Methods: In this single-center, observational study, the authors deployed an anonymized survey of outcomes that was completed by 107 parents of children with BA who were younger than age 12 years. A detailed assessment of general neurodevelopment (Mullens Scale of Early Learning and Vineland Adaptive Behavior Scale) was carried out in 50 infants younger than 5 years old, and emerging autistic traits (Autism Diagnostic Observation Schedule) were assessed in those eligible. There were 93 matched controls.
Key findings:
Neurodevelopmental concerns were raised by 37% of parents
47% of children required support from at least 1 service (such as speech and language therapy physiotherapy, play therapy, or seen a clinical psychologist), and a further 42% (n = 45) had used more than 1 service. The most accessed service was speech and language therapy (20%, n = 10)
A clinical or research diagnosis of autism was made in 30% of 35 children >2 years old
Early surgical intervention and faster clearance of jaundice after surgery was associated with better general neurodevelopmental outcomes (F = 2.428, P = .042) but not with the presence of emerging autistic traits
My take: High levels of neurodevelopmental difficulties occur in children with BA.
Recently Dr. Balistreri gave our group an excellent lecture. I have taken some notes and shared some slides. There may be inadvertent omissions and mistakes in my notes.
Key Points:
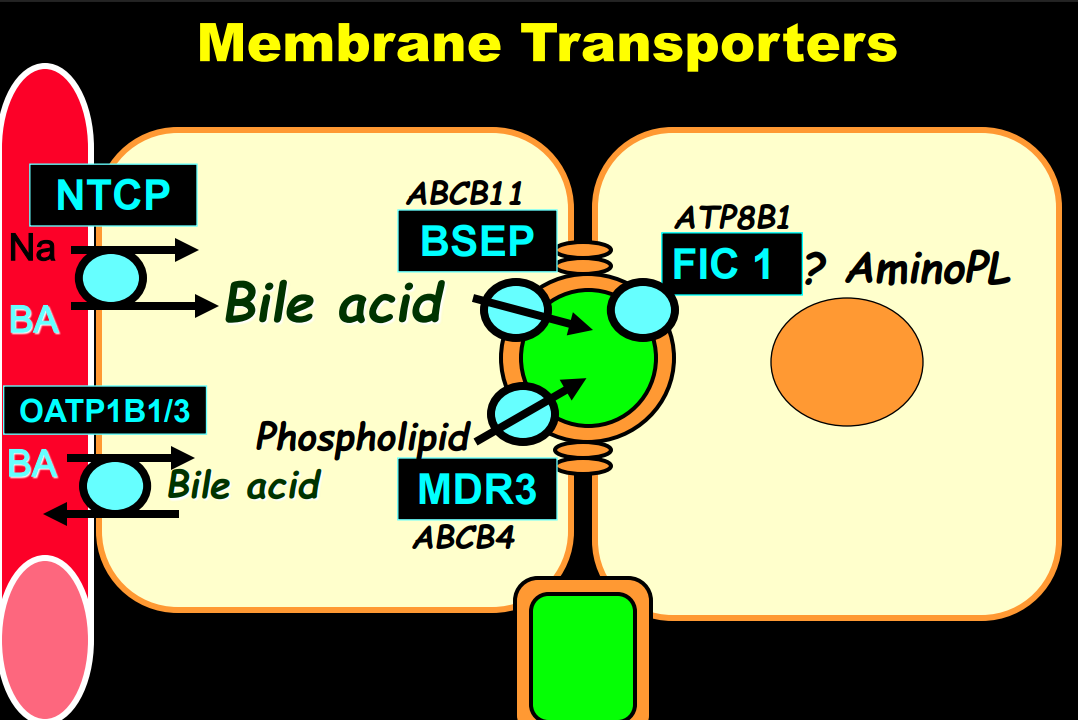
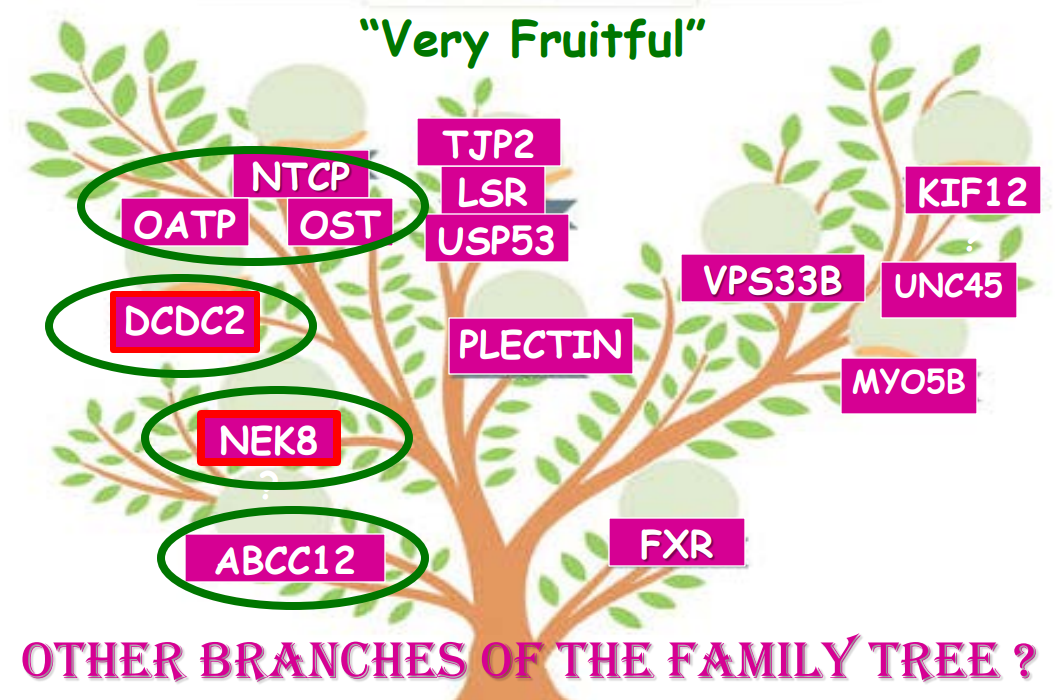
Producing enough bile acids and recycling bile acids in enterohepatic circulation is crucial for bile acid flow. In addition, there are ‘good’ bile acids like cholic acid that have trophic properties and ‘bad’ bile acids like lithocholic acid that cause liver toxicity
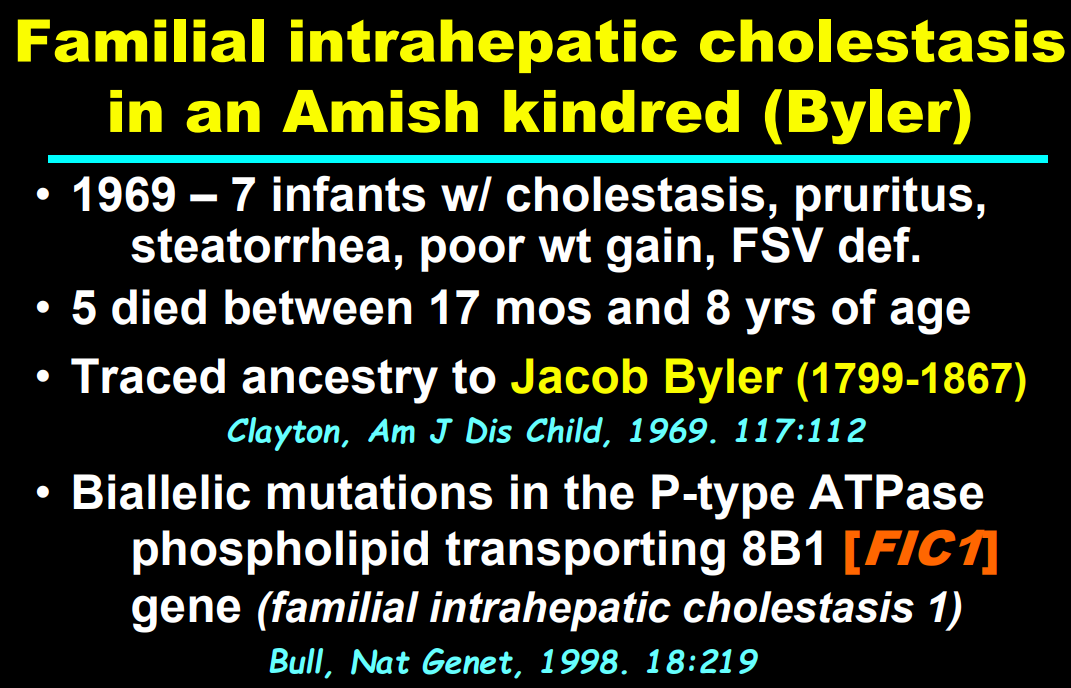
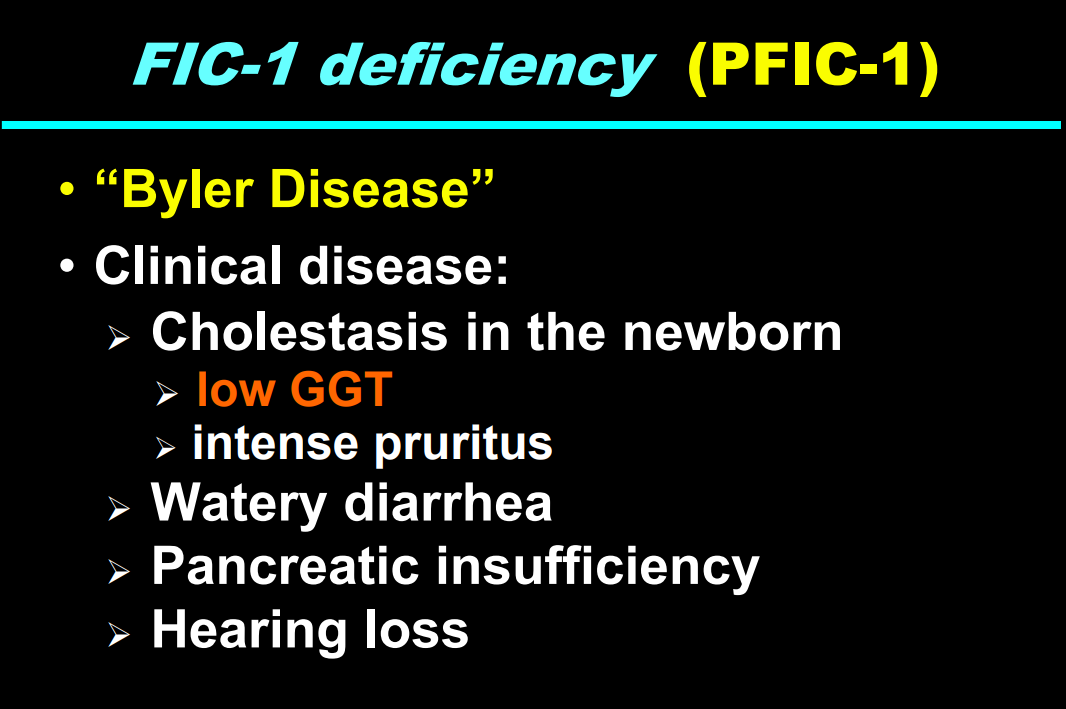
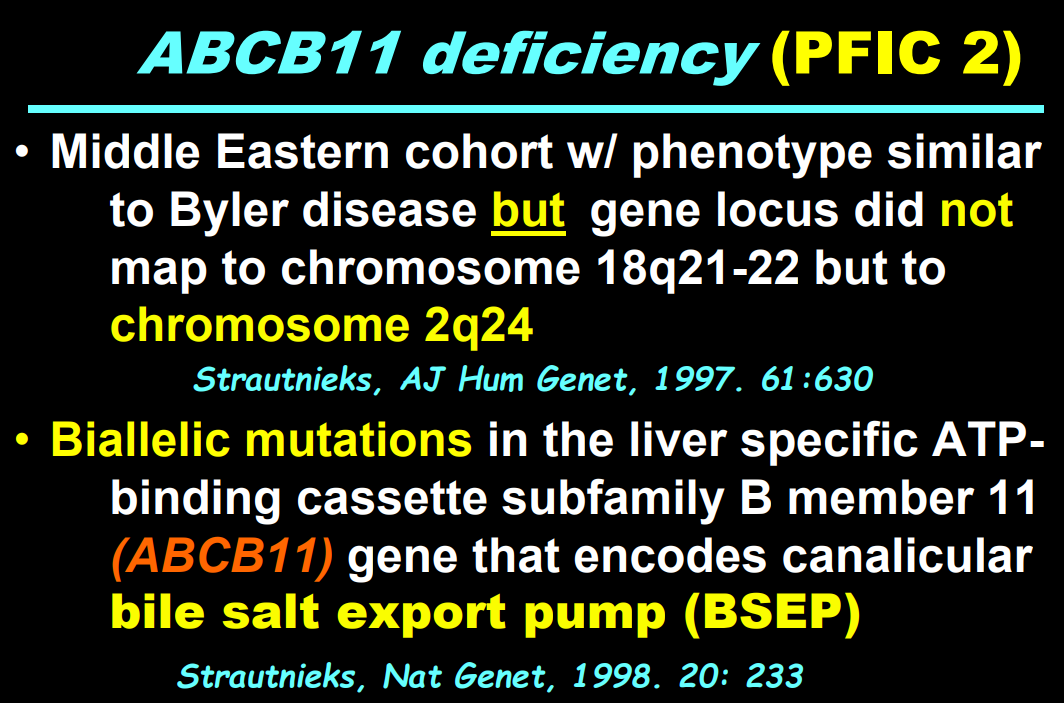
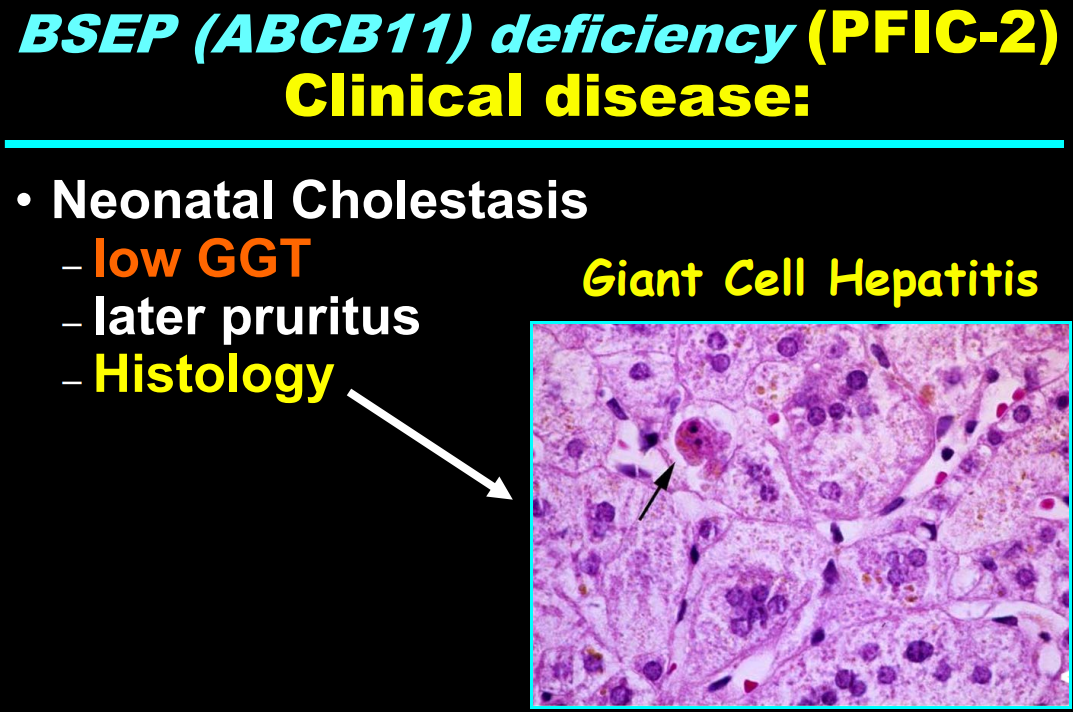
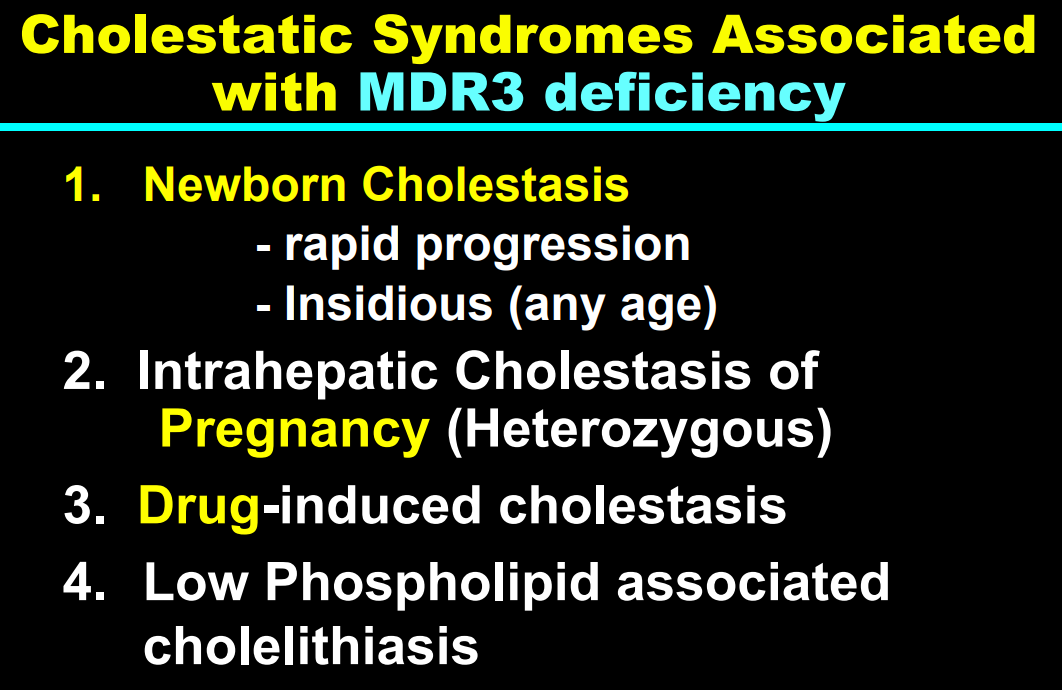
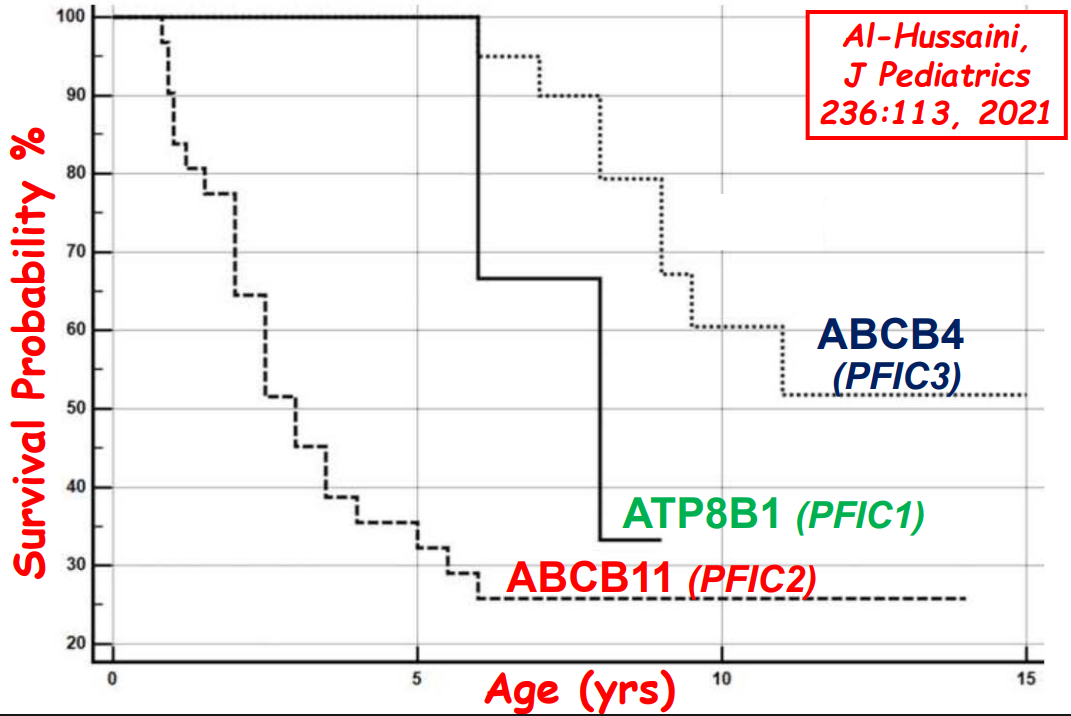
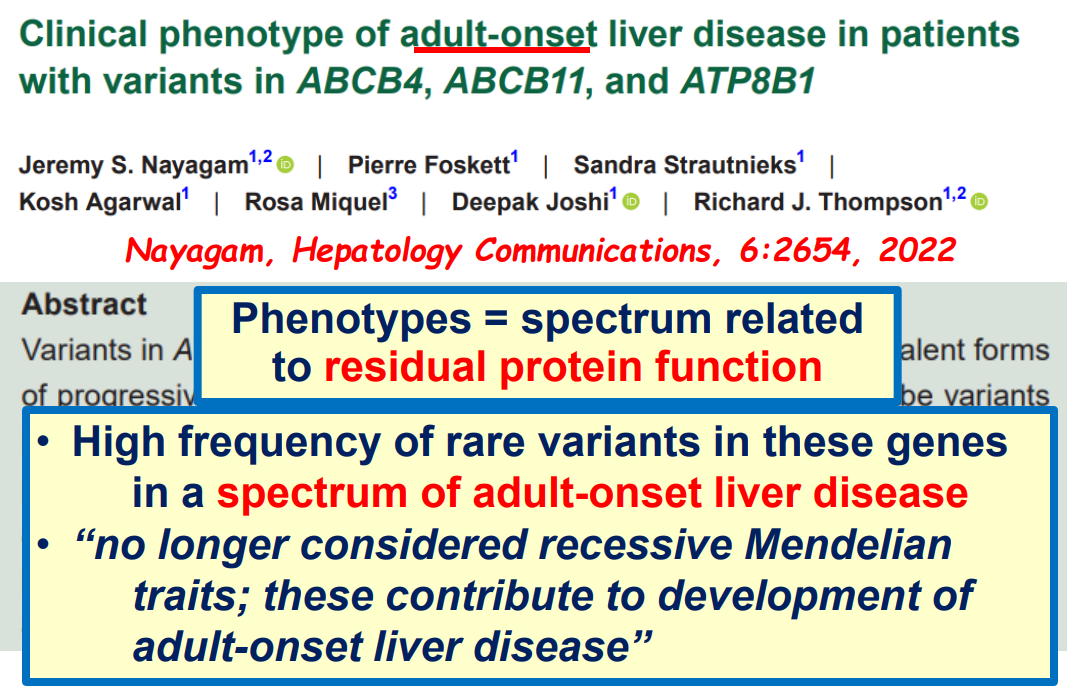
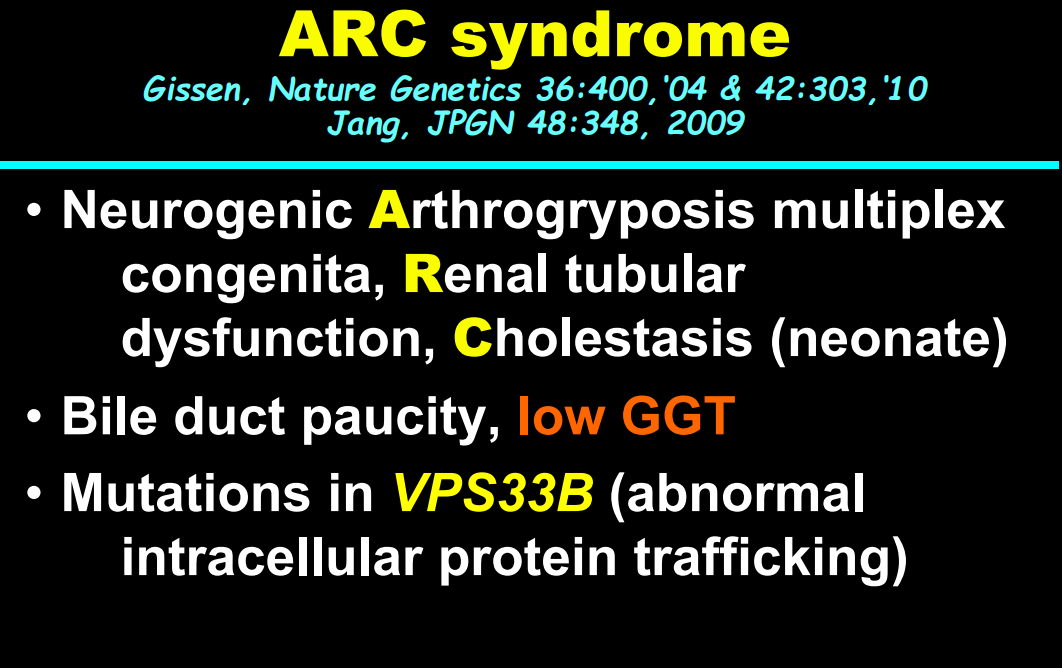
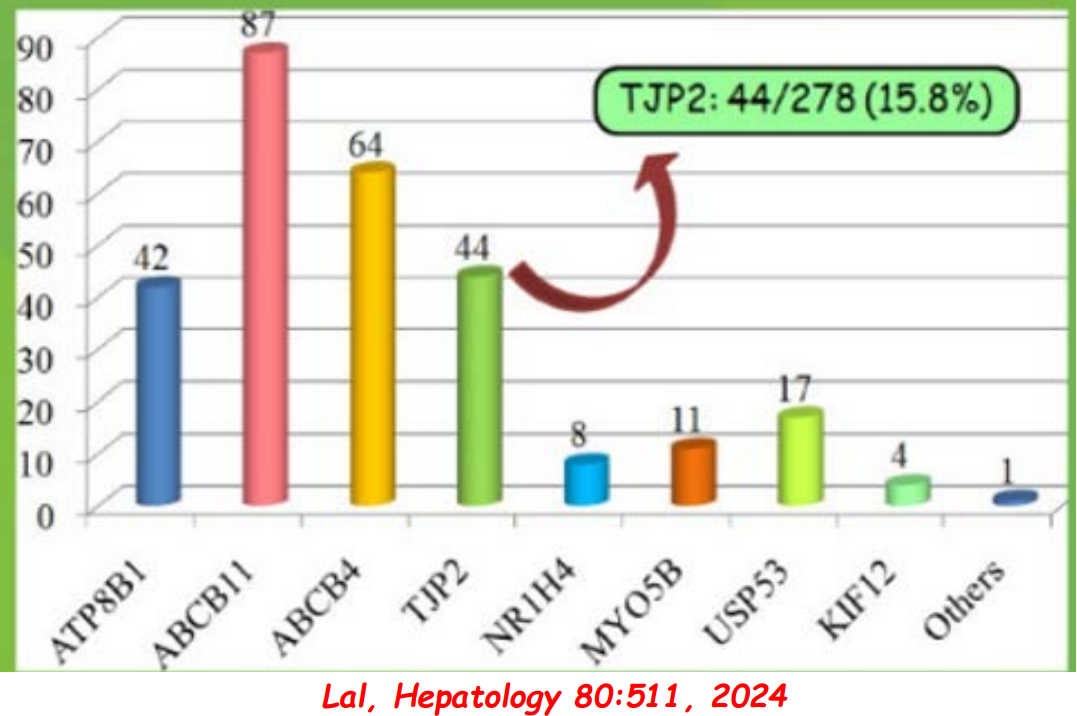
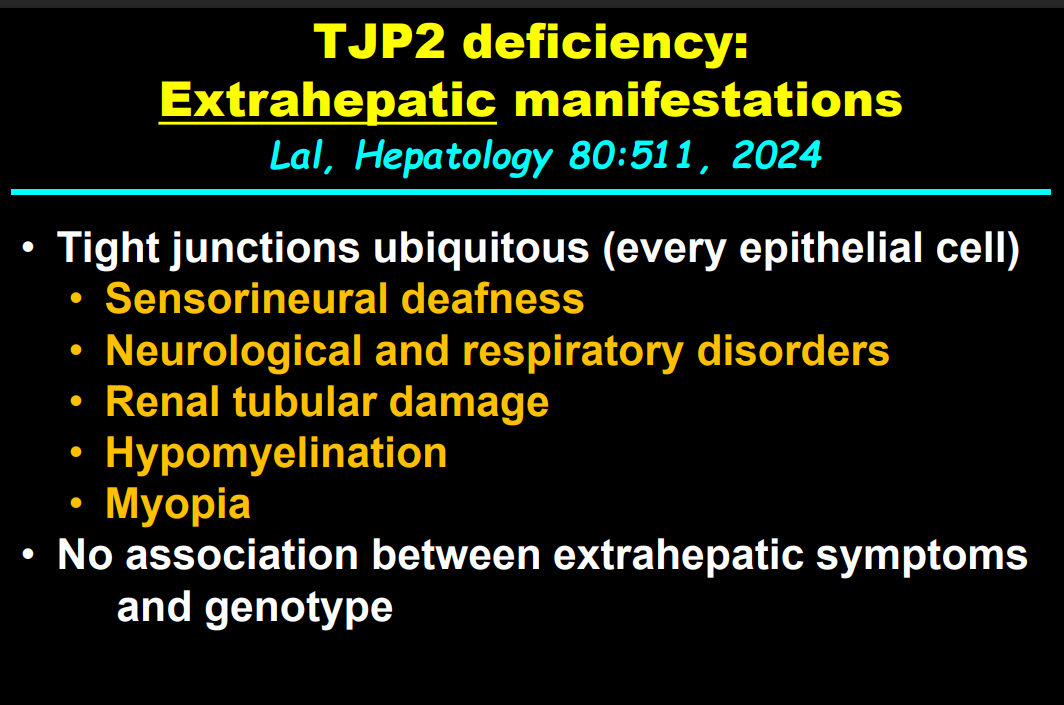
In addition to defects in the metabolic pathway of bile acids, discoveries identified defects in the membrane transporters (eg. FIC1, BSEP, MDR3), trafficking proteins (eg. MYO5B, VPS33B), nuclear control receptors (eg. FXR), and tight junction proteins (eg. TJP2). Tight junction protein defects are associated with bile leakage from bile canaliculus
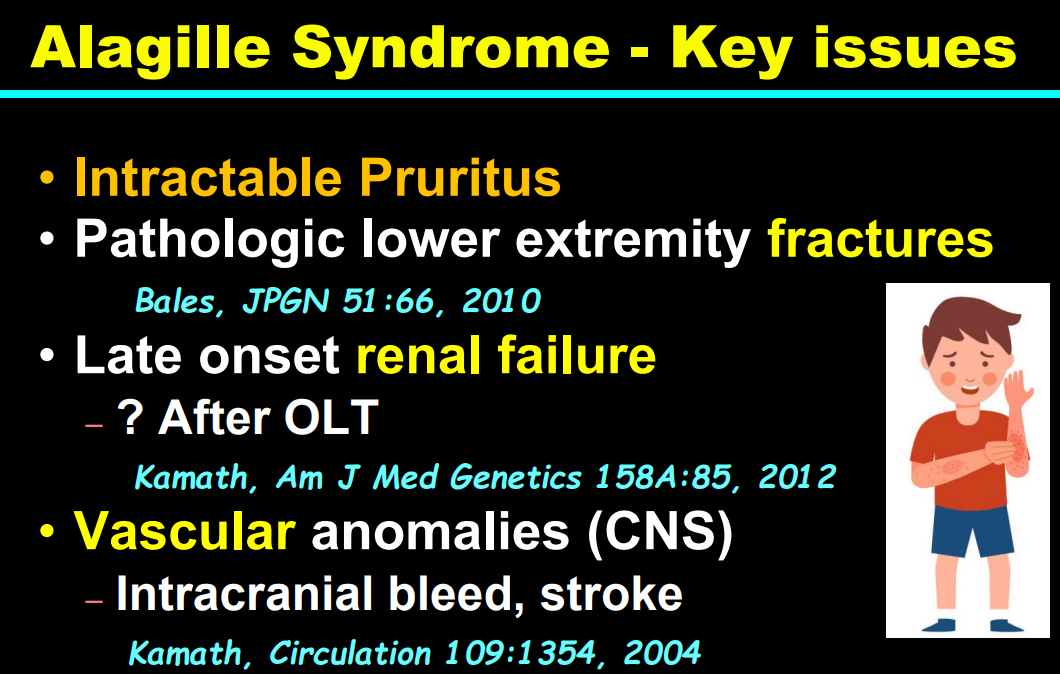
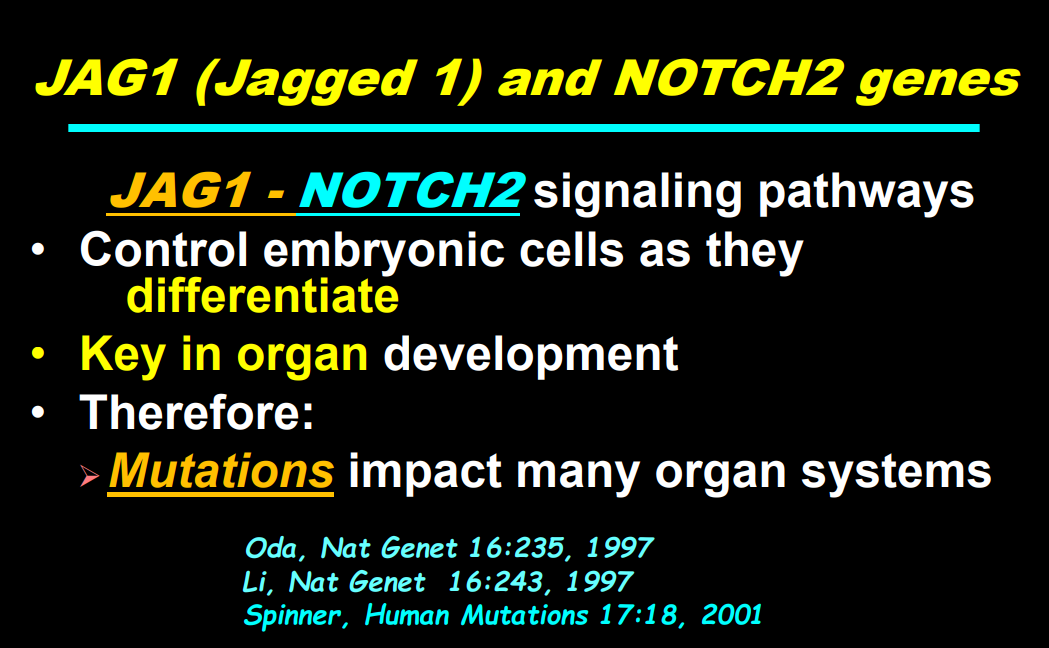
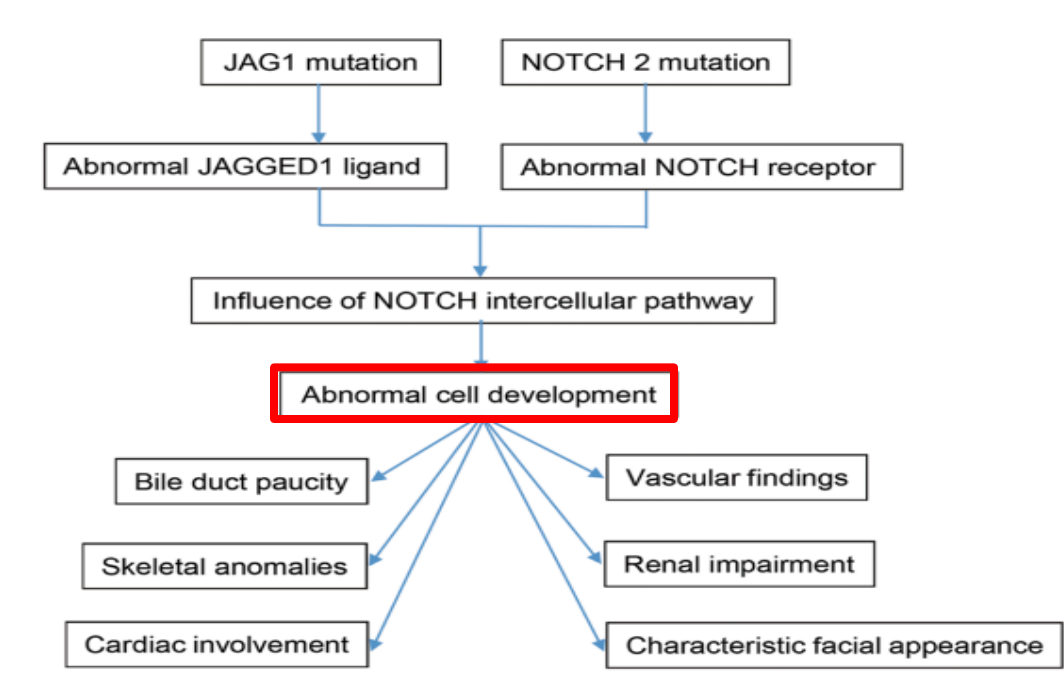
Alagille syndrome, a disorder of embryogenesis, related to JAG1-NOTCH2 signaling pathways affects organs throughout the body
Many of these genetic mutations are now being identified in adults with unexplained liver diseases (eg. intrahepatic cholestasis of pregnancy and cryptogenic cirrhosis)
Cholestasis panels and whole exome sequencing are important tools
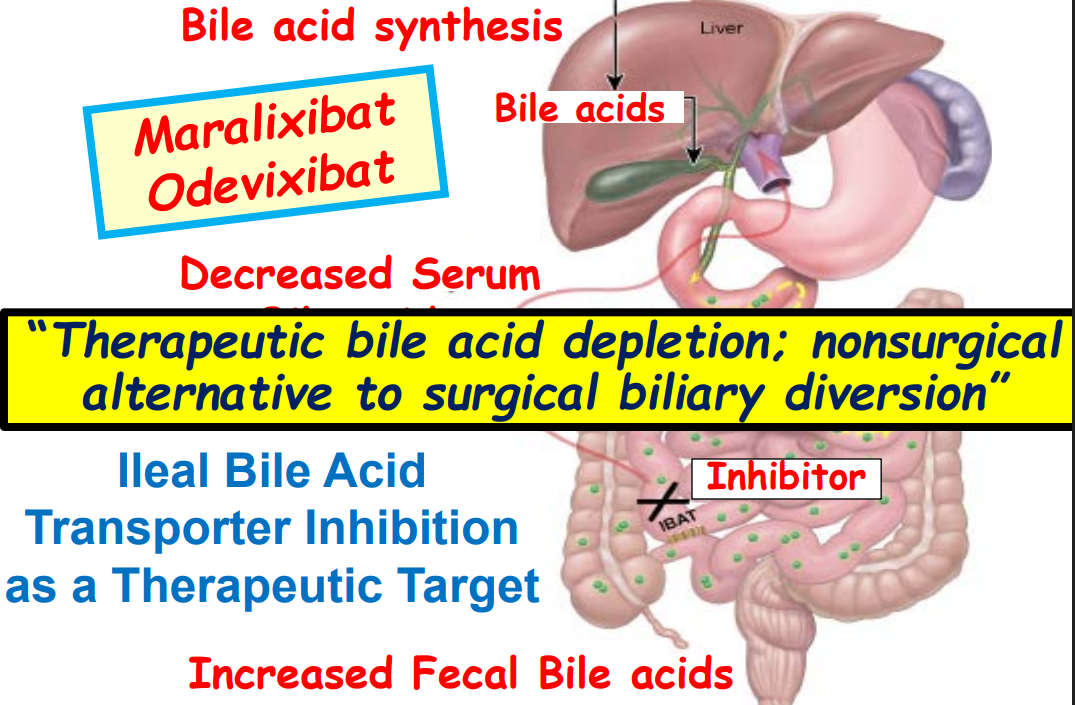
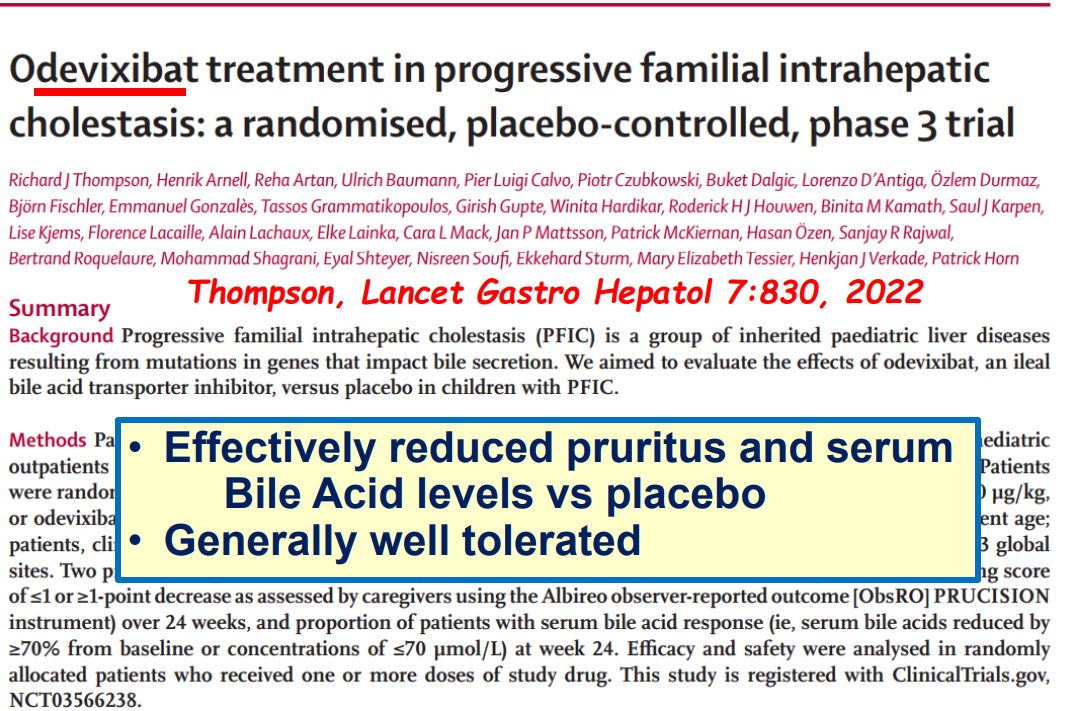
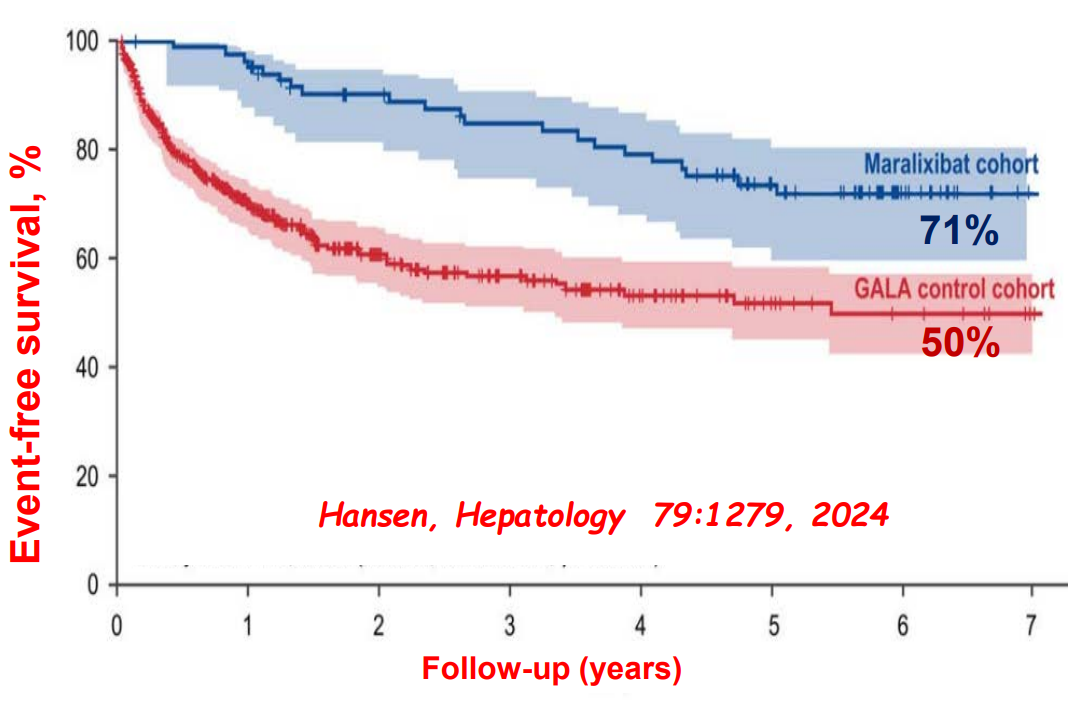
Ileal bile acid transporter (IBAT) inhibitors have emerged as important therapies for conditions like Alagille which were previously treated with biliary diversion
My take: This lecture really shows how the field of pediatric liver disease has been a puzzle. Now one can see how almost all of the pieces of the puzzle work together.
Background: “Measles is a highly contagious disease and, despite the availability of a safe and effective vaccine, remains still an important cause of childhood death worldwide [1,2]. The risk of severe illness in measles-naive individuals is particularly high in immunocompromised patients with inflammatory bowel disease (IBD) or after liver transplantation (LT) [3]…Ideally, vaccination with live attenuated vaccines (LAVVs) should be completed four weeks before organ transplantation or the initiation of immunosuppressive therapy (IST) to allow for the live vaccine’s incubation period and minimize the risk of vaccine-associated disease…LAVVs are considered contraindicated during IST due to safety concerns and limited experience.”
Methods: “In this prospective multicenter observational study (DRKS00014569) 22 children and adolescents with incomplete MMR vaccination status were identified… with stable immunosuppressive therapy in the last three months with no evidence of underlying disease activity…Sixteen patients were vaccinated against MMR, eleven after liver transplantation and five with inflammatory bowel disease. At the time of vaccination, four patients were receiving moderate (e.g., tacrolimus drug level below 5 ng/ml), eleven were receiving high-intensity immunosuppression (e.g. anti-tumor-necrosis factor agents, mycophenolate mofetil) and one child had previously discontinued immunosuppressive treatment.”
Immediately prior to the references, the authors provide a downloadable document detailing how they chose to categorize the degree of immunosuppression and their precise protocol, including immunologic pretesting and drug contraindications as noted below.
Key findings:
There were no serious adverse events or complications related to the vaccination
In children receiving immunosuppressive medications, the seroconversion rate for measles after the first MMR vaccination was 73.3 % (11/15) and after the second vaccination 80 % (12/15)
My take: In carefully-selected immunocompromised pediatric patients, the MMR vaccine may be safe. However, given the small numbers receiving vaccination in this study, the absolute safety is unclear. Even infrequent adverse effects would be problematic. This study’s protocol could be helpful for those considering vaccination in immunocompromised populations with a measles epidemic. For now, the most important approach is improving vaccination rates in those (especially family members) without contraindications.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: “Current guidelines recommend treating all children aged 3 years or older with DAAs (direct-acting antivirals). These treatments achieve cure in more than 98% of HCV cases and reduce risks for cirrhosis, hepatocellular carcinoma (HCC), and liver-related mortality. Despite availability of DAAs, only 62% of adults with HCV have linked to care, 39% initiated treatment, and 26% attained cure (sustained virologic response) as of 2023.”
Methods: This retrospective cohort analysis included children born between 2000 and 2018 who were diagnosed with HCV between the ages of 0 and 18 years. The study analyzed TriNetX Research Network data, a US national electronic health records network with more than 87 million individuals within the U.S.
Key findings:
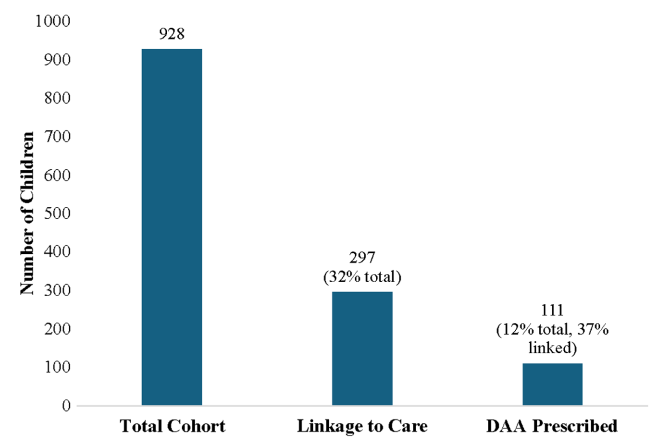
Among 928 children with HCV, 297 (32.0%) linked to HCV care and 111 (12.0%) were prescribed a DAA (direct-acting antiviral). Thus only 1 in 8 children with HCV were prescribed DAAs
Of 928 children with HCV, 35.9% of children were diagnosed with HCV perinatally (by 3 years old), 44.5% during childhood (between 4 and 12 years old), and 19.6% in adolescence (between 13 and 18 years old)
White and Hispanic/Latinx children were much more likely than black children to receive a DAA prescription with OR of 3.44 and 2.20 respectively
Children in Midwest, North, and West had higher rights of DAA prescription compared to the South with OR of 2.40, 1.50, and 4.19 respectively
Discussion points:
Potential barriers to treatment:
DAAs were only approved for children aged 3 years or older in 2019 for some genotypes and not until 2021 for all genotypes.
Some parents choose to wait to treat young children because of difficulty administering medications at the ages of 3 and 4 years old
Insurance: “The cause of low uptake of treatment is likely multifactorial: Medicaid and commercial insurers implemented restrictions based on degree of liver fibrosis, active or recent substance use, or specialty prescribing because of the very high initial cost of DAAs. Although most of these restrictions have now been removed, some still remain, and some insurance plans have varying criteria for pregnant or pediatric members.”
New CDC Recommendations: “In light of the new Centers for Disease Control and Prevention perinatal HCV testing recommendations and universal HCV screening recommended in pregnancy, more young children with HCV will be identified”
Limitations: Retrospective study relies on data from a database
My take: Being able to cure HCV with DAAs has been an incredible medical achievement. However, efforts to eradicate HCV have not gotten very far and had a severe setback with the opioid epidemic which increased rates of HCV. This study shows that very few children with HCV actually receive curative treatment. Advancing the goal of HCV elimination will require sustained efforts to get those identified with HCV to treatment, both in children and adults.
“The prevalence of HCV in pregnant people jumped 16-fold between 1998 and 2018 to 5.3 cases per every 1000 pregnancies, and these patients can transmit the disease perinatally. Many people are unaware they are infected.”
“More than half of children clear the infection on their own by age 3, the age at which treatment can also begin”
Background: “Hemangiomas remain the most common tumor of the liver in newborns and infants…A subtype classification system for hepatic hemangioma (HH) was first proposed based on our Liver Hemangioma Registry in 2007, delineating focal, multifocal, and diffuse HH…Focal hepatic lesions correspond to congenital hemangiomas whereas multifocal and diffuse lesions represent infantile hemangiomas.”
Methods: This was a retrospective review of 96 infants over an 18 year period (2004-2022). Patients with infantile HH were excluded.
Key Findings:
32% were diagnosed prenatally, 23% developed heart failure, and 23% developed respiratory failure
There was a balanced sex distribution (50% for each gender)
Common clinical features included transient anemia (n = 23/48, 48%) and thrombocytopenia (n = 30/53, 57%).
On average, patients demonstrated 43% residual HH volume at 12 months and 16% residual volume at 24 months
No difference in time to 50% HH volume reduction between patients with and without medical therapy was observed
Larger hemangioma volumes were associated with an increased risk of anemia (P = .005) and thrombocytopenia (P < .001)
There was not a significant association between HH volume and congestive heart failure (CHF) or cardiomegaly. For example, the HH volume was 824 mL vs 579 mL (P=0.689) in those with and without CHF, respectively
Discussion Points:
“Congenital HH is present at birth and typically does not undergo postnatal growth”
“Congenital HH occurs equally in males and females and is immunonegative for GLUT-1. This stands in contrast to infantile hepatic and cutaneous hemangioma, which exhibits an early proliferative phase followed by gradual involution”
“HH size at diagnosis was associated with respiratory failure but not with the development of cardiomegaly or CHF, suggesting intralesional shunting may not be related to absolute tumor volume. Hence, all HH regardless of size should be assessed for shunting by doppler US”
“We advocate consideration of cross-sectional imaging and/or biopsy if patients with presumed congenital HH do not follow the expected clinical behavior of early signs of involution”
“Although corticosteroids and propranolol have proven benefit for infantile HH, we demonstrate that there was no significant difference in the rate of congenital HH involution between patients who had received medical therapy and those that did not”
“Medical therapy does have a role in the medical management of high-output heart failure occurring secondary to shunting. If refractory to pharmacologic therapy, these patients should undergo embolization of symptomatic intrahepatic shunts”
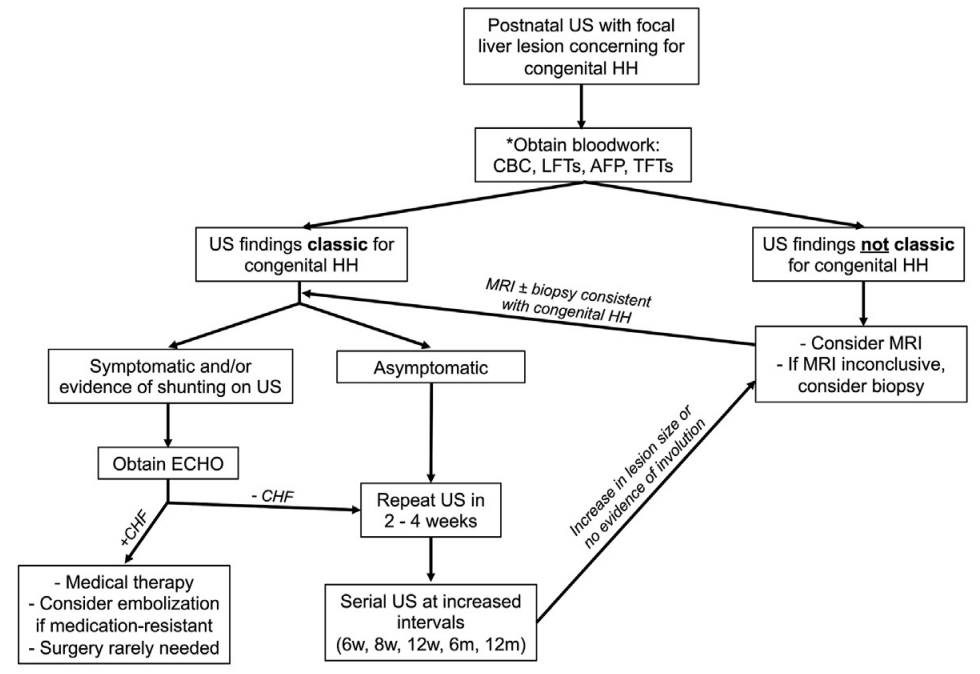
The practice algorithm for evaluation and management of congenital HH suggested by the authors. *Obtain baseline labs and repeat as needed. Repeat CBC if lesion increases in size during monitoring period and there is concern for intralesional bleeding. Repeat AFP as necessary to rule out hepatoblastoma. TFTs indicated if unclear whether congenital HH or infantile HH .
My take: This is a very useful study. It is important to distinguish congenital HH from infantile HH. Even in those with congenital HH, “a subset of patients develop life-threatening complications including respiratory failure and CHF that warrant directed medical management.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.