The August issue of Hepatology had several articles on Hepatitis C confirming the efficacy of newer agents:
- LI Backus et al Hepatology 2016; 64: 405-14. This “real-world” observational study from the VA Clinical registry with 4,365 genotype 1 treatment-naive patients who received ledipasvir/sofosbuvir showed SVR rates of 91.3% (w/o ribavirin) and 92% (w ribavirin).
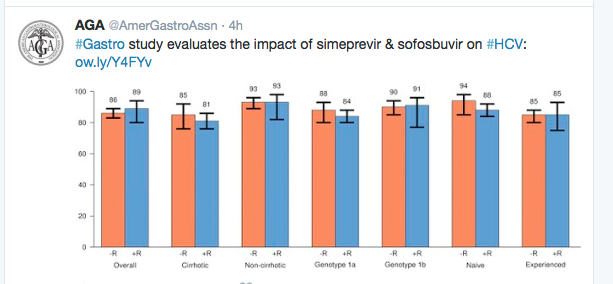
- P Kwo et al. Hepatology 2016; 64: 370-80 (OPTIMIST-1) This study showed that 12 weeks of simeprevir+sofusbuvir for 12 weeks was highly effective (97% SVR) and that 8 weeks of this therapy was inferior (83% SVR). N=310 with genotype 1 (w/o cirrhosis). No patients stopped therapy due to adverse effects.
- E Lawitz et al. Hepatology 2016; 64: 360-69 (OPTIMIST-2) This study showed that simeprevir+sofusbuvir for 12 weeks was effective in genotype 1 patients (n=103) with cirrhosis. For treatment-naive, the SVR was 88% and for treatment-experienced patients, the SVR was 79%.
Also in Hepatology:
- S Heibani et al Hepatology 2016; 64: 549-55. This study looked at 1-week versus 2-week intervals for endoscopic ligation. While 1-week ligation eradicated varices more quickly, neither approach was associated with differences in number of endoscopies, complications (including rebleeding) or other clinical outcomes.
From earlier study of “real-world” treatment of Genotype 1. Gastroenterol 2016; 150: 419-29. (Full text link)