About gutsandgrowth
I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
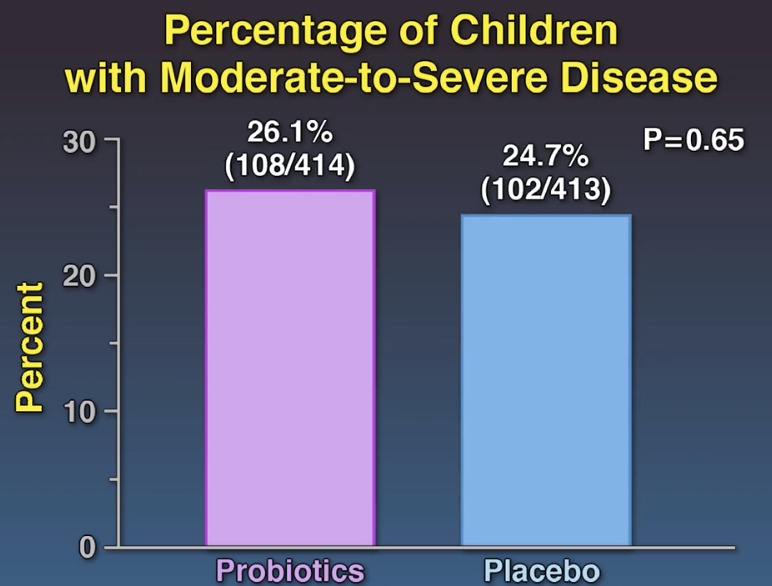
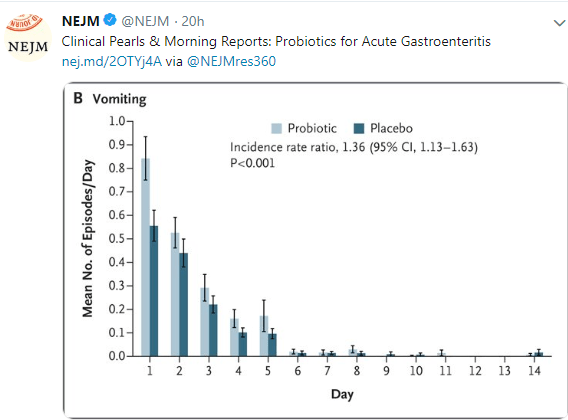
This blog post highlights a second study showing a lack of efficacy of probiotics for acute gastroenteritis. Link to 2 minute Summary: Quick Take on Probiotics for AGE
My take: While some probiotic strains have been shown to be helpful in some conditions (eg. antibiotic associated diarrhea), this study indicates that probiotics are likely ineffective in altering the course of acute gastroenteritis.
SB Freedman et al. N Engl J Med 2018; 379:2015-2026 Link to abstract: Multicenter Trial of a Combination Probiotic for Children with Gastroenteritis



Related blog posts:
My opinion has been that probiotics are generally over-hyped and are likely ineffective for many conditions in which they are commonly used (see related blog posts below).
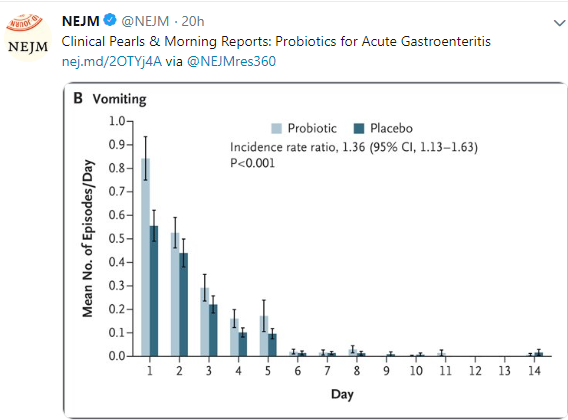
A recent study (D Schnadower et al.N Engl J Med 2018; 379:2002-2014) provided more data to support this skeptical view when probiotics are utilized for acute gastroenteritis. Another study in the same issue will be highlighted tomorrow and reaches a similar conclusion.
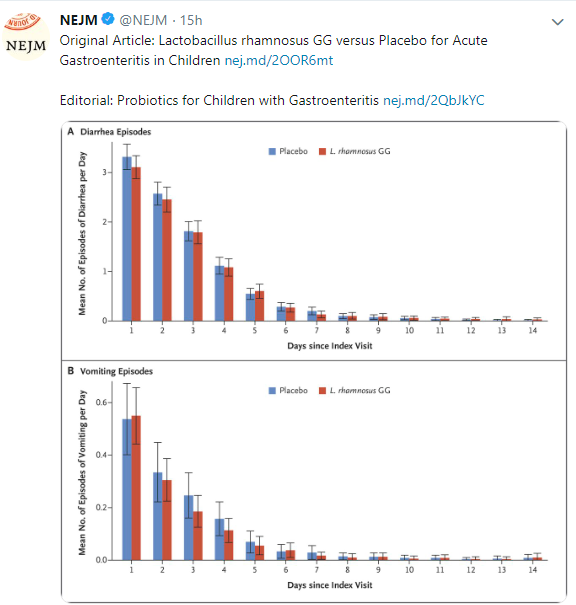
Link to Abstract: Lactobacillus rhamnosus GG versus Placebo for Acute Gastroenteritis in Children
METHODS: We conducted a prospective, randomized, double-blind trial involving children 3 months to 4 years of age with acute gastroenteritis who presented to one of 10 U.S. pediatric emergency departments. Participants received a 5-day course of Lactobacillus rhamnosus GG … twice daily or matching placebo…
RESULTS Among the 971 participants, 943 (97.1%) completed the trial…There were no significant differences between the L. rhamnosus GG group and the placebo group in the duration of diarrhea (median, 49.7 hours in the L. rhamnosus GG group and 50.9 hours in the placebo group; P=0.26), duration of vomiting (median, 0 hours in both groups; P=0.17), or day-care absenteeism (median, 2 days in both groups; P=0.67) or in the rate of household transmission (10.6% and 14.1% in the two groups, respectively; P=0.16).
CONCLUSIONS Among preschool children with acute gastroenteritis, those who received a 5-day course of L. rhamnosus GG did not have better outcomes than those who received placebo
My take: While some probiotic strains have been shown to be helpful in some conditions (eg. antibiotic-associated diarrhea), this study indicates that probiotics are likely ineffective in altering the course of acute gastroenteritis.

Related blog posts:
A recent systematic review and meta-analysis (J Dionne et al. Am J Gastroenterol 2018; 113: 1290-1300) throws some shade on the effectiveness of dietary therapies for irritable bowel syndrome. Thanks to Ben Gold for this reference. The authors reviewed 1726 citations -only 9 were eligible for systematic review; two RCTs (n=111 participants) with gluten-free diet (GFD) and 7 RCTs (n=397) with low FODMAPs diet.
Key findings:
- A GFD was associated with reduced global symptoms compared with control interventions (RR=0.42, CI 0.11-1.55) which was not statistically significant. Thus, there is “insufficient evidence to recommend a GFD to reduce IBS symptoms.”
- A low FODMAP diet was associated with reduced global symptoms compared with control interventions (RR=0.69, CI 0.54-0.88). The three RCTs with rigorous control diets found the least magnitude of effect. Thus, the overall quality of the data was “very low” according to the GRADE criteria.
Given the limited data supporting dietary therapy for IBS, the authors caution that in those who are placed on a low FODMAPs diet, that after a 2-6 week trial, those who “fail to improve should not continue the diet. ”
Related blog posts:


From a previous blog lecture from Athos Bousvaros (NASPGHAN Postgraduate Course 2014)
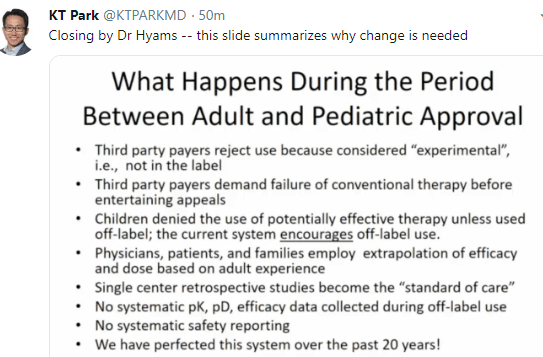
Off-label does not equate to experimental
FDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature.
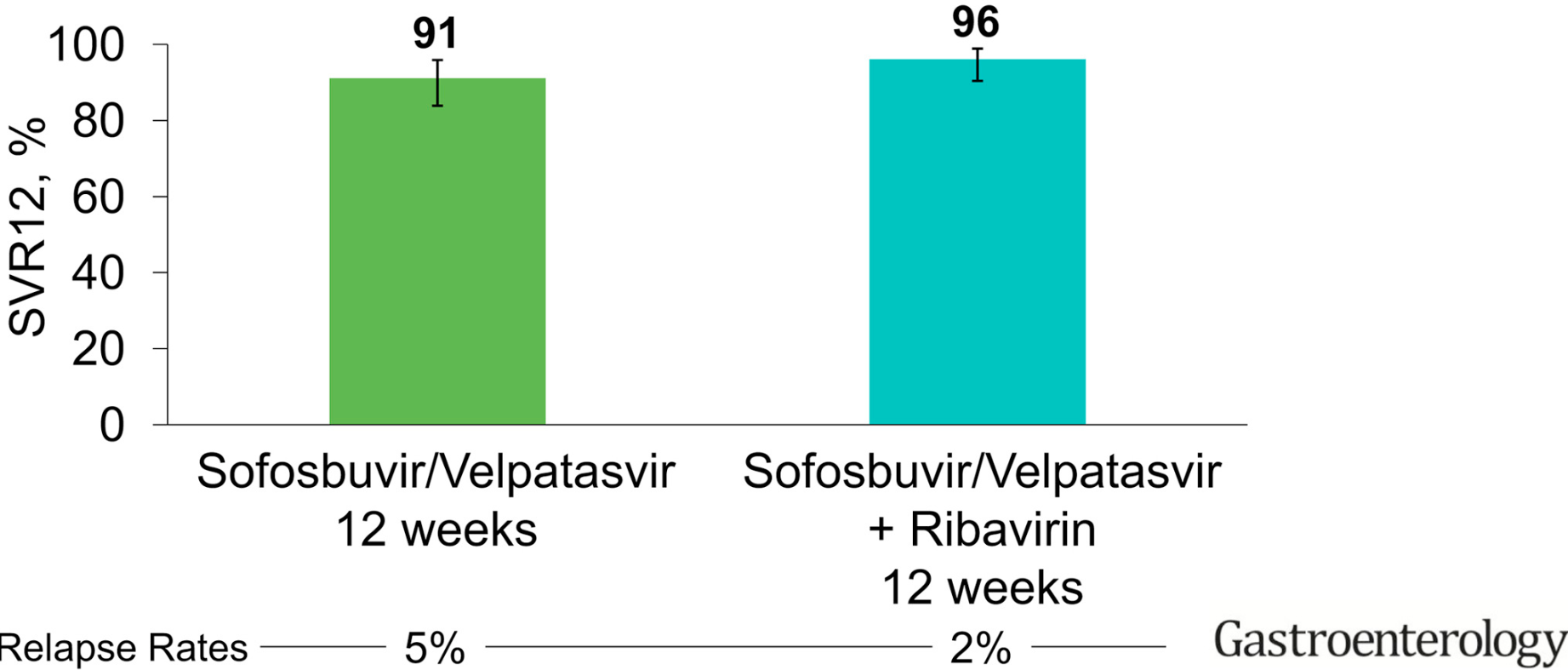
A recent study (R Esteban et al. Gastroenterol 20018; 155: 1120-7) evaluated the efficacy of sofosbuvir and velpatasvir in patients with hepatitis C genotype 3.
Overall, the study shows good efficacy of this regimen with and without ribavirin, though with higher SVR12 and lower relapse with the addition of ribavirin.
The difference in response was driven almost entirely based on whether there were pretreatment NS5A resistance-associated substitutions (RASs) present.
- In those with NS5A RASs the difference in response with added ribavirin compared to without was 96% vs 84%.
- In those without NS5A RASs the difference in response with ribavirin compared to without was 99% vs. 96%.
My take:
- If RAS testing is available and baseline Y93H is absent, then ribavirin is not likely needed
- Genotyping is still important. The associated editorial (pg 969-71) labeled genotype 3 ‘the problem child in the era of direct-acting antivirals.” That is, there are still differences in treatment recommendations based on HCV genotype.
Related blog posts:

DE Yung et al. Inflamm Bowel Dis 2018; 24: 2327-38. This systematic review and meta-analysis of four studies “did not detect an increased risk of postoperative complications with preoperative vedolizumab” (VDZ). This study included 281 patients who received VDZ.
SC Ng et al. Inflamm Bowel Dis 2018; 24: 2431-41. The authors examined the frequency of opportunistic infection among 4 VDZ trials and postmarketing surveillance, accounting for ~114,000 patient-years of exposure. The most common infection was C difficile (0.5 per 100 patient-years); tuberculosis was reported at 0.1 per 100 patient years. This study showed “that the rate of serious opportunistic infections in patients receiving VDZ was low and most patients could continue VDZ treatment.”
SL Gold et al. Gastroenterol 2018; 155: 981-2. This clinical image showed a case of Henoch-Schonlein Purpura (HSP) that developed in a 53 year receiving VDZ.
E Shmidt et al. Inflamm Bowel Dis 2018; 24: 2461-7. This retrospective review of a prospectively maintained IBD registry provides information of risk factors for VDZ loss of response and management. 444 patients out of 788 who received VDZ had a significant response.The majority of VDZ recipients 75) had failed prior anti-TNF Rx. Key points:
- Loss of response (LOR) at 6 months and 12 months was 20% and 35% respectively
- UC patients compared to Crohn’s disease (CD) patients were more likely to have LOR with R of 1.54.
- Shortening VDZ infusion interval from q8 weeks to q4-6 weeks recaptured response in 49% and led to remission in 18% of this cohort.
- LOR was more common (2-fold) among those who had a LOR to anti-TNF agent. Patients with primary nonresponse were less likely to have LOR with VDZ.
U Kopylov et al. Inflamm Bowel Dis 2018; 24: 2442-51. This retrospective multicenter study examined VDZ effectiveness among anti-TNF naive patients, n=184.
- For CD, 42/50 (82%) responded by week 14, and 32 (64%) were in clnical remission. At last followup (30-52 weeks), clinical remission was noted in 24/35 (69%)
- For UC, 116/134 (79%) responded at week 14 and 53 (40%) were in clinical remission. At last followup (30-52 weeks), 67% were in remission (69/103)
The authors conclude that VDZ is similarly efffective for anti-TNF naive CD and UC patients.
My take: These studies show that we still have a lot to learn about the effectiveness of VDZ as its use becomes more widespread.
Related blog posts:

Jasper, Canada
Briefly noted: U Krishnan et al. Analysis of eosinophilic esophagitis in children with repaired congenital esophageal atresia. JACI 2018. Published online Oct 24, 2018.
This retrospective, single-center study examined 4 eosinophilic esophagitis (EoE) study cohorts and identified EoE in 20 of 110 patients (18%) who had surgically-repaired esophageal atresia.
This association has been seen previously: World J Gastroenterol. 2014 Dec 21; 20(47): 18038–18043. This case study stated ” We are suggesting that EoE is a frequent concomitant problem in patients with history of congenital esophageal deformities, and for this reason any of these patients with refractory reflux symptoms or dysphagia (with or without anastomotic stricture) may benefit from an endoscopic evaluation with biopsies to rule out EoE.”

Related blog posts:
A recent commentary (MH Wallenstein, DK Stevenson. JAMA Pediatr. 2018;172(11):1004-1005.) discusses the potential advantages of transpyloric feedings in premature infants. Thanks to Ben Gold for this reference.
Key points:
- First, preterm infants are highly susceptible to pulmonary aspiration, primarily due to, among other factors, immature tone of the lower esophageal sphincter and use of uncuffed endotracheal tubes.”
- Second, aspiration of gastric contents probably contributes to bronchopulmonary dysplasia..
- Third, transpyloric feeding is an effective strategy to reduce the risk of aspiration…we believe that early prophylactic transpyloric feeding may be the only effective strategy to prevent aspiration-associated lung injury.
- Transpyloric feedings “fell out of favor in the 1980s after a single trial showed an increased risk of mortality”
My take (borrowed from authors): “the practice of early transpyloric feeding with human breastmilk merits a thorough reevaluation of its risks and benefits in the setting of modern neonatal practice.”

More from Banff

When I place an order for an upper GI, the computer prompt asks whether this should be with or without a scout film. A recent retrospective study (S Abdullah et al. JPGN 2018; 67: 576-9) provides data indicating that the default setting should be without a scout xray.
After reviewing UGIs in 197 outpatients over a 2 year period, the authors found that
- 97% found no significant findings in scout xray
- 1.5% (n=3) had findings that were not addressed
- 1% (n=2) had findings that required additional evaluation –both minor lung findings, later deemed insignificant
- 0.5% (n=1) had a finding which resulted in a change in management –>a cleanout for excessive stool. The report does not state whether this patient had a rectal exam which generally is more accurate with regards to the need for a cleanout
My take: This study provides convincing data that scout studies are usually unnecessary. For inpatients, the main reason to order a scout xray would be if a patient had previous contrast that needs to be cleared prior to UGI.
Related blog post: Pre-PEG UGIs Often Unnecessary

Lake Maligne, near Jasper Canada

A recent editorial (B Koletzko et al. JPGN 2018; 67: 561-3) explain why pureed fruit/food pouches can be detrimental for child health. An easy-to-read editorial in NY Times discusses some of the same issues –Link: Rethinking Baby Food Pouches
Key points:
- Pouches may interfere with learning to eat from a spoon.
- Feeding infants “a variety of food textures and lumpy foods by spoon feeding and finger foods provides great opportunities for intensive reciprocal interaction between parent and infant”
- These products generally have high energy density, high sugar content, and a very sweet taste and likely predispose towards bad food choices/selection as the child gets older.
- Also, these food pouches may increase the risk of dental caries
Additional points from NY Times:
- The popular pouches, introduced about a decade ago, now account for 25 percent of baby food sales in the United States, according to Nielsen’s Total Food View.
- The features that make pouches so convenient, though — the smooth texture and squeeze packaging — have some experts concerned. They caution against relying on them too much, saying that they can be a gateway to bad long-term snacking habits and routine overeating
- If given these pouches when irritable, children also run the risk of learning to associate sweet snacks with calming down, and to think of snacking in general as an activity to satisfy emotional rather than physiological needs.
- “Feeding is truly a developmental process, just like learning to crawl, walk, run. We would never do anything to keep a child from crawling,” Ms. [Melanie] Potock [a feeding specialist] said. “Let’s not do anything that would stall them in the development of eating.”