CC Reed et al. Clin Gastroenterol Hepatol 2025; 23: 946-953. Open Access! Daily or Twice Daily Treatment With Topical Steroids Results in Similar Responses in Eosinophilic Esophagitis
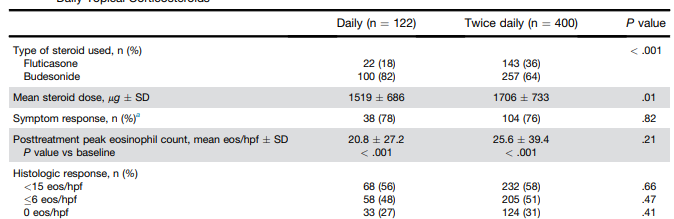
Methods: This was a retrospective cohort study using the UNC EoE Clinicopathologic Database of newly diagnosed patients with EoE treated with a tCS who had a follow-up endoscopy with biopsy. In total, there were 522 patients, including 195 pediatric patients (<18 yr). 122 patients received once daily dosing and 400 patients received twice daily dosing.
At our center, patients are typically treated on a clinical basis with either oral viscous budesonide or fluticasone from a multidose inhaler, with daily doses ranging from 1–2 mg for budesonide and 440–1760 μg for fluticasone based on patient size and at the discretion of the provider.
Key findings:
- Global symptomatic response (78% vs 76%; P = .82), posttreatment eosinophil count (20.8 vs 25.6; P = .21), posttreatment EoE Endoscopic Reference Score (2.2 vs 2.2; P = .92), and histologic response (<15 eos/hpf; 56% vs 58%; P = .66) did not differ by dosing frequency
- Candida was less frequent with daily dosing (2% vs 8%; P = .04)
My take: This study suggests that once daily dosing can be as effective as twice daily dosing. It may be that the total dose administered may be more important than the frequency. More studies are needed to confirm these results.
Related blog posts:
- Impact of Disease Severity on Eosinophilic Esophagitis Treatment Responses
- Delivery Vehicle and Outcomes for Budesonide-Treated Eosinophilic Esophagitis
- I-SEE for Eosinophilic Esophagitis (has pictures and table to calculate I-SEE score)
- I-SEE (Index of Severity for Eosinophilic Esophagitis) Works in Kids TooPractical Tips for Eosinophilic Esophagitis
- AGA: High Quality Upper Endoscopy
- “Esophageal Hypervigilance” and Outcomes in Eosinophilic Esophagitis
- “Real-World” Dupilumab for Eosinophilic Esophagitis
- Budesonide FDA-Approved for Eosinophilic Esophagitis
- “Tug” Sign For Eosinophilic Esophagitis and EoE Bowel Sounds Tips
- Budesonide for Maintaining EoE Remission
- Head-to-Head: Budesonide vs Fluticasone for Eosinophilic Esophagitis
- Budesonide Looks Better for Eosinophilic Esophagitis