Here’s a link to CDC website and COVID-19 symptom self-checker (advice for families):
CDC Link: Testing for COVID-19
———
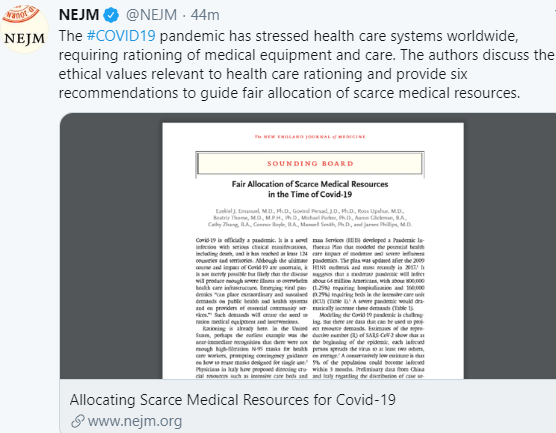
Full Link NEJM 2020 (Ezekial J Emmanuel et al): Fair Allocation of Scarce Medical Resources in the Time of Covid-19
This article spells out an ethical approach to the likely need to ration care in the midst of this pandemic.
Here’s an excerpt:
Recommendation 1: In the context of a pandemic, the value of maximizing benefits is most important…Saving more lives and more years of life is a consensus value across expert reports… Because young, severely ill patients will often comprise many of those who are sick but could recover with treatment, this operationalization also has the effect of giving priority to those who are worst off in the sense of being at risk of dying young and not having a full life….Because maximizing benefits is paramount in a pandemic, we believe that removing a patient from a ventilator or an ICU bed to provide it to others in need is also justifiable and that patients should be made aware of this possibility at admission..Undoubtedly, withdrawing ventilators or ICU support from patients who arrived earlier to save those with better prognosis will be extremely psychologically traumatic for clinicians — and some clinicians might refuse to do so. However, many guidelines agree that the decision to withdraw a scarce resource to save others is not an act of killing and does not require the patient’s consent
Recommendation 2: Critical Covid-19 interventions — testing, PPE, ICU beds, ventilators, therapeutics, and vaccines — should go first to front-line health care workers and others who care for ill patients and who keep critical infrastructure operating, particularly workers who face a high risk of infection and whose training makes them difficult to replace…Priority for critical workers must not be abused by prioritizing wealthy or famous persons or the politically powerful above first responders and medical staff — as has already happened for testing. Such abuses will undermine trust in the allocation framework.
Recommendation 3: For patients with similar prognoses, equality should be invoked and operationalized through random allocation, such as a lottery, rather than a first-come, first-served allocation process
Recommendation 4: Prioritization guidelines should differ by intervention and should respond to changing scientific evidence. For instance, younger patients should not be prioritized for Covid-19 vaccines
Recommendation 5: People who participate in research to prove the safety and effectiveness of vaccines and therapeutics should receive some priority for Covid-19 interventions
Recommendation 6: There should be no difference in allocating scarce resources between patients with Covid-19 and those with other medical conditions.
Placing such burdens on individual physicians could exact an acute and life-long emotional toll… To help clinicians navigate these challenges, institutions may employ triage officers, physicians in roles outside direct patient care, or committees of experienced physicians and ethicists,
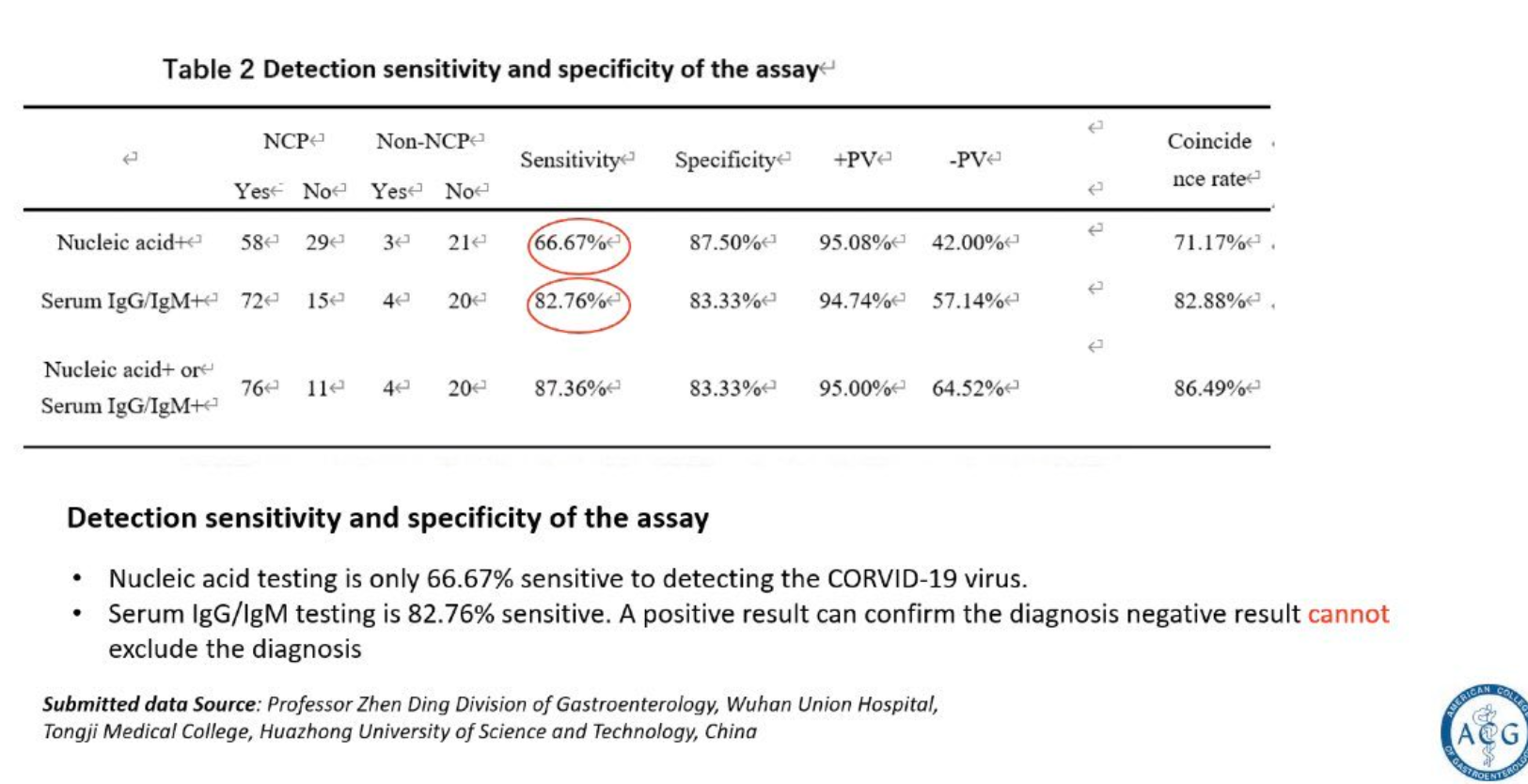
My take: Reading this article is so sad. It is heart-breaking just contemplating the need for these well-considered recommendations. Also, see below -ACG shared data indicating significant fallibility with testing for Sars-Cov2/COVID-19.