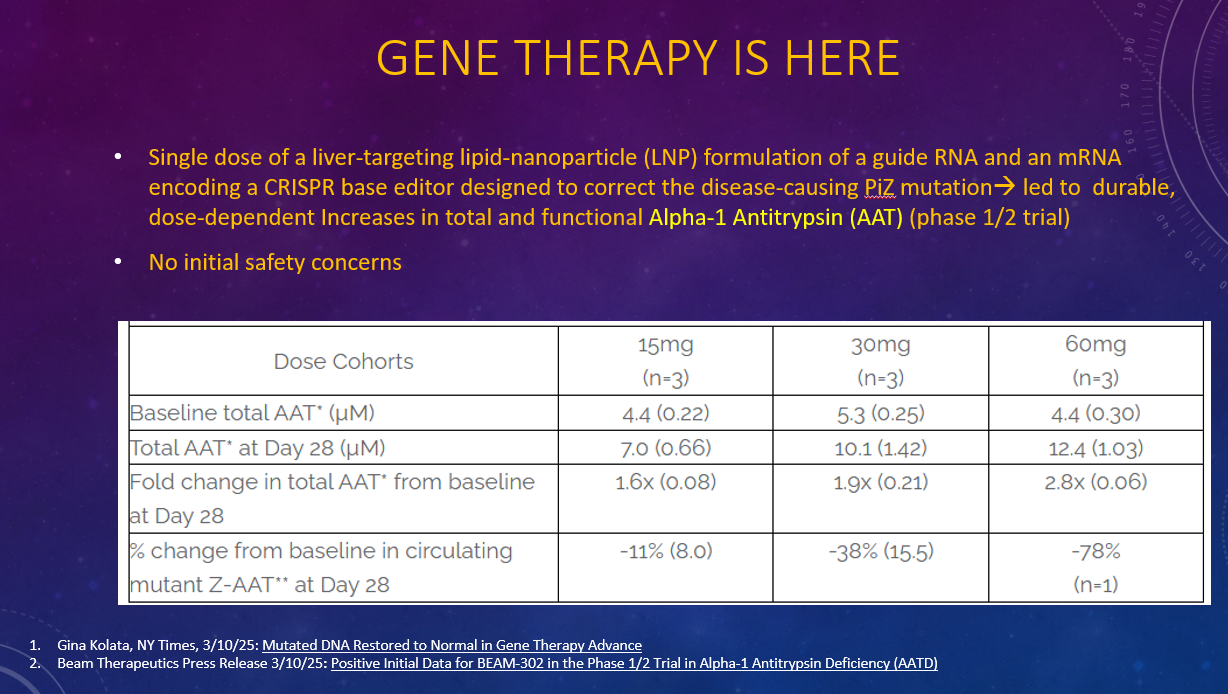
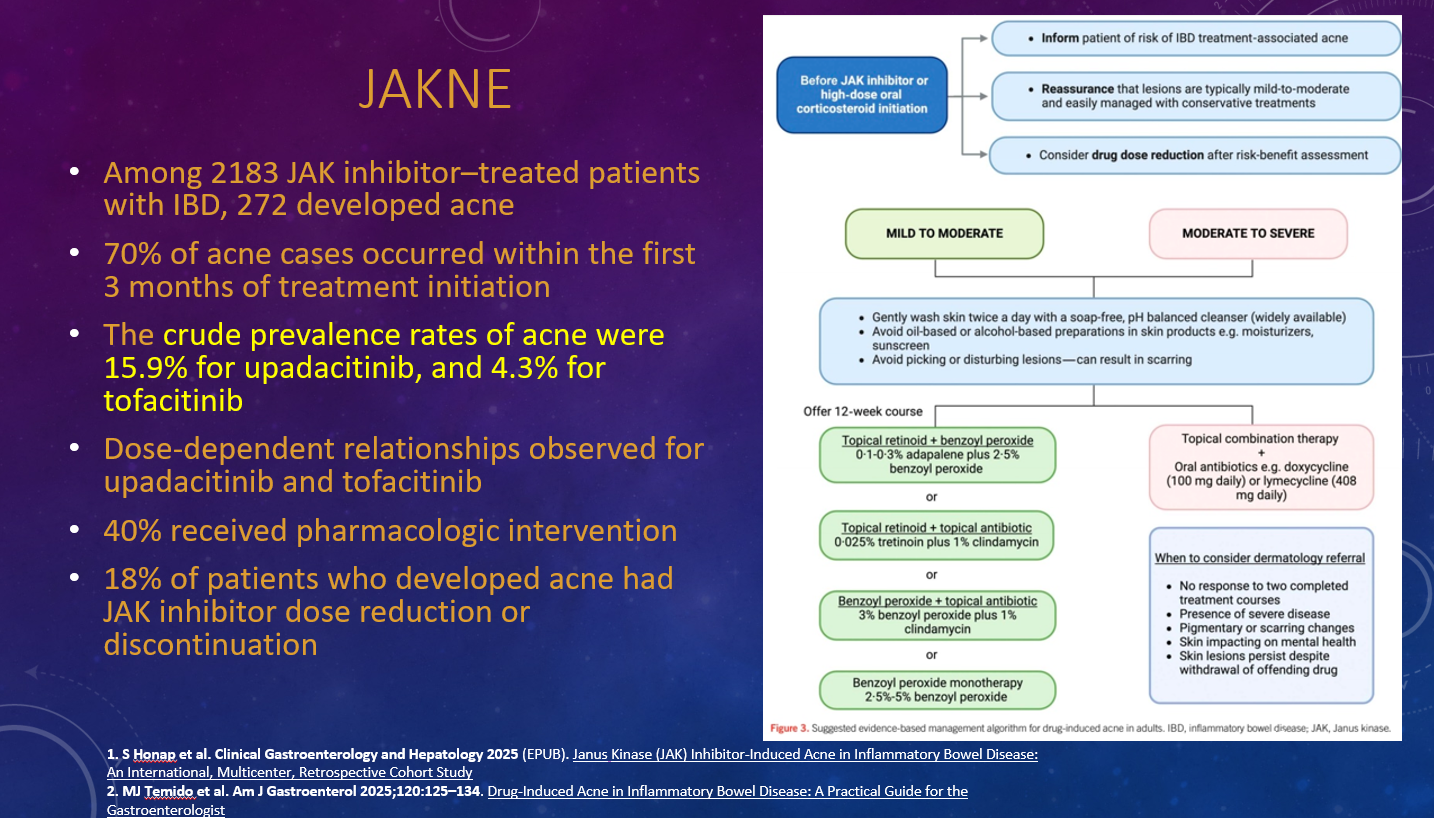
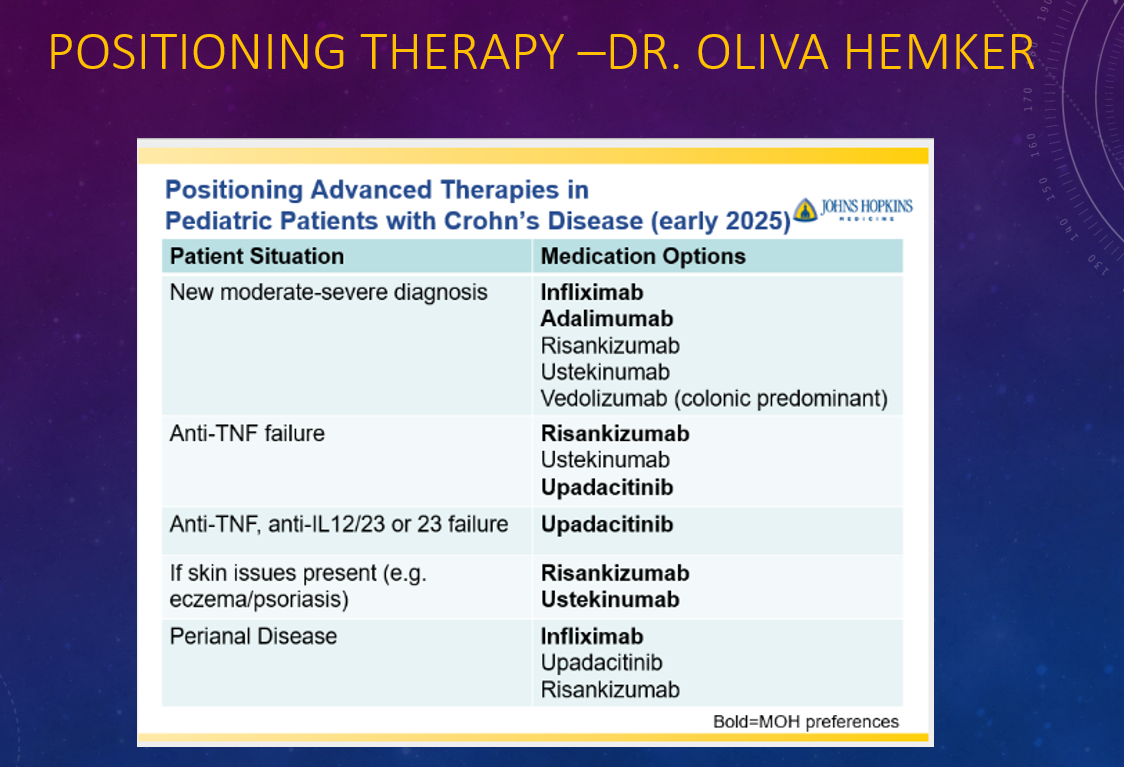
This year was the 2nd year that I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2025. All of the slides are based on studies or lectures that were reviewed on my blog, gutsandgrowth. Here are some of the slides:
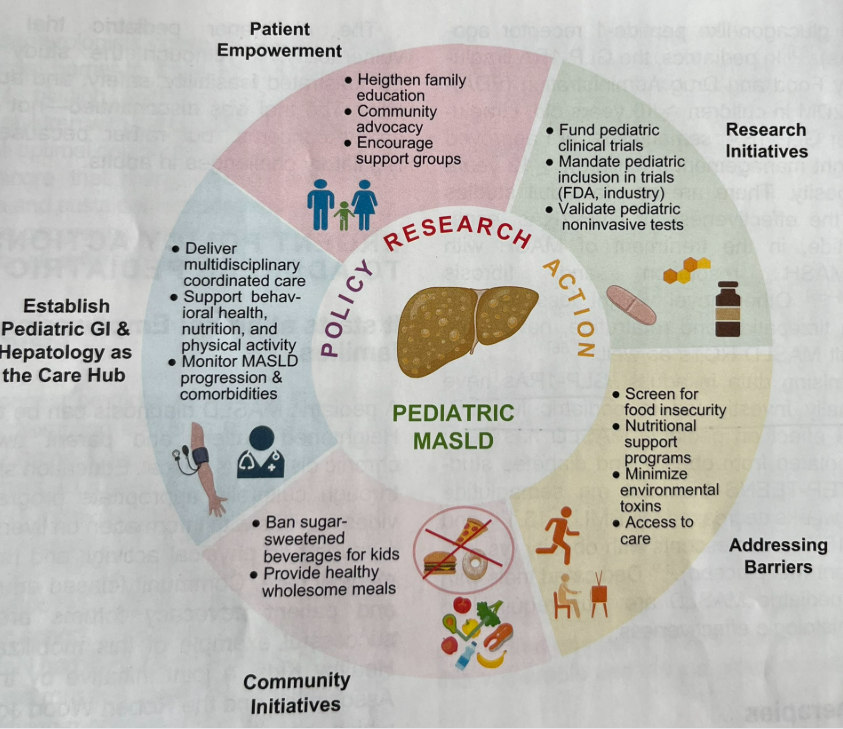
“Pediatric MASLD is still perceived as an indolent condition by many patients, families, and clinicians. In this Call to Action, we aim to raise awareness of pediatric MASLD as a public health crisis. Herein, we describe insufficient screening and disease staging practices, and a lack of accurate non-invasive tests and effective pharmacotherapy, both stemming from a paucity of multicenter clinical trials in pediatric MASLD.”
“GLP-1 RAs have not been formally investigated in pediatric MASLD.”
This was a retrospective study with 5 Latino adolescents obesity and MASLD who received semaglutide for at least 3 months. The range of BMI at the start of treatment was between 51 and 68.
Key findings:
There were clinically significant reductions in liver enzymes and APRI, a noninvasive marker of fibrosis. Specifically, mean ALT decreased by 38.4 IU/L (p < 0.01), mean AST decreased by 21.0 IU/L (p < 0.01), and mean APRI decreased by 0.128 (p = 0.01)
All 5 patients experienced weight loss with drop in BMI% from 2.3% to 14.2%
My take: This small study is consistent with others that show GLP1 RAs are likely to be an important tool for patients with MASLD. Current recommendations support use mainly in patients with comorbidities including obesity and T2DM.
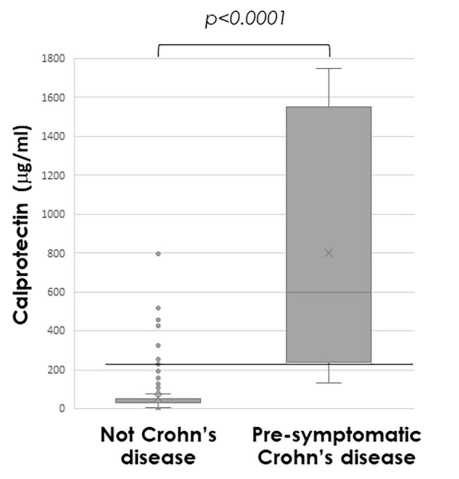
Methods: “Faecal calprotectin was measured in asymptomatic FDRs aged 6–38 years; those with persistent elevation, defined as >70 µg/g in at least two separate tests, were offered panenteric video capsule endoscopy or ileocolonoscopy”
Population: 331 (35%) first-degree relatives (FDRs) (from a group of 950) agreed to be screened: 63 (19%) had persistently elevated calprotectin, of whom 42 underwent further evaluation
Key findings:
From the initial screened cohort of 331 patients, nine (2.7%) had endoscopic appearance compatible with presymptomatic CD, and 22 (6.6%) had non-specific macroscopic mucosal changes
Median calprotectin was significantly higher in those with presymptomatic CD (772µg/g (IQR 279–1685)) compared with others (31µg/g (IQR 30–61), p<0.0001)
Calprotectin >225 µg/g predicted presymptomatic CD (area under the receiver operating characteristic curve 0.97 (95% CI 0.94 to 1.0; p<0.001; sensitivity 89%, specificity 94%)
Discussion Points:
“There is no universally accepted definition for preclinical stages of CD, and the distinction between these stages remains partly subjective.”
“The lack of longitudinal follow-up is also a limitation, but this will be completed as part of the PIONIR trial.”
My take (borrowed in part from the authors):
Identification of pre-symptomatic CD “can facilitate designing targeted interventions and defining inclusion criteria for prevention trials.” The disease may be more modifiable in the early stages of disease.
This trial suggests the calprotectin threshold of >70 is too low to target screening. For specificity, the study showed that persistent elevation above 225 merits investigation; though, it has been our practice to use a threshold of >150 for children older than 5 years.
Approximately 5% of asymptomatic FDRs of CD patients have evidence of pre-symptomatic CD and approximately 10% more have non-specific mucosal changes when evaluated
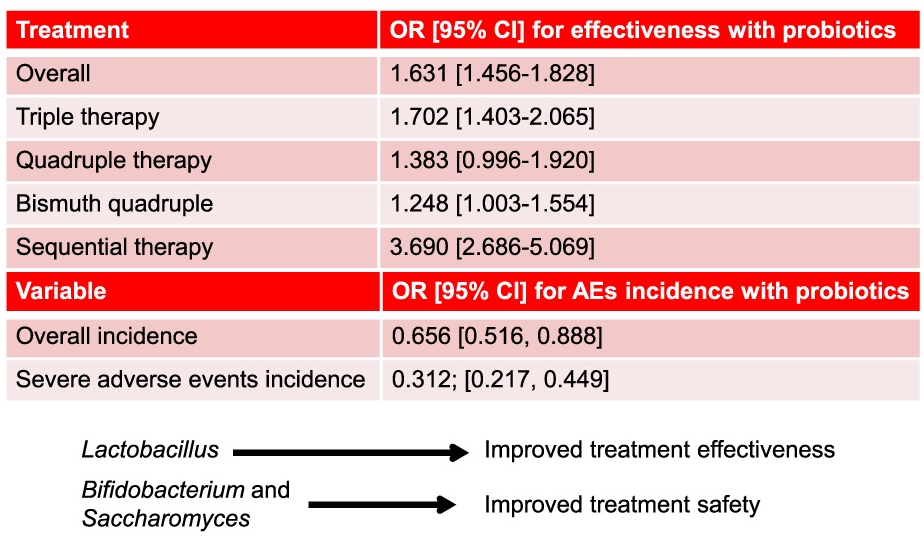
Methods: Prospective European registry with 36,699 treatments were recorded, where 8,233 (22%) were prescribed with probiotics. The analysis of the effectiveness of probiotics was restricted to those receiving first-line therapy.
Key findings:
Overall, the eradication rate was 90.6% with probiotics and 86.1% without probiotics.
With quadruple therapy, the eradication rate was 93.1% with probiotics and 89.3% without probiotics
Discussion Points:
“The prevalence of H pylori infection remains close to 45% in the European population”
The population receiving probiotics may have been expected to have a higher risk of eradication failure (eg. antibiotic resistance and more prior treatments) and/or higher expectations of adverse effects
This was NOT a randomized study which limits a more definitive conclusion on the effectiveness of adding a probiotic
My take: In highly-motivated families, probiotics may be worthwhile as part of an H pylori eradication regimen. This could, of course, necessitate changes in nomenclature. Would quadruple therapy with probiotics be called 5-drug (quintuple) treatment?
This article summarizes the recent changes in the treatment options for Clostridioides difficile (C diff).
Key points:
Fidaxomicin targets C diff with limited collateral microbiome disruption. This leads to significantly lower recurrence rates compared to vancomycin. Thus, it is preferred 1st line therapy for initial and recurrent C diff. In “the coming years, fidaxomicin is expected to come off patents” which will improve access and affordability.
Bexlotoxumab which lowered recurrence rate is no longer being produced
FMT via Openbiome is no longer available. In those in which FMT was used, options include the following:
live-jslm (REBYOTA), a broad consortium enema-based formulation
live-brpk (VOWST), a narrow consortium of Firmicutes in an encapsulated form. This treatment in adults: four capsules daily for three days
Both treatments are not recommended for patients who are severely immunocompromised. In these patients, prolonged vancomycin course with taper or using every other day therapy with fidaxomicin for days 7-25 could be considered
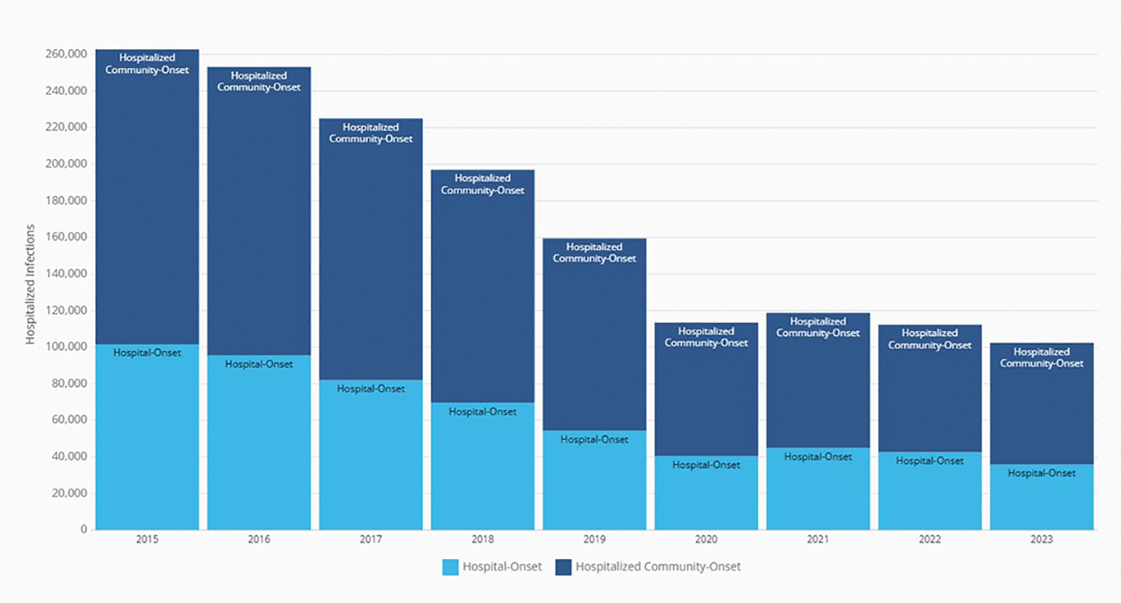
My take: I have been seeing less C diff cases recently. This may be due to better antibiotic stewardship, changes in C diff strains, or improved testing approaches.. My observation is supported by recent reports:
Annual number of hospitalized community-onset and hospital-onset CDI events reported to the National Healthcare Safety Network, 2015 to 2023. (From CDC’s Antibiotic Resistance & Patient Safety Portal (Available at https://arpsp.cdc.gov/profile/nhsn/cdi).)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.