A recent double-blind, double-dummy study (ES Dellon et al. Gastroenterol 2019; 157: 65-73) found similar efficacy between budesonide and fluticasone for newly-diagnosed eosinophilic esophagitis. They had hypothesized that an oral viscous budesonide would be more effective due to increased esophageal contact time.
Methods: The authors compared an oral viscous budesonide OVB) at 1 mg BID (n=56) to fluticasone (swallowed) MDI dosed at 880 mcg BID (n=55). Patients aged 16-80 years, with mean of 37 years.
Baseline characteristics:
- ~95% in both groups with dysphagia
- ~75% with any atopic condition
- ~50% with dilatation required at baseline
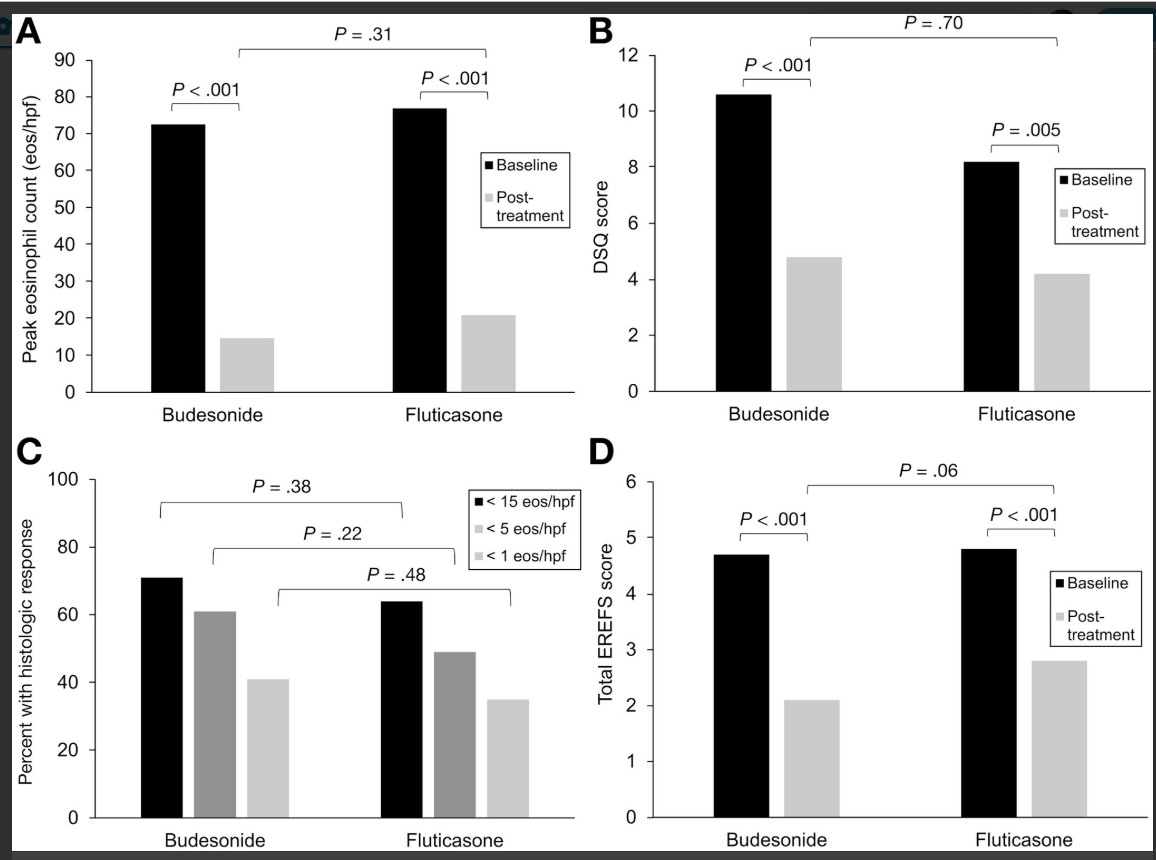
Key findings:
- Similar drop in eosinophil count: 73 (OVB) and 77 (MDI) eos/hpf at baseline to 15 and 21 respectively
- Histologic response (<15 eos/hpf) rates of 71% (OVB) and 64% (MDI).
- Response to <5 eos/hpf occurred in 61% OVB and 49% MDI; response to <1 eos/hpf was noted in 41% and 35% respectively
- Symptom scores (DSQ) responded similarly as well
- Similar degree of candidiasis 12% for OVB and 16% for MDI
In the associated editorial, the authors speculate that one reason for similar efficacy was the detailed instructions given for patients taking the MDI.
My take: This study supports both topical steroid therapies; practical issues like cost and insurance coverage could be influential in selecting the specific treatment for an individual patient.
Related blog posts:
- Orodispensable Budesonide Tablets for Eosinophilic Esophagitis
- Surprising Findings in Prospective Study of Budesonide in EoE Study
- What Happens When Topical Steroids are Stopped in EoE
- Neglibible Effect of Eosinophilic Esophagitis Treatment on Longitudinal Growth
- What is EoE?
- EoE Update 2018 (Dr. Seth Marcus)
- Updated Consensus Guidelines for Eosinophilic Esophagitis
- A Better Budesonide for Eosinophilic Esophagitis
- A Better Budesonide for Eosinophilic Esophagitis (Part 2) | gutsandgrowth
- Dilatation for Eosinophilic Esophagitis -Pediatric Data | gutsandgrowth
- Adrenal Insufficiency due to Fluticasone in … – gutsandgrowth
- Higher Doses of Topical Steroids for Eosinophilic … – gutsandgrowth
From AGA twitter feed