A recent study (SJ Spechler et al. NEJM 2019; 381: 1513-23) on first glance appears to support surgery as more effective than medical treatment for refractory heartburn.
Only ~20% of enrolled patients were included in the reported outcomes!
Here’s what happened. Among a cohort of VA patients (n=360, mean age 48 years) who were reportedly refractory to PPI-treatment:
- 78 were excluded during prerandomization
- 42 had relief of their heartburn during a 2-week omeprazole lead-in (20 mg BID)
- 70 did not complete trial procedures
- 23 had non-GERD disorders
- 99 had functional heartburn
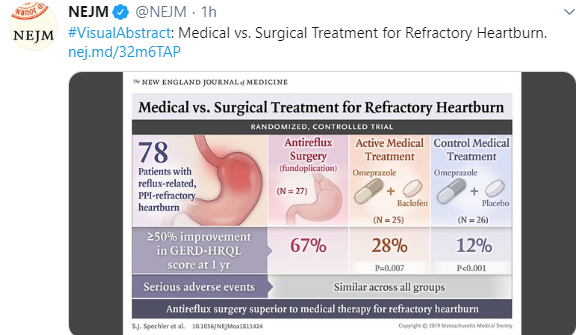
This left 78 patients who underwent randomization. All patients in this highly-selected group had undergone endoscopy with biopsy, impedance-pH testing, and esophageal manometry. 18 of 27 (67%) had treatment success with surgery compared to 7 of 25 patients treated with baclofen/PPI and 3 of 26 with control medical treatment (PPI alone).
Key points:
- Careful evaluation is needed in any patient with refractory heartburn, especially if contemplating surgery. Most will either respond to PPI treatment or have a disorder other than reflux; the authors note that 122 patients (out of 360 patients) did NOT have reflux –99 had functional heartburn.
- Careful instruction in PPI use can be helpful. Omeprazole and similar agents should be taken 30 minutes before meals.
- The authors noted that in addition to reflux, that reflux hypersensitivity can “respond to fundoplication…treatment success was 71% among the 14 with reflux hypersensitivity and 62% among the 13 with abnormal acid reflux.”
Limitations: The VA population is not representative of the general population; this trial had a predominance of white males. Also, it is hard to exclude that some of the ‘success’ of the procedure could relate to a powerful placebo response.
My take: This trial reinforces the notion that reflux surgery is helpful in very few highly-selected patients.
Related blog posts:
- What’s Going On in Patients with Reflux Who Fail to Respond to PPIs?
- How Many Kids with Reflux Actually Have Reflux?
- Why didn’t patient with documented reflux get better with PPI …
- Failure of PPI test | gutsandgrowth
- Guidelines on Functional Heartburn
- Better to do a coin toss than an ENT exam to determine reflux
- How Likely is Reflux in Infants with “Reflux-like … – gutsandgrowth
- PPI Webinar
- The Connection Between Anxiety and Gastroesophageal Reflux Disease