BJ Griffiths et al. Clin Gastroenterol Hepatol 2025; 23: 1798-1807. Open Access (PDF)! Hypercoagulation After Hospital Discharge in Acute Severe Ulcerative Colitis: A Prospective Study
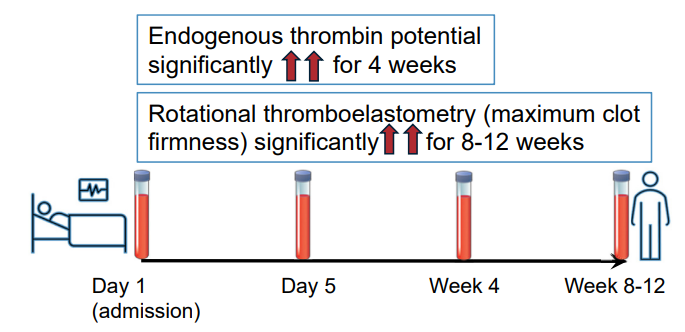
Methods: In this prospective study, twenty-seven adult patients with ASUC and 25 control patients with quiescent ulcerative colitis were recruited. Thrombin generation (endogenous thrombin potential), rotational thromboelastometry (EXTEM and FIBTEM maximum clot firmness), procoagulant factors, anticoagulant factors, and fibrinolytic markers were assessed for those with ASUC on admission (Day 1), Day 5, 4 weeks, and at 8–12 weeks. These assessments were performed on a single occasion for control patients.
Key findings:
Discussion:
- “Patients with ASUC had a hypercoagulable profile on initial presentation to the hospital, before receipt of LMWH, which was consistently demonstrated by individual and global assays of coagulation. The most marked elevations of individual factors at presentation were seen in the levels of Clauss fibrinogen, platelets, VWF, and FVIII, alongside heightened
levels of the inhibitors of fibrinolysis PAI-1 and TAFIa.” - “This hypercoagulable state persisted for many weeks after hospital discharge, with levels of FVIII, fibrinogen, VWF, and inhibitors of fibrinolysis (TAFIa) remained significantly elevated at all timepoints up to 12 weeks, compared with the control population. This is despite
intensive treatment for ASUC in all patients.” - “VTE and pulmonary embolism are 1 of the leading causes of morbidity and mortality during IBD flare-ups. The findings from this study reinforce the importance of thromboprophylaxis administration to all patients with ASUC at first presentation to hospital.”
My take: This study is in adults; the risk of VTE is lower in children and guidance on VTE prophylaxis is not clear.
Related blog posts:
- VTE Protocol for Hospitalized Kids with IBD (provides suggested pediatric protocol)
- Venous Thrombosis in Pediatric Inflammatory Bowel Disease | gutsandgrowth
- Latest on VTE in Pediatric IBD
- Thrombosis in Pediatric Patients with Intestinal Failure
- Ustekinumab in Pediatric Patients and More on VTE Prophylaxis
- Catheter-Related Venous Thromboembolism
- Venous Thromboembolism: A Good Question for Pediatric Collaboration
- VTE with IBD
- Neurological Complications Associated with Inflammatory Bowel Disease