I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
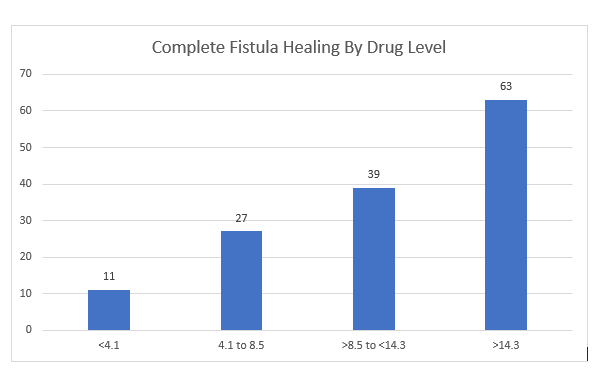
In this multicenter retrospective review with 183 patients, the adalimumab (ADM) levels were examined with respect to healing of perianal fistulas. Most patients (82%) had complex perianal fistulizing CD.
Key findings:
87 patients (48%) received intensified dosing at the time of therapeutic drug monitoring (TDM)
Patients with complete fistula healing (CFH) had higher median ADM levels: 12.9 compared to 6.1 for those witout CFH
“Optimal ADM concentration associated with CFH was 12.2 mcg/mL” which had positive predictive value of 64% and negative predictive value of 80%. Among those with ADM >12.1, CFH was achieved in 64% compared to 20.5% in those with concentrations <12.1 (Odds ratio, 5.7). “Even higher drug levels may be needed.”
There were 46 patients in each drug level category
My take: There is a lot of data supporting TDM, including proactive TDM, with anti-TNF agents like adalimumab and infliximab. This study shows that with fistulizing disease higher drug levels are needed to achieve better outcomes.
From Caitlyn Rivers Newsletter, Force of Infection 11/4/24:
Norovirus is high and increasing right now. Nationally, test positivity is at nearly 12%. To put this in context, the peak last year was 13.6%. Rates are particularly high in the Southern region.
A reminder as cases increase: norovirus causes stomach pains, diarrhea, and vomiting. It is extremely transmissible via bodily fluids and through contaminated surfaces, food, and water.
To reduce your odds of getting sick, remember to wash your hands frequently with soap and water for at least 30 seconds (norovirus is able to withstand hand sanitizer).
If you or someone in your household becomes sick, wash hard surfaces with soap and water or a diluted bleach mixture, and wash soiled clothing and linens in hot water and then dry on high heat.
Norovirus is still highly transmissible for several days after symptoms improve or go away. As such, insofar as is possible, avoid preparing food for others for at least 72 hours after symptoms end. Longer is better: it can spread up to two weeks after symptoms end, though it is most transmissible during those first few days of illness and after symptoms resolve.
In this observational prospective cohort with 114 children (after excluding 6), outcomes following the first episode of acute pancreatitis (AP) were determined. In addition, pancreatitis risk genes (CASR, CEL, CFTR, CLDN2, CPA1, CTRC, PRSS1, SBDS, SPINK1, and UBR1) were sequenced. A genetic risk score was derived from all genes with univariable P < .15.
Pre-DM was defined as follows: fasting blood glucose ≥100 mg/dL and <126 mg/dL, or hemoglobin A1C ≥5.7% and <6.5%
Key findings:
95/114 (83%) remained normoglycemic and 19/114 (17%) developed endocrine insufficiency (4 DM, 15 pre-DM) 12 months after the first episode of AP
Sixty-three subjects (52.5%) had at least 1 reportable variant identified
Severe AP (58% vs 20%; P = .001) and at least 1 gene affected (79% vs 47%; P = .01) were enriched among the endocrine-insufficient group
CFTR (53%), SPINK1 (13%), PRSS1 (10%), and UBR1 (9%) accounted for the majority of variants identified
My take: 3.5% of this cohort developed diabetes and 13% developed prediabetes. The risk is increased in those with severe acute pancreatitis and underlying genetic variants. As noted recently with Dr. Freeman’s lecture (summarized on prior blog posts), it is worthwhile for patients to follow-up after an episode of acute pancreatitis.
“A new report by the Commonwealth Fund finds some US states have firearm death rates comparable to countries in conflict…For instance, Mississippi’s rate of firearm-related violence (28.5 per 100,000 people) was nearly double that of Haiti (15.1 per 100,000) in 2021…
Rhode Island, which has the lowest firearm death rate in the US (three per 100,000) is still 23 times higher than the United Kingdom (0.13 per 100,000) and nearly 1.3 times higher than France (2.3 per 100,000).
The US overall is in the 93rd percentile of all countries and territories for overall firearm mortality, at 13.5 deaths per 100,000 people…
In another example, Mississippi, Louisiana, Alabama and New Mexico all have higher firearm mortality rates than Mexico, where decades of violence between state forces and rival drug cartels has caused hundreds of thousands of deaths and left more than 115,000 people missing…
More than half of all firearm-related deaths (56.1%) in 2022 were from suicide…the rate of firearm deaths among American children is 72 times higher in the US than in the UK (36.4 deaths per million versus 0.5 deaths per million)
My take: The fact that the U.S firearm mortality rates can be compared unfavorably to places with violent reputations like Haiti and Mexico is awful. What’s worse is the capitulation by most to not even try to improve the situation.
No Exaggeration: Too Many Children Are Dying in the U.S. (2019) “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
Yesterday’s pumpkin -please no snide remarks about how I can now retire and become a sculptor:
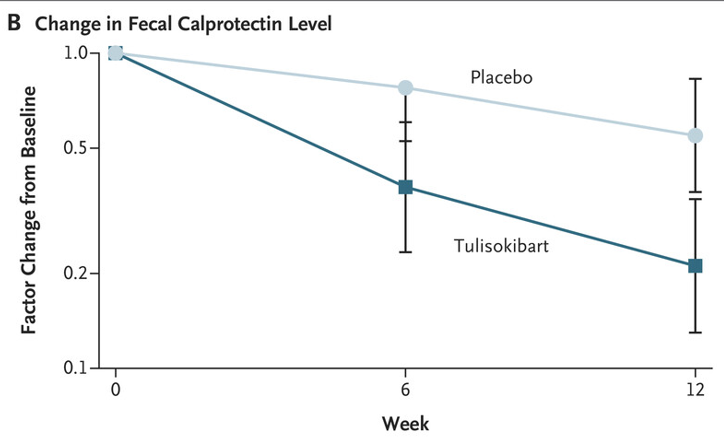
BE Sands et al. N Engl J Med 2024;391:1119-1129. Phase 2 Trial of Anti-TL1A Monoclonal Antibody Tulisokibart for Ulcerative Colitis
Background: “Several studies have implicated human tumor necrosis factor–like cytokine 1A (TL1A) in the pathogenesis of inflammatory bowel disease…Tulisokibart (formerly PRA023) is a humanized IgG1 kappa monoclonal antibody that binds to the membrane-bound and soluble forms of TL1A with high affinity and specificity. Tulisokibart prevents the interaction of TL1A and DR3, thereby suppressing type 1 and type 17 helper T-cell responses, increasing regulatory T-cell activity, and decreasing profibrotic pathways.”
Methods: (ARTEMIS-UC trial) The authors “randomly assigned patients with glucocorticoid dependence or failure of conventional or advanced therapies for ulcerative colitis to receive intravenous tulisokibart (1000 mg on day 1 and 500 mg at weeks 2, 6, and 10) or placebo. Cohort 1 included patients regardless of status with respect to the test for likelihood of response. Cohort 2 included only patients with a positive test for likelihood of response.”
“The inclusion of an integrated assessment of a panel of genetic markers as a diagnostic assay was based on the notion that patients with a propensity to overexpress TL1A might be more likely to have a response to tulisokibart than an unselected population.”
Key findings:
In the first cohort, a significantly higher percentage of patients who received tulisokibart had clinical remission than those who received placebo (26% vs. 1%), endoscopic healing (31% vs. 4%), endoscopic improvement (37% vs 6%) and clinical response (66% vs 22%)
“Among patients with a positive test for likelihood of response (cohorts 1 and 2 combined), clinical remission occurred in a higher percentage of patients who received tulisokibart than in those who received placebo (32% vs. 11%).”
Improvement in CRP and Calprotectin were noted as early as 2 weeks and 6 weeks respectively
The incidence of adverse events was similar in the tulisokibart and placebo groups
My take: Tulisokibart was effective in a group of patients with moderately to severely active ulcerative colitis who were refractory to advanced therapies.
The researchers found a 25.6% drop in people undergoing bariatric surgery in the final six months of 2023 compared with the number of surgeries people had during the same period the year before. During the latter half of 2023, the number of patients who took a glucagon-like peptide 1, or GLP-1 medication for weight loss, surged by more than 130%, according to a study published Friday in JAMA Network Open…Another popular weight loss drug, Eli Lilly’s Zepbound, was not included because the Food and Drug Administration did not approve it until November 2023…[And there are] anecdotal reports of hospitals that shut down bariatric surgery programs as the number of patients seeking operations slumped…
In 2022, nearly 280,000 metabolic and bariatric procedures were performed in the United States, according to the American Society for Metabolic and Bariatric Surgery. That represented about 1% of all U.S. residents eligible for weight loss operations…The CDC estimates that about 40% of U.S. residents have obesity and 1 in 10 have severe obesity.
Reference: Lin, K., et al. (2024). Metabolic Bariatric Surgery in the Era of GLP-1 Receptor Agonists for Obesity Management. JAMA Network Open. doi.org/10.1001/jamanetworkopen.2024.41380.
Methods: This cross-sectional study, we used 2022 to 2023 deidentified claims from 17 million unique deidentified adult patients with medical and pharmaceutical coverage through commercial and Medicare Advantage insurance in the OptumLabs Data Warehouse. We included only patients without diabetes and with obesity.
**Only 6% of patients with obesity in the study population received either GLP-1 drugs or surgery, suggesting that many more patients could be receiving treatment.
My take: The GLP-1 drugs have established a medical therapy with a good probability of effectiveness. This was lacking from prior medical treatments. It certainly is logical that their availability could reduce the use of bariatric surgery. The AAP may need to revise their bariatric surgery recommendations from 2020.
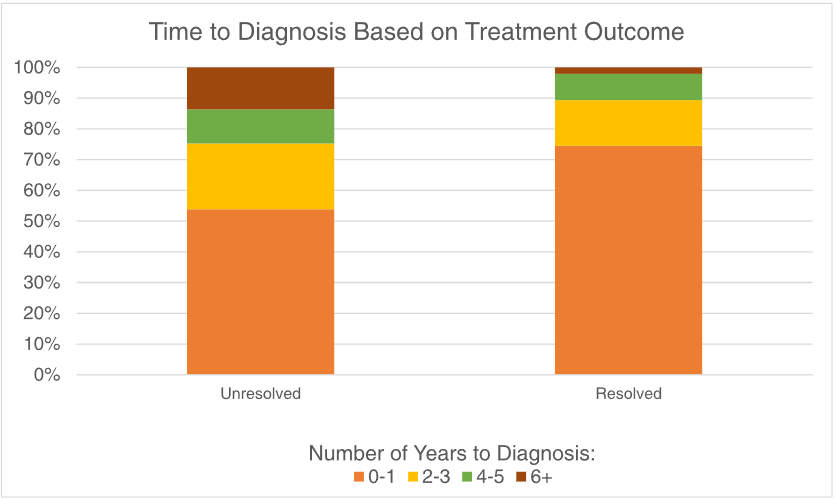
MR Jia et al. J Pediatr Gastroenterol Nutr. 2024;79:850–854. Delay in diagnosis is associated with decreased treatment effectiveness in children with rumination syndrome
In this retrospective single-center study with 247 patients, the authors evaluated whether the time from symptom onset to diagnosis over time and whether it was associated with symptom resolution.
Key findings:
The median age at symptom onset was 11 years and median age at diagnosis was13 years
Among the 164 children with outcome data, 47 (29%) met criteria for symptom resolution after treatment
A longer time to diagnosis was associated with a lower likelihood of symptom resolution after treatment (p = 0.01)
In the discussion, the authors note that “we suspect that one contributing factor to worse outcomes associated with diagnostic delays is the excessive testing leading to over‐medicalization of DGBIs…Our findings are the first to show that diagnostic delay contributes to poorer outcomes in children with RS, which highlights the importance of a timely diagnosis.” In fairness to the authors, other parts of the manuscript state that the delay in diagnosis is associated with worse outcomes but does not attribute causality.
Limitations:
The patient cohort is derived from a specialized referral center (Nationwide Children’s)
Recall bias
My take:
While I concur that a timely diagnosis of rumination syndrome is useful, it is unproven that a delayed diagnosis contributes to a worse outcome. The outcome differences could more easily be explained by a selection bias. Patients who never recovered from rumination symptoms previously may be less likely to respond to treatment regardless of when treatment is instituted. Perhaps attributing poor outcomes to delayed diagnosis, rather than a selection bias, is due to a confirmation bias.
Another important finding is that the more than 70% of patients did NOT have resolution of their symptoms. Realizing that many patients have some symptoms after treatment helps gastroenterologists set reasonable goals.
Methods: Two randomized, placebo-controlled, double-blind studies were conducted in patients with moderately to severely active CD or UC and inadequate response or intolerance to corticosteroids and immunomodulators. All patients received open-label CT-P13 IV 5 mg/kg at weeks 0, 2, and 6. At week 10, clinical responders were randomized (2:1) to CT-P13 SC 120 mg or placebo every 2 weeks until week 54 (maintenance phase) using prefilled syringes.
Key findings:
At week 54 in the CD study, statistically significant higher proportions of CT-P13 SC–treated patients vs placebo-treated patients achieved clinical remission (62.3% vs 32.1%; P < .0001) and endoscopic response (51.1% vs 17.9%; P < .0001)
In the UC study, clinical remission rates at week 54 were statistically significantly higher with CT-P13 SC vs placebo (43.2% vs 20.8%; P < .0001).
CT-P13 SC was well tolerated, with no new safety signals identified.
The mean serum infliximab trough concentrations at weeks 14 and 54 were 13.2 and 14.8 mcg/mL with CD study and 14.6 and 16.3 with UC study, respectively.
Proportions of patients achieving co-primary and key secondary end points at week 54 in the CD study (all randomized population)Proportions of patients achieving primary and key secondary efficacy end points at week 54 in the UC study (all randomized population)
Discussion:
“The present findings are generally comparable with or numerically better than those observed in previous clinical trials that evaluated IV infliximab in patients with CD or UC…At week 50 in the SONIC trial, 35% of patients receiving infliximab achieved corticosteroid-free clinical remission,30 compared with 40% of patients in the CT-P13 SC group in the current study.”
“In terms of UC, the ACT 1 study4 found that patients receiving infliximab 5 mg/kg and 10 mg/kg were more likely to achieve clinical remission based on total Mayo score after 54 weeks (34.7% and 34.4%, respectively) compared with participants receiving placebo (16.5%), and in the current study, 43.2% and 20.8% of patients, all of whom had responded to induction therapy, achieved clinical remission at week 54 in the CT-P13 SC and placebo groups, respectively.”
This study had a high rate of antidrug antibody detection (63.8%–65.1%)…” likely due to the use of highly sensitive, next-generation ADA assays, which have improved sensitivity compared with those used in historical studies… This suggests that route of administration of CT-P13 does not affect rates of ADA formation, and that the observed incidence of ADA is not unexpected.”
“The decision to initiate CT-P13 SC maintenance therapy at week 10, 4 weeks after finishing CT-P13 IV induction therapy, was based on results of PK or pharmacodynamic model simulation.”
My take: These studies suggest that SC infliximab is likely to have similar efficacy as IV infliximab
A Simard et al. J Pediatr Gastroenterol Nutr. 2024;79:800–806. Role of ileal diversion in pediatric inflammatory bowel disease
Indications:
Severe, medically refractory colitis
Complex and medically refractory perianal disease
In combination with bowel resection for irreversible bowel damage (e.g., fistulae, abscesses, or strictures)
Diversion “provides the opportunity to reduce steroid use, improve growth and observe the natural history of the disease in a more controlled manner. It may also enhance quality of life”
My take: This is a handy article when considering ileal diversion in a patient with medically-refractory inflammatory bowel disease.