In the REPREVIO study, a double-blind, randomized, placebo-controlled trial, 80 adults received either vedolizumab (300 mg IV) (n=43) or placebo (n=37) at weeks 0, 8, 16 and 24 following ileocolonic resection and had one or more risk factors for recurrence.
Key findings:
At week 26, the probability of a lower modified Rutgeerts score with vedolizumab versus placebo was 77·8% (95% CI 66·4 to 86·3; p<0·0001).
Severe endoscopic recurrence was observed in ten (23·3%) of 43 patients in the vedolizumab group versus 23 (62·2%) of 37 patients in the placebo group (difference –38·9% [95% CI –56·0 to –17·3]; p=0·0004).
Adverse effects were noted in three patients who received vedolizumab (bilateral tubo-ovarian abscesses, thrombosed hemorrhoids, and pancreatic adenocarcinoma) and two patients who received placebo (intestinal perforation related to Crohn’s disease and severe abdominal pain)
My take: This study shows that vedolizumab is another biologic capable of reducing postoperative recurrence following ileocolonic resection in Crohn’s disease. Infliximab has been shown to reduce recurrence as well (shown in the PREVENT study).
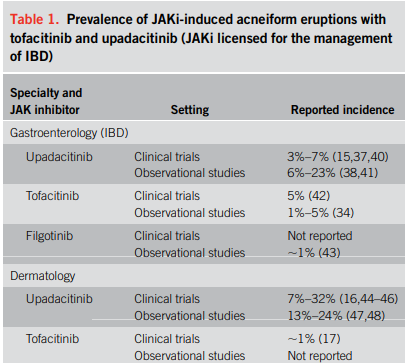
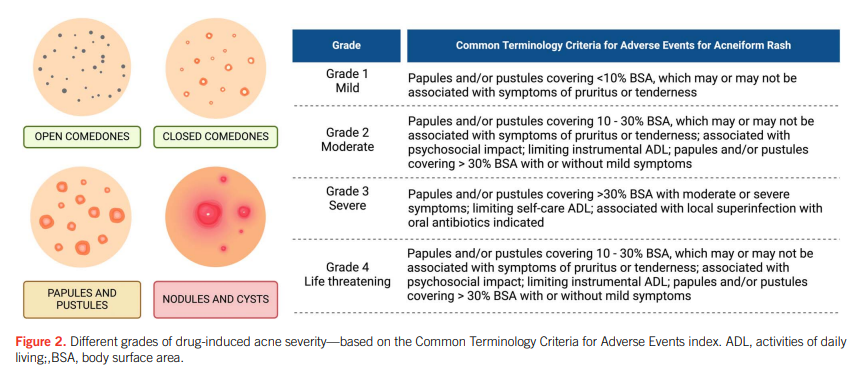
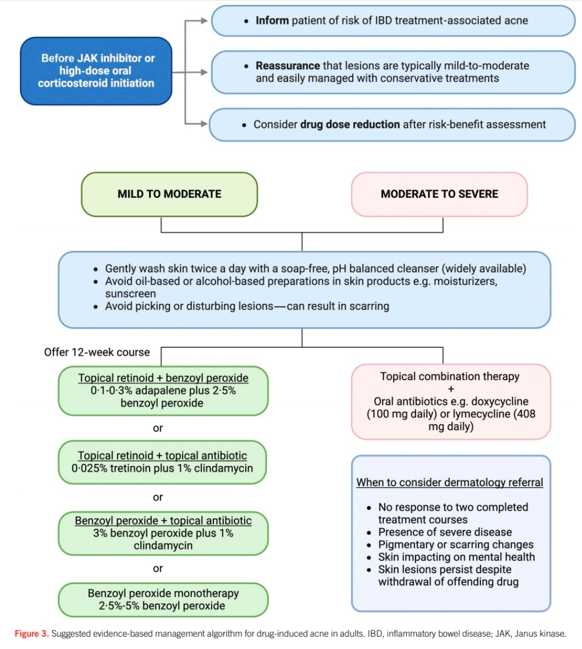
“Corticosteroids and Janus kinase inhibitors (JAKi) are commonly used for the treatment of inflammatory bowel disease (IBD) and are known to aggravate a prior tendency to acne or trigger the development of new acneiform eruptions. Both randomized controlled trials and real-world studies have identified acne as one of the most common treatment-emergent adverse events in JAKi… This review examines the characteristics of drug-induced acne in IBD treatments, provides a practical guide for gastroenterologists to manage mild-to-moderate occurrences, and highlights when to seek specialist dermatology advice.”
My take: This is a helpful review of acne management in the setting of IBD.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This was a retrospective chart review of patients who underwent serological testing for suspected Alpha-Gal Syndrome (AGS) between 2014 and 2023 at Mayo Clinic. Of 1260 patients who underwent testing,124 tested positive for AGS. –matched with 380 seronegative control subjects. 40 patients had long-term followup data available
Key findings:
AGS patients reported a higher frequency of tick bites (odds ratio [OR], 26.0)
AGS patients reported a higher prevalence of urticaria (56% vs 37%; P = .0008)
A total of 47% experienced at least 1 GI symptom, such as diarrhea, nausea, vomiting, abdominal pain, abdominal cramps, bloating, heartburn, and constipation, in descending order of frequency
11% of AGS patients presented solely with GI symptoms
After institution of red meat restriction, 22 of 40 were asymptomatic at followup, 14 of 40 were improved, and 4 of 40 reported no improvement. 7 of the asymptomatic group were able to resume a diet without restrictions.
Discussion point:
“Symptom onset in AGS typically occurs more than 4 hours after allergen exposure, with studies emphasizing a tight association with delayed reactions within the 3- to 6-hour range.”
My take: This study provides some more granular data on Alpha-gal and highlights the importance of asking about tick bites and urticaria in patients with possible AGS.
For a lot of patients with rheumatologic complaints like joint pain, treatment often consists of sending patients to physical therapy rather than using pharmaceuticals. This type of approach is under-utilized in gastroenterology. A recent study, however, suggests that an analogous approach is likely beneficial in patients with chronic laryngopharyngeal symptoms.
Background: Laryngopharyngeal symptoms such as cough, throat clearing, voice change, paradoxic vocal fold movement, or laryngospasm are hyper-responsive behaviors resulting from local irritation (e.g., refluxate) and heightened sympathetic tone. Laryngeal recalibration therapy (LRT) guided by a speech-language pathologist (SLP) provides mechanical desensitization and cognitive recalibration to suppress hyper-responsive laryngeal patterns.
Methods: Adults (n=65, mean age 55 years) with chronic laryngopharyngeal symptoms referred for evaluation of GERD to a single center were prospectively followed. Inclusion criteria included ≥2 SLP-directed LRT sessions (60 minutes sessions). “Mechanical desensitization focuses on well-known laryngeal suppression techniques (i.e. pursed lip breathing to suppress throat clearing or cough) or changing voice production by means of acoustic and aerodynamic techniques…Cognitive recalibration uses relaxation and conceptualization of symptoms to rework thought patterns around chronic laryngeal behaviors.”
Key findings:
Overall, 55 participants (85%) met criteria for symptom response. 17 (26%) had complete resolution, 19 (29%) had near-complete resolution, and 19 (29%) had a moderate response
Specifically, symptom response was similar between those with isolated laryngopharyngeal symptoms (13/15, 87%) and concomitant laryngopharyngeal/esophageal symptoms (42/50, 84%)
My take: Historically, patients with laryngopharyngeal symptoms have been difficult to treat. Many do not respond to reflux therapies. This study highlights a different approach and shows that the benefit of working with highly-skilled SLPs.
Background: “Guselkumab is a dual-acting, human IgG1, interleukin-23p19 subunit inhibitor that potently neutralises interleukin-23 and can bind to CD64.”
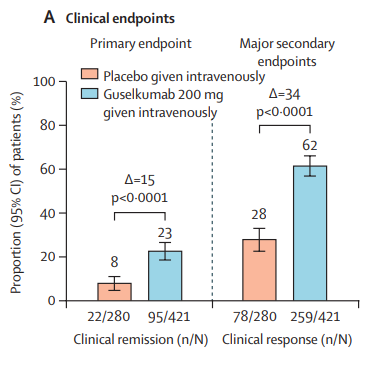
Methods: “Two phase 3, randomised, double-blind, placebo-controlled studies (QUASAR phase 3 induction and maintenance) included randomised and treated adults with moderately to severely active ulcerative colitis (induction baseline modified Mayo score from 5 to 9) with inadequate response or intolerance to conventional or advanced ulcerative colitis therapy.”
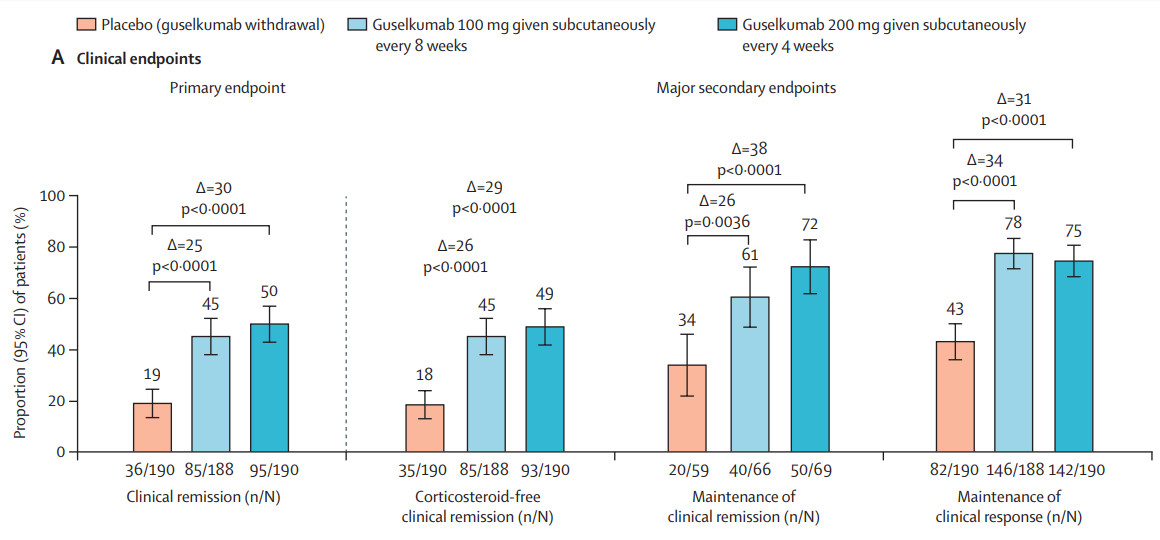
“The induction study primary population included 701 patients (guselkumab 200 mg given intravenously 60% [421 patients]; placebo 40% [280 patients]). The maintenance study primary population included 568 guselkumab induction responders randomly assigned to receive guselkumab 200 mg given subcutaneously every 4 weeks (190 [33%] patients) or 100 mg every 8 weeks (188 [33%] patients) or placebo (guselkumab withdrawal 190 [33%] patients).”
Key findings:
INDUCTION DATA AT 12 WEEKS:
At induction week 12 At induction week 12Induction symptomatic endpoints -response noted in majority of guselkumab-treated patients by 4 weeks
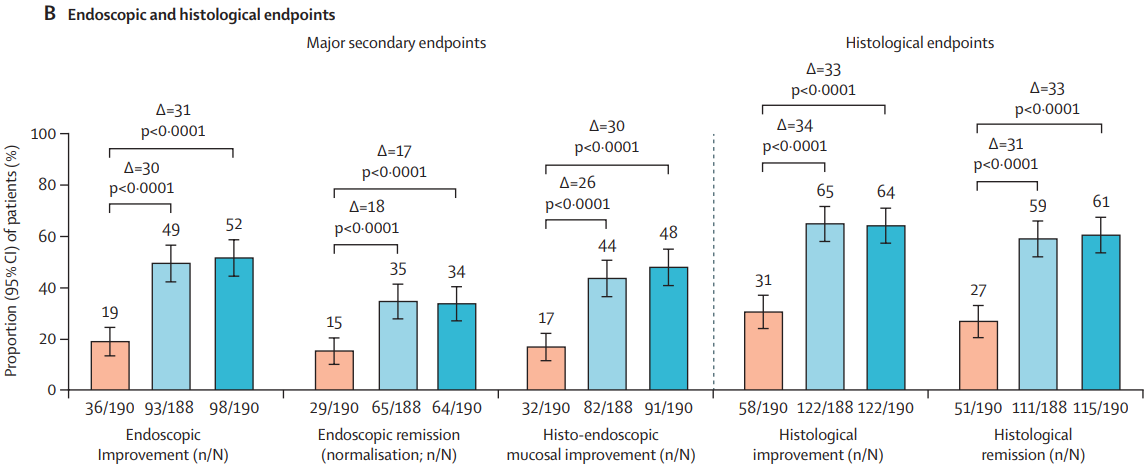
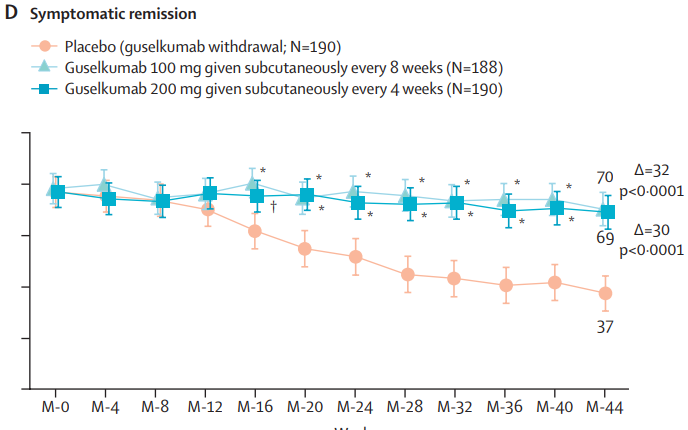
MAINTENANCE DATA AT 44 WEEKS
Results and Discussion points:
“Symptomatic improvement was observed as early as induction week 1 (first assessed timepoint)”
“Greater reductions in C-reactive protein and faecal calprotectin concentrations with guselkumab induction compared with placebo were observed as early as induction week 4 (first assessed timepoint)”
“Guselkumab efficacy was shown in both biologic naive and JAK inhibitor-naive patients, and in patients with a history of inadequate response or intolerance to biologics or JAK inhibitors”
“Overall, 34% (129 of 378) of patients in the guselkumab groups achieved endoscopic remission at maintenance week 44. Among the 180 patients in the guselkumab groups in clinical remission at maintenance week 44, 124 (69%) of 180 were in endoscopic remission”
“Symptomatic remission and deep symptomatic remission achieved with guselkumab induction was generally maintained to maintenance week 44 with guselkumab relative to placebo”
“The incidences of anti-guselkumab antibodies and NAbs were low in both the induction and maintenance studies…titres were low and did not affect serum concentration, efficacy, or safety”
“Head-to-head comparison data with other IL-23 antagonists are currently not available”
“Safety results were consistent with the known and favourable safety profile of guselkumab in its approved indications. Rates of adverse events, serious adverse events, and adverse events leading to treatment discontinuation generally did not occur more frequently in patients treated with guselkumab versus placebo-treated patients”
Limitation: The primary analysis population for themaintenance study included only guselkumab induction respondersfollowing 12 weeks of intravenous treatment
My take: Overall, this is a pivotal study showing that guselkumab is an effective agent for moderately to severely active ulcerative colitis in those with and without prior treatments. More head-to-head studies are needed to determine the optimal positioning of therapies for UC. Currently, AGA guidelines (AGA Living Guideline for Moderate-to-Severe Ulcerative Colitis –The Good and The Bad) suggest that guselkumab should be considered in the top tier of medications used in patients naive to biologics/advanced therapies and in the second tier for those with prior biologic treatments.
First of all: Bilberries are similar to blueberries, but have red inner flesh rather than white flesh.
Background: The authors note that some small studies have shown that anthocyanin-rich extract (ACRE), the bioactive ingredient of bilberries, has been effective for ulcerative colitis (UC)
“ACs have been associated with many protective biological effects, including anti-oxidative, anti-carcinogenic, antimicrobial, and anti-inflammatory properties [17,20,21]. Due to their phenolic structure, ACs exhibit an anti-oxidative capacity in vivo as they scavenge reactive oxygen species (ROS) [20,22], also a classical effect of 5-ASA [23]. After ingestion, ACs largely bypass absorption in the upper gastrointestinal tract, reaching the colon intact, where they are metabolized by microbiota through deglycosylation and further degraded into vanillic, protocatechuic, p-coumaric, gallic, and syringic acids (i.e., phenolic acids) [24]. ACs interrupt the pro-inflammatory signaling and are inhibitors of 5-lipoxygenase, a key enzyme implicated in the arachidonic acid pathway for the biosynthesis of active leukotrienes.”
Methods: A multi-center, randomized, placebo-controlled, double-blind study with a parallel group was conducted. Due to COVID-19’s effect on study enrollment, only 34 patients were randomized and only Eighteen ACRE and eight placebo patients could be analyzed (per protocol set)
Key finding:
Half (9/18) of ACRE patients and 3/8 of placebo patients responded clinically (p = 0.278). An improvement in the Mayo score was observed in the ACRE arm (77.8% vs. 62.5% placebo).
Fecal calprotectin (FC) dropped from 1049 ± 1139 to 557 ± 756 μg/g for ACRE but not for the placebo group (947 ± 1039 to 1040 ± 1179; p = 0.035).
The authors state that the placebo group had an unusually high response and that improved FC with ACRE patients indicates efficacy in UC.
Figure 2Figure 3
My take: This is a negative study (despite the secondary finding of improved FC at some timepoints). Importantly, the study did not demonstrate any harms in the ACRE group. It did help me understand more about bilberries!
Methods: The authors used a cross-sectional study using data from the National Health and Nutrition Examination Survey (2005-2010) and they used two 24-hour dietary recalls and, based on the Nova classification, calculated intakes of ultra-processed foods (UPFs) and minimally-processed foods (MPFs). N=12,716 adults.
Key Findings:
Median UPF and MPF intakes were 26.5% and 66.2% of total grams per day, respectively
Greater UPF consumption (in % gram/d) was associated with higher odds of constipation (adjusted OR [aORQ4 vs Q1], 2.20]
Discussion point: The authors did not find an association with diarrhea. “UPF consumption has been associated with increased risks of GI disorders that can cause chronic diarrhea including IBD and irritable bowel syndrome (IBS). This was thought to be related to alteration of the gut barrier integrity and activation of the immune response in the setting of microbial dysbiosis. The overall effect induces a pro-inflammatory micro-environment in the intestine and alterations in bowel function. However, the amount of UPFs needed to be consumed by individuals such that the risk of diarrhea would be higher is unknown and likely varies between individuals.”
My take: Limiting UPFs and promoting fresh foods/minimally-processed foods is better for our health.
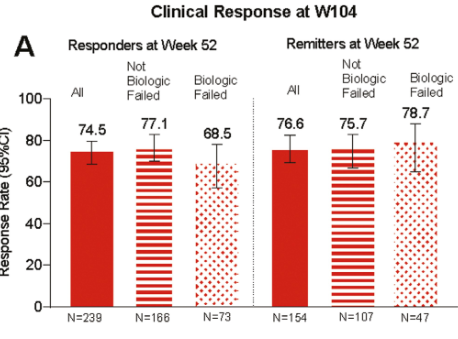
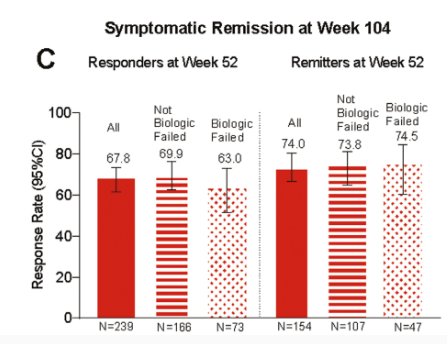
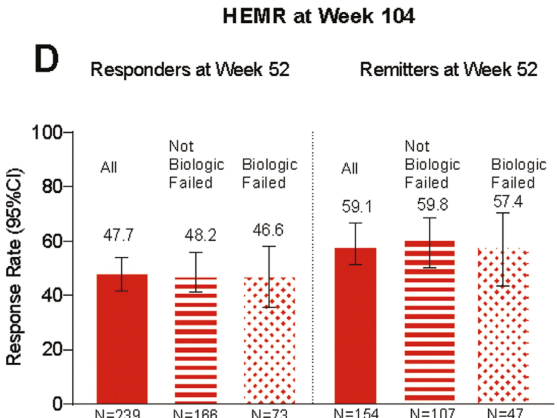
In this LUCENT-3 study, the authors examined response at 2 years among patientswho had response to treatment at 1 year; patients received 200 mg mirikizumab every 4 weeks. The authors stratified patients by induction response and by previous biologic exposure.
Key findings (from Figure 4):
HEMR= histologic-endoscopic mucosal remission
No new safety signals were identified, and the discontinuation rate due to adverse events was 2.8%
My take: It is good to see extended data for mirkizumab. Head-to-head trials, though, are needed to better determine which therapies are most effective.
Methods: VIVID-1 was a global phase 3, randomized, double-blind, double-dummy, placebo-controlled and active-controlled, treat-through study which enrolled 1150 patients with moderate-to-severe Crohn’s disease. There were three treatment groups: mirikizumab group, ustekinumab group, and placebo group. In each group, 48-49%were considered “biologic-failures” including 45-46% who were anti-TNF failures.
Key findings:
Discussion points:
Early treatment effect: “Symptomatic improvement was evident as early as week 4 accompanied by a statistically significant reduction in high-sensitivity CRP and faecal calprotectin, and endoscopic response was seen at week 12.”
Compared to ustekinumab: “Mirikizumab reached non-inferiority versus ustekinumab for clinical remission by CDAI at week 52…mirikizumab showed statistically significantly greater improvements from baseline in fecal calprotectin and CRP compared to ustekinumab. In addition, a greater percentage of patients reached the combination endpoint of endoscopic response and clinical remission by CDAI at week 52.”
Comparison across treatment trials: “. At week 52, 45∙4% of patients treated with mirikizumab met the endpoint of clinical remission by CDAI in the treat-through analysis with composite endpoint, 54∙1% met the endpoint in the treat-through analysis, and 64∙3% met the endpoint in the responder analysis. This example, with a range of nearly 20% percentage points depending on analysis type, shows the profound limitations in comparing unadjusted outcomes across phase 3 trials.” The authors note other differences in trial design between VIVID-1 and SEQUENCE (risankizimab) and state “no conclusions on relative efficacy can be drawn.”
My take: This study shows that mirikizumab is effective in adults with moderate-to-severe Crohn’s disease with and without prior biologic treatments. Pediatric studies are underway.
Background: The exposure–response relationship for the intravenous (IV) formulation of infliximab is well established, with multiple studies demonstrating that higher trough concentrations (C-trough) are associated with improved patient outcomes…However, the 2-week cycle of subcutaneous administration showed many-fold higher C-trough than the 8-week cycle of IV-IFX. Direct comparison of C-trough between SC- and IV-IFX is not appropriate because of different bioavailability and concentration–time profile. It is also not appropriate to apply the C-trough thresholds that predict achieving the therapeutic targets for IV.
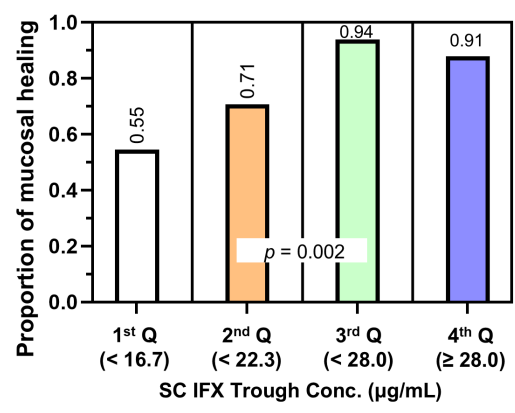
This was a cross-sectional retrospective study with 124 patients with Crohn’s disease (CD) who had received SC-IFX maintenance therapy for ≥6 months. SC-IFX C-trough was measured immediately before SC-IFX injection. Key findings:
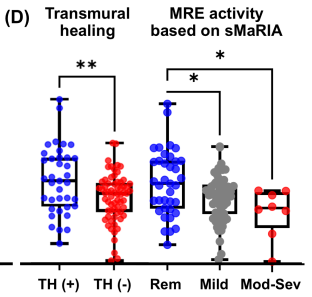
Mucosal healing (MH) was noted in 77.9% (74/95) and transmural healing (TH) in 36.3% (37/102).
SC-IFX C-trough was significantly higher in patients with MH (24.1 vs.16.9 μg/mL; p=0.001) and TH (26.0 vs. 20.5 μg/mL; p=0.007) than in those without.
Discussion:
Target trough levels: In this study, the authors found that “the C-trough thresholds for clinical remission, biochemical remission, MH and TH were 12, 16, 18 and 30 μg/mL, respectively, based on ROC analysis. The C-trough of SC-IFX increased with the depth of remission.”
Why trough level targets may differ between IV administration and SC: Administration via the IV route results in early and rapid peak concentration followed by a steady decline to trough, whereas administration via the SC route has slower absorption, lower bioavailability, lower peak concentration and smaller differences between peak and trough concentrations.
The authors note that a study by Ye et al (United European Gastroenterology Journal; 2020: 8: 385–386) with 55 patients found that a C-trough >26.6 mcg/mL achieved clinical remission and fecal calprotectin levels <250 mcg/g at week 54 in 79% and 91% respectively compared to 46% and 62% in those with with C-trough <16.4 mcg/g.
These C-trough levels are significantly higher that the median C-trough levels of standard dosing (120 mg biweekly) in a phase 1 dosing RCT which was only 13.3 mcg/mL (S Schreiber et al. Gastroenterology 2018; 154: 1371). The dosing of 180 mg and 240 mg biweekly resulted in C-trough levels of 19.9 mcg/mL and 26.5 mcg/mL respectively.
My take: This study suggests that therapeutic drug monitoring will have different targets with SC-IFX than with IV-SC. SC formulations will offer more convenience. However, more effort will be needed to make sure patients are adherent with therapy in order to achieve optimal outcomes.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.