Yesterday, the AAP put out a statement (see below) regarding the numerous lawsuits related to necrotizing enterocolitis. The lawsuits allege that formula companies did not provide physicians and patients warning that their products could increase the risk of necrotizing enterocolitis relative to breast milk or donated human milk.
Currently, when one searches for “NEC and lawsuits,” it is difficult to find these news reports due to dozens of law firm websites trying to attract clients. Per CNBC article, “close to 1,000 lawsuits have been filed against Abbott, Enfamil formula maker Reckitt Benckiser or both in federal or state courts.”
My take: These lawsuits are likely to exponentially increase the cost of formulas for all infants with little justification. It has been well-recognized for decades that there are many factors contributing to NEC; infants receiving human milk also develop NEC. For many infants in the NICU, sometimes there is no availability of human milk. What is going to happen to them if formula companies stop making premature formulas?
The most promising therapeutic to try to reduce the risk of NEC would be a safe probiotic. However, the FDA closed off this avenue (see: End of the Line for Probiotics for Preterm Infants). Even if the FDA reversed its position, no company would be willing to try to develop these products due to fear of litigation.
Background/Methods: A constitutional disease‐causing variant (DCV) in the SMAD4 or BMPR1A genes is present in 40%–60% of patients with juvenile polyposis syndrome (JPS). A total of 124 children with JPS were included: 69 (56%) DCV‐negative and 55 (44%) DCV‐positive (53% SMAD4 and 47% BMPR1A) with a median (interquartile range) follow‐up of 4 (2.8–6.4) years
Key findings:
DCV‐positive children were diagnosed at an older age compared to DCV‐negative children [median 12 years vs. 5 years, respectively, p < 0.001], had a higher frequency of family history of polyposis syndromes (50.9% vs. 1.4%, p < 0.001), experienced a greater frequency of extraintestinal manifestations (27.3% vs. 5.8%, p < 0.001), and underwent more gastrointestinal surgeries (16.4% vs. 1.4%, p = 0.002). All operations in the DCV‐positive group were performed in patients with SMAD4 mutations
DCV-positive children had more frequent new polyps: average of 12.2 versus 2 new polyps for every year of follow‐up
DCV-positive children had a lower frequency of rectal bleeding (56% compared to 93%) which could be a factor in later presentation
There was no difference in the burden of polyps between patients with SMAD4 and BMPR1A mutations. A higher frequency of gastric polyps was observed in the SMAD4 group (55.3%vs. 9.1% for the patients in the BMPR1A group ,p = 0.004). . HHT was observed only in the SMAD4 mutations group (20.7% vs. 0 in the BMPR1Agroup. p = 0.024)
My take: Children with DCV-positive JPS likely require more frequent surveillance than DCV-negative JPS.
ESPGHAN Juvenile Polyposis Syndrome Recommendations These recommendations are different in that they do not recommend EGD in the pediatric age group: “Surveillance of the upper GI tract in affected or at-risk JPS patients is not required in childhood or teenage years, unless there is unexplained anaemia or upper GI symptoms.”
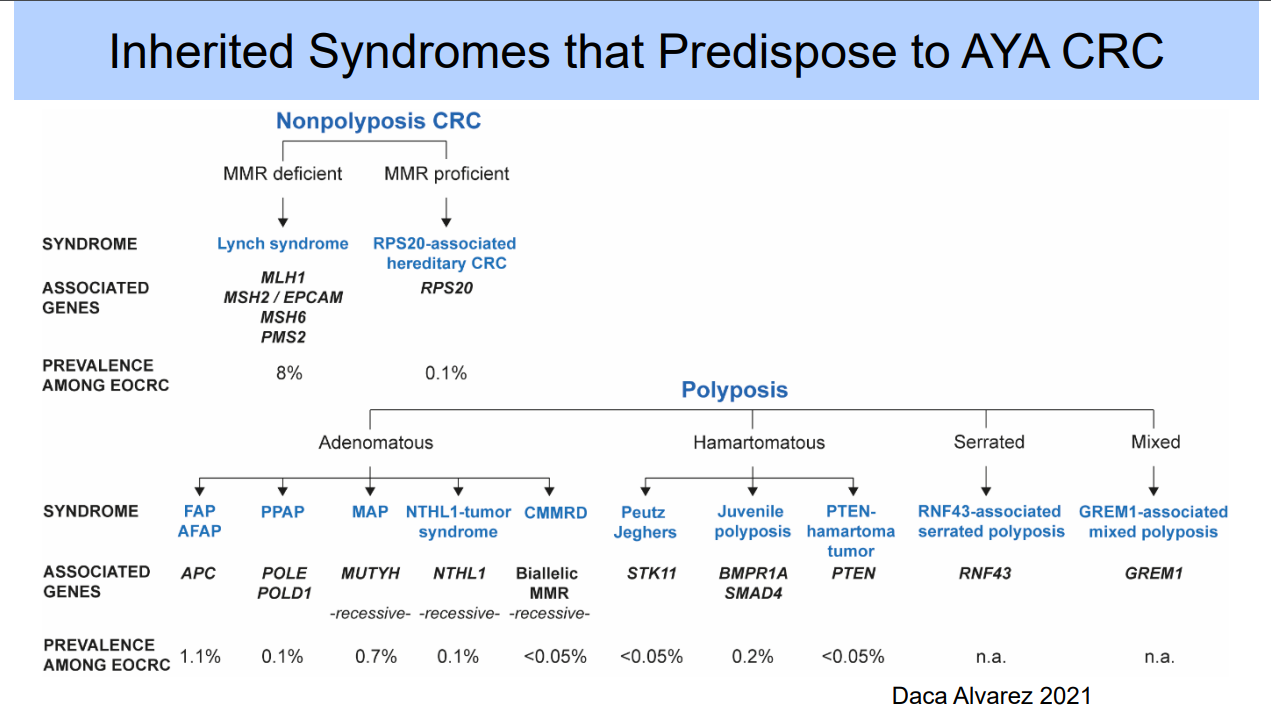
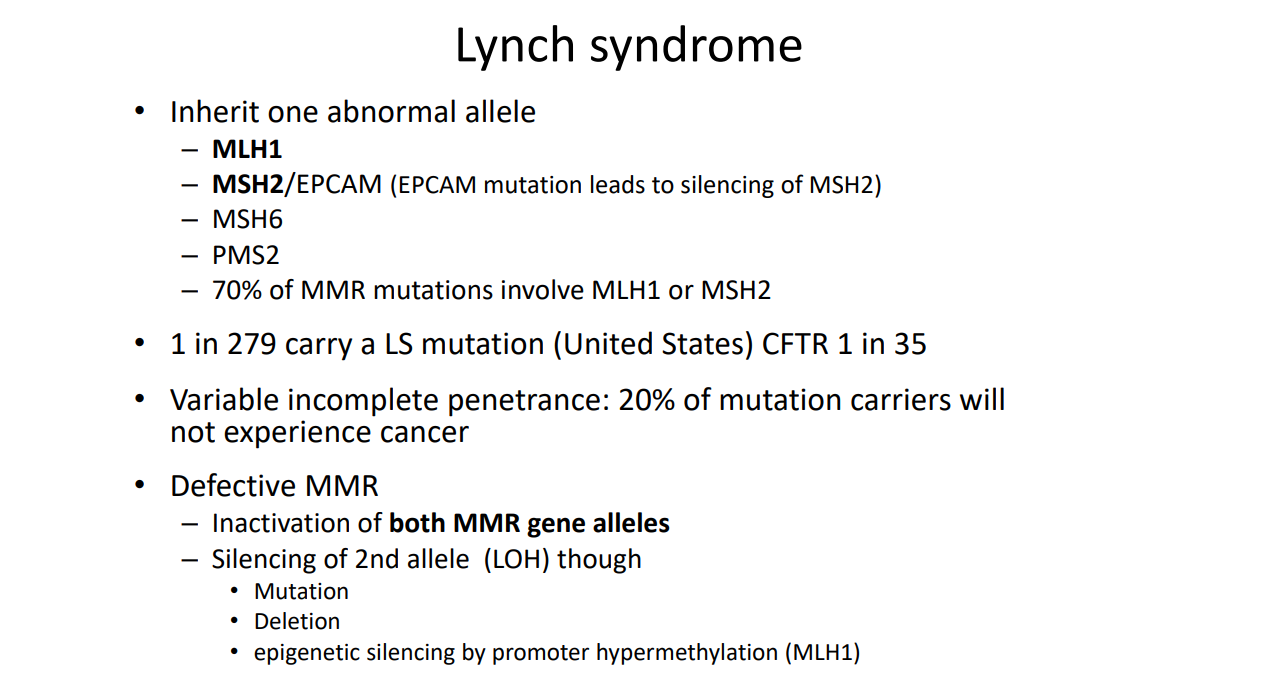
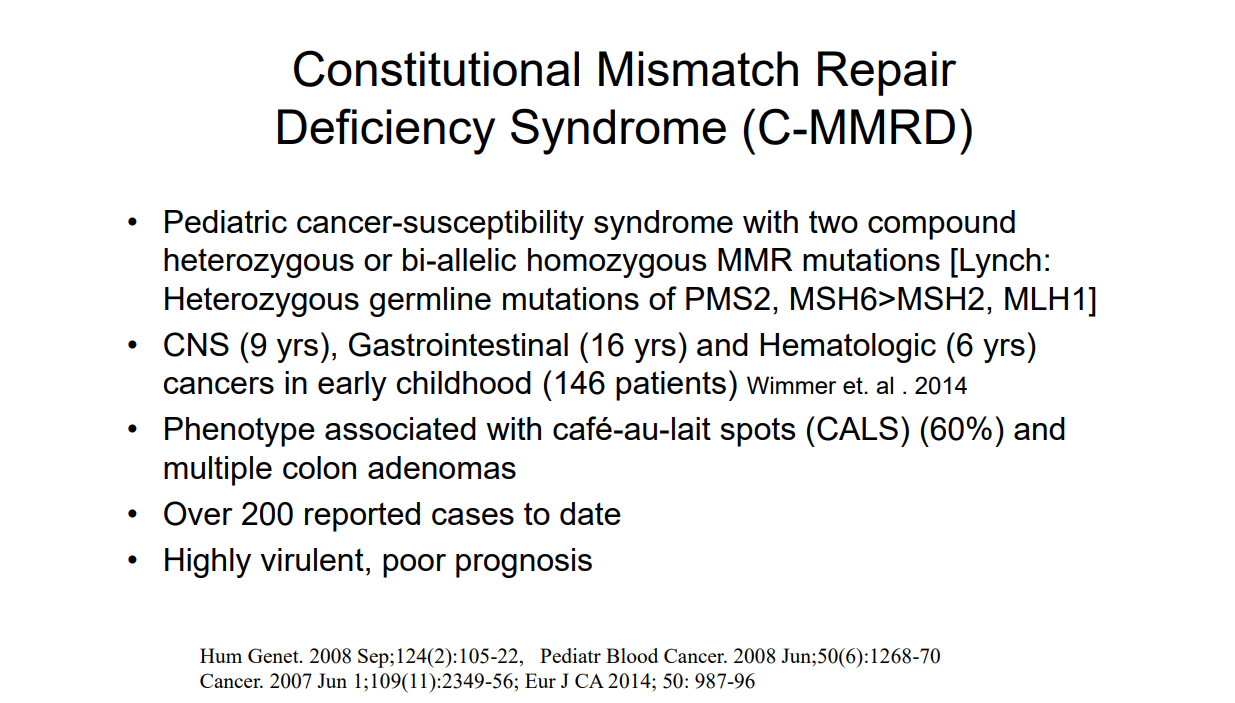
Are You Familiar with CMMR-D? The term CMMR-D refers to constitutional mismatch repair deficiency. This occurs when an individual inherits two MMR gene defects (rather than one gene defect in Lynch syndrome); with CMMR-D screening recommendations include yearly endoscopic evaluation beginning at age 3 years or at diagnosis.
Recently, Dr. Steve Erdman gave our group a great update on polyposis disorders. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
Key points:
There has been breath-taking progress in understanding of polyposis disorders. It is important to have genetic counselors participate to optimize testing and evaluation
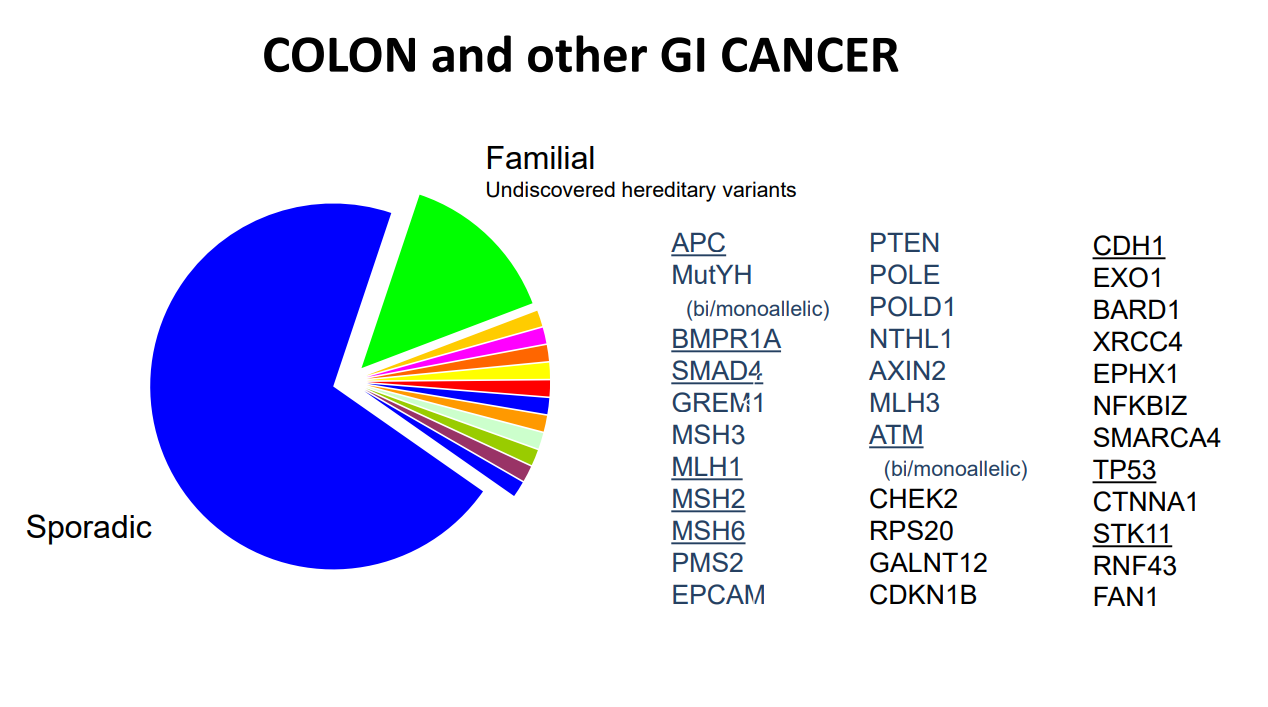
In patients with suspected polyposis syndromes, a genetic diagnosis is very important and can help guide management
Family history is very important. If several family members have had GI or other cancers at a young age, more aggressive interventions are usually indicated. However, individual family members can have a wide variation in presentation
In patients with many polyps, it is worthwhile to alert family to the fact that some polyps can be missed on colonoscopy and to contact medical team if there are recurrent symptoms like rectal bleeding
Some disorders, like juvenile polyposis syndrome (JPS), the connection between polyp presence and cancer risk is not clear. The increased risk for colon cancer my remain after polypectomy.
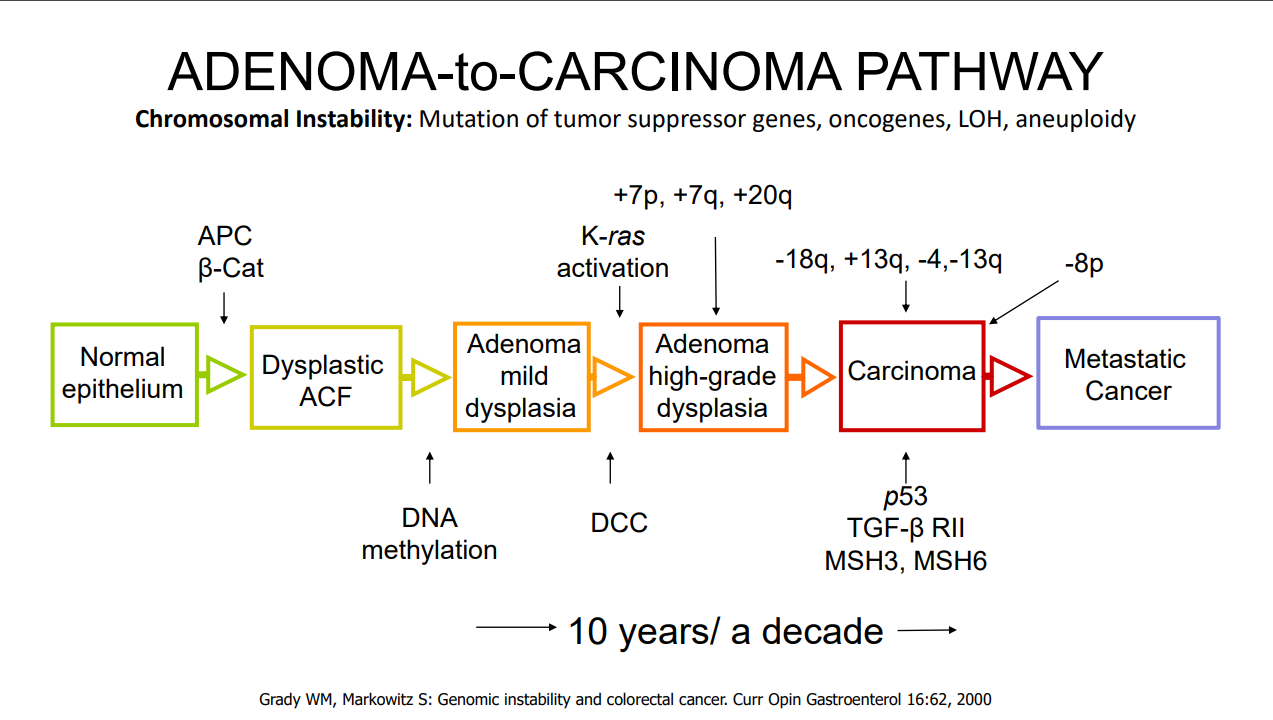
For most individuals with adenomatous polyps, removal of the polyps prevents cancer development (in the GI tract) as there is a well-described adenoma-to-cancer sequence that typically takes 7-10 years to progress from adenoma to colon cancer
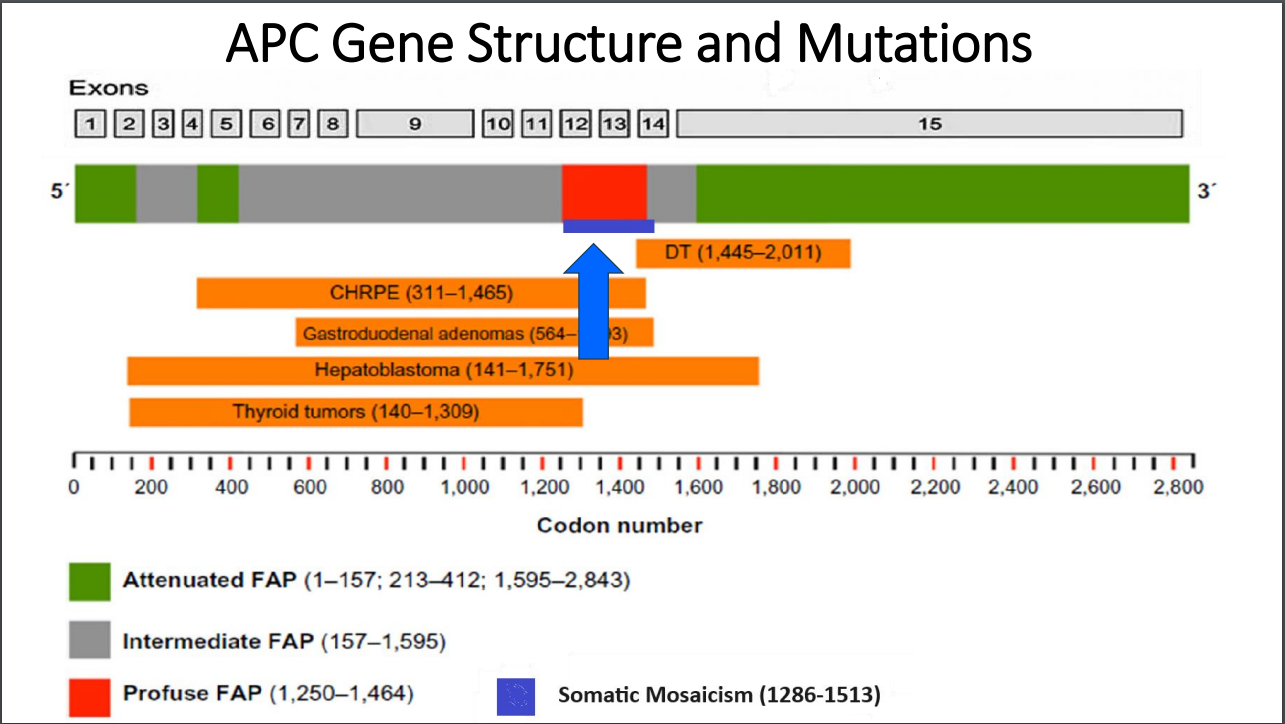
With FAP, the severity is related in part to the specific mutation. Mutations in the mutation cluster region are associated with an aggressive phenotype and mutations causing attenuated FAP are less aggressive
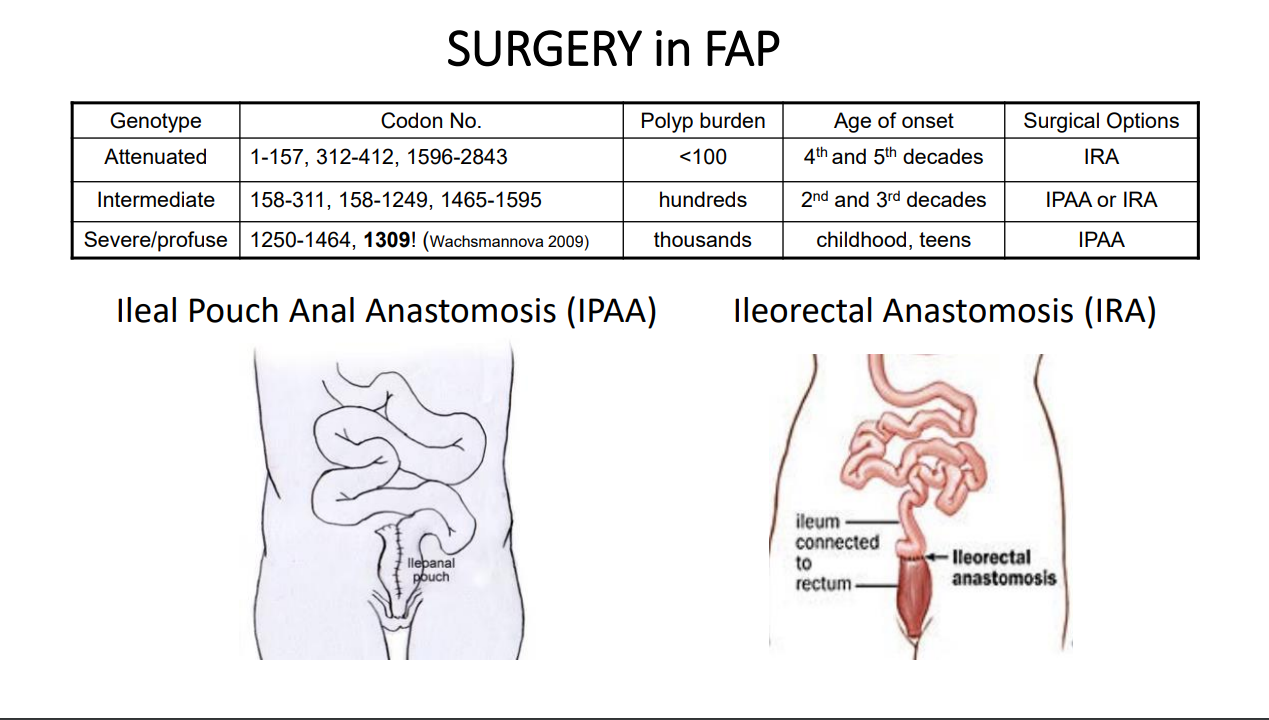
For FAP, timing of potential colectomy involves factors including severity as well as social factors. In teenagers in which there is a concern about being lost to follow-up, this is a factor that could influence earlier intervention
Many times a 2nd opinion in pathology can be helpful, especially if colon cancer is reported. However, histologic dysplasia can be tricky as well
Isolated CHRPE usually does not require evaluation. Dr. Erdman noted that sometimes genetic testing is offered to a family for reassurance. He discouraged colonoscopy in this setting unless a genetic diagnosis has been established or symptoms like rectal bleeding are present. The penetrance of APC mutations (development of polyps) can be quite variable (especially with attenuated form)
Case #1 presented a 14 yo with 50+ multilobulated pedunculated polyps which histologically were tubulovillus adenomas. Initial diagnosis was elusive despite extensive testing
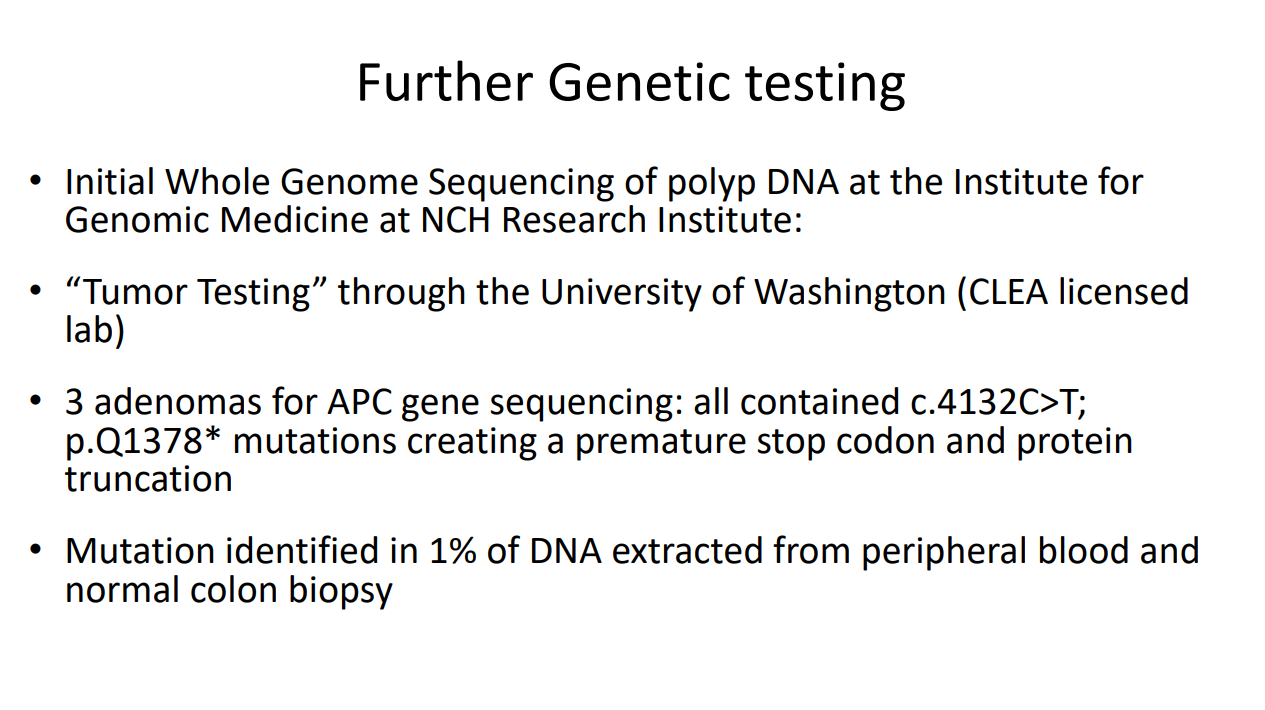
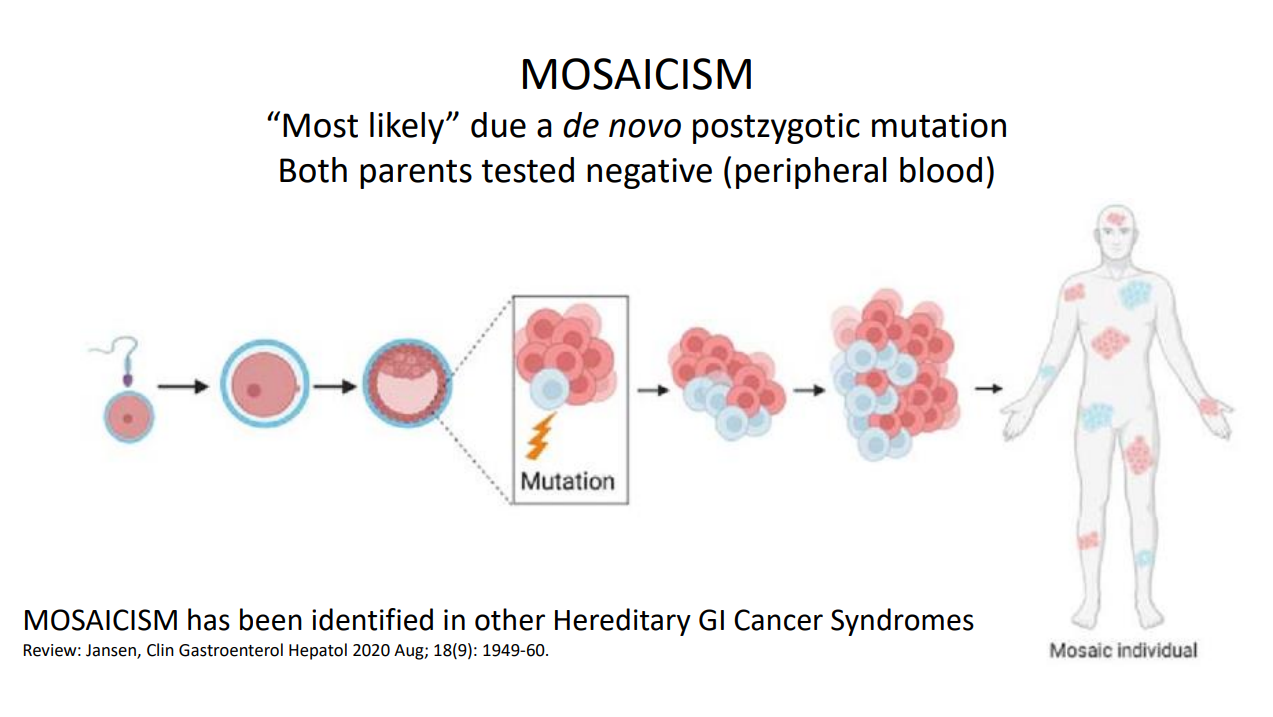
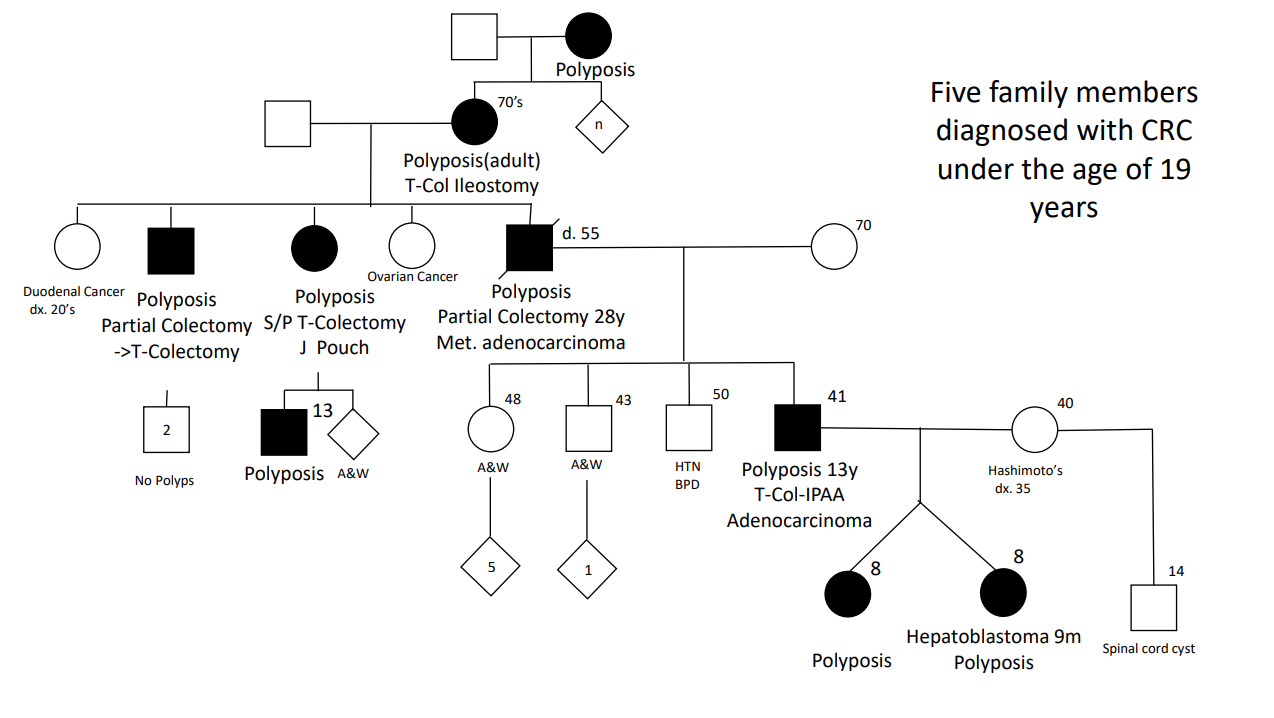
Case#2 presented 8 yo twins. Aggressive management was indicated as 5 family members developed colorectal cancer prior to age 20 years.
Case#2 Improvements in testing allowed identification of a point mutation in the 1B promoter region of the APC gene
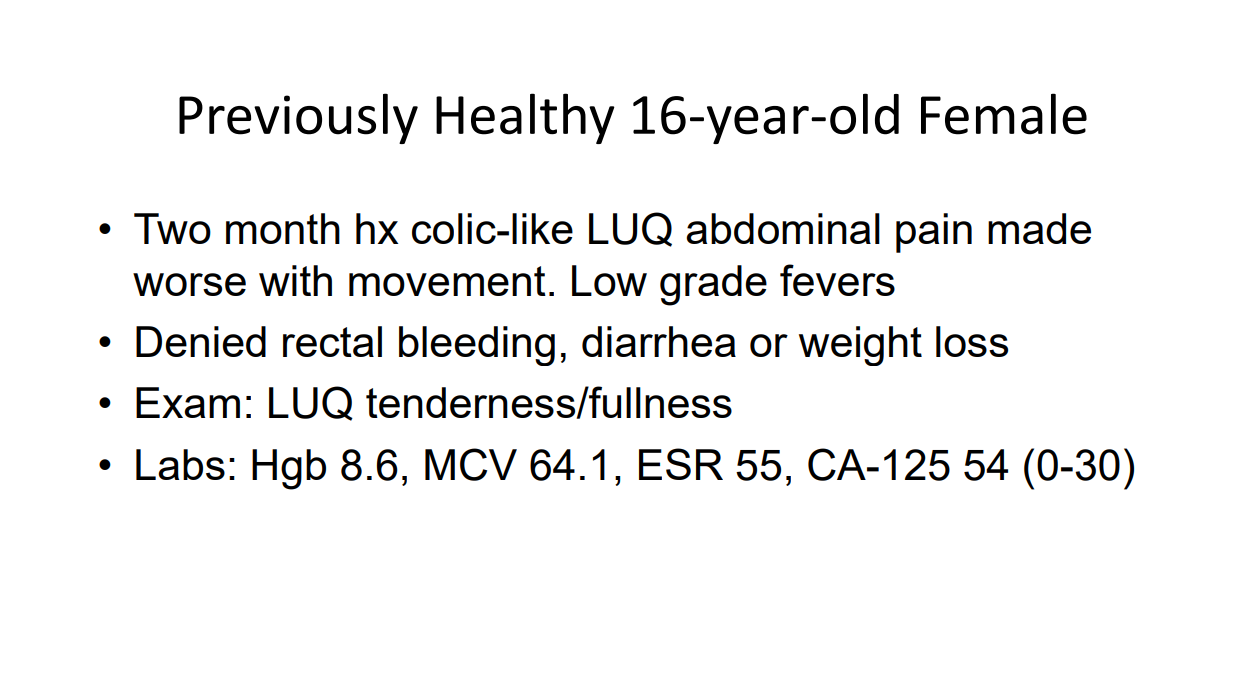
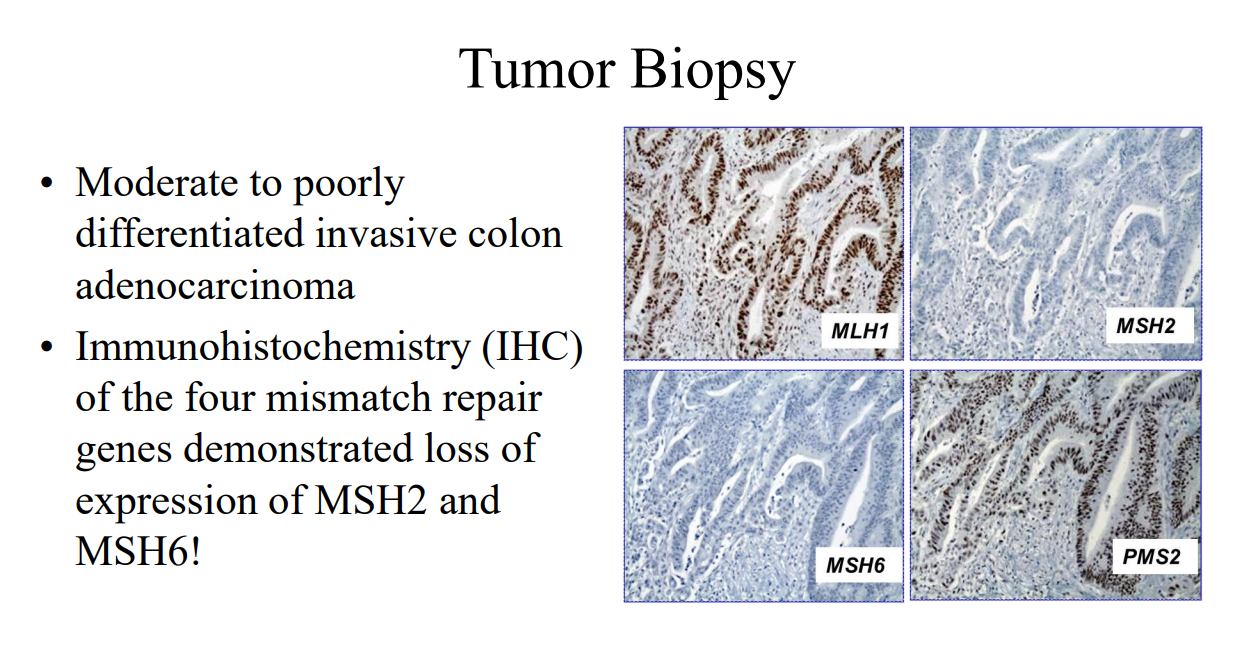
Case#3 presented a 16 yo with anemia and pain who was found to have a colonic mass related to mismatch repair mutation. Dr. Erdman indicated that obtaining adequate tissue for a diagnosis (“dig a hole”) is important. (As an aside, other colleagues have had the experience of tumors which were highly vascular and it is important to keep this possibility in mind)
Amsterdam II Criteria for Lynch Syndrome
Case#4 presented a 12 yo with neurofibromatosis (NF-1) who developed CRC and ultimately diagnosed with CMMR-D. This is a highly aggressive cancer susceptibility disorder with a very poor prognosis (see post: Are you familiar with CMMR-D?)
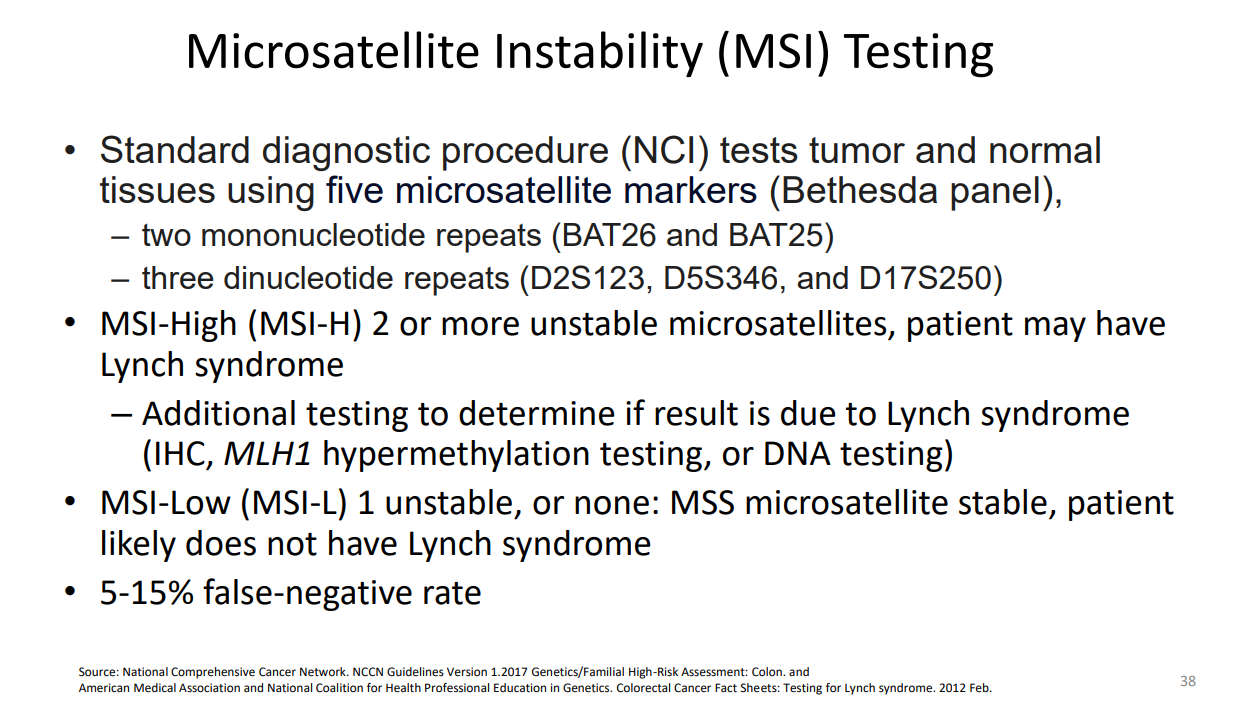
Case#5 presented two siblings (13 yo, 17 yo) who had half-sibling who died from CRC at age 25 yrs. This case illustrated “genetic anticipation” as each generation in this family with Lynch syndrome tended to develop CRC earlier in life. Amsterdam criteria can be helpful in identifying Lynch syndrome
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
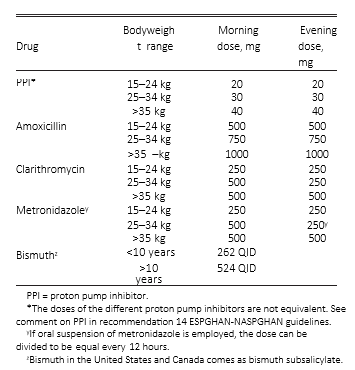
C Andrews et al. J Pediatr Gastroenterol Nutr. 2024;79:35–41. Impact of medication dosage on Helicobacter pylori eradication rates among pediatric patients
As I write this post on July 1st, I recollect having to learn the weight-based dosing of acetaminophen during my first day of pediatric internship. Even at this early stage, it was quite clear of the importance of getting the right dose. This article makes clear that there is a lot of room for improvement in dosing with regards to H pylori.
This retrospective study examined 144 children. Correct dosing was based on ESPGHAN-NASPGHAN guidelines:
Key findings:
The overall eradication rate was 73.6% (“well below the greater than 90% optimal eradication cut-off for H. pylori therapies”)
There was a high rate of improper weight‐based dosing: proton pump inhibitor(PPI) 31.2% (45/144), amoxicillin 31.7% (39/123), metronidazole (MET) 19.4% (12/62), clarithromycin (CLA) 23.9% (22/70), tetracycline 50% (6/12), bismuth 26.1% (6/23).
When PPIs were properly weight‐dosed, there was a 78.8% eradication rate that dropped to 62.2% with suboptimal dosing (p = 0.036, odds ratio [OR]: 2.26). The dose of PPI was incorrect in 45 patients.
When amoxicillin was properly weight‐dosed, successful eradication was achieved in 81% versus only 53.8% when improperly dosed (p = 0.002; OR: 3.64). The dose of amoxicillin was incorrect in 39 patients. There was no statistically significant impact on eradication rates with improper weight‐based dosing of MET, CLA, tetracycline, or bismuth.
My take: It is worthwhile to double-check on dosing for H pylori treatments -it results in better eradication rates. Also, in this study, as expected, quadruple therapy regimens had higher success rates (85% eradication); however, it was used in only 20 patients. In patients (virtually all of my patients) without known antimicrobial sensitivity, it has been my practice to use quadruple therapy (related post: Quadruple Therapy for Helicobacter Pylori Favored in Toronto Guidelines).
This retrospective study examined 546 children with esophageal atresia (EA) who underwent 1,473 surveillance endoscopies (2004-2023). The authors defined a hiatal hernia as at least 1 cm of gastric folds present above the level of the diaphragmatic pinch. “Actionable findings” were any finding that prompted a change in management.
Key findings:
A total of 770 endoscopies (52.2%) in 394 unique patients (72.2%) had actionable pathology
The most common actionable finding was esophagitis which lead to escalation of therapy (484 endoscopies in 32.9% of patients). However, de-escalation of therapy was common as well; this occurred in 233 patients (after 310 endoscopies)
Barrett’s esophagus (intestinal metaplasia) was identified in 7 unique patients (1.3%) at a median age of 11.3 years. 6 of 7 patients with Barrett’s were receiving acid suppression at time of diagnosis
Actionable findings leading to surgical intervention were found in 55 children (30 refractory reflux and 25 tracheoesophageal fistulas).
Significant predictors of actionable pathology included increasing age, long gap atresia, and hiatal hernia.
Symptoms were not predictive of actionable findings, except dysphagia (OR 5.80), which was associated with stricture.
Acid suppression was associated with a reduced odds of actionable findings (OR 0.78); however, there was still a high rate of actionable findings in this group. 51% of endoscopies while a patient had been receiving acid suppression had actionable findings.
Fundoplication was NOT associated with protection against actionable findings (OR 1.42)
Table 2 notes that 52 (3.5%) patients had eosinophilic esophagitis therapy escalated. Infrequently, non-esophageal diseases were identified: Celiac in 3 patients (0.2%), Crohn’s disease in 2 patients (0.1%), eosinophilic gastritis and/or duodenitis in 2 (0.1%), and H pylori in 4 patients (0.3%).
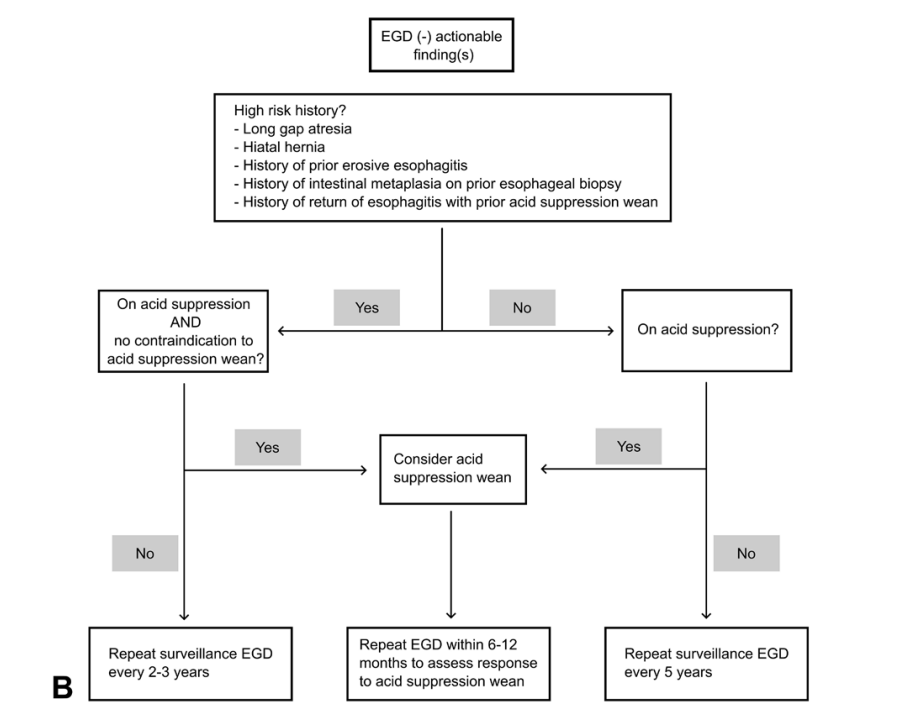
Proposed Management Algorithms:
Discussion Points (from authors):
Take multiple levels of esophageal biopsies: “Any surveillance esophagogastroduodenoscopy (EGD) should at minimum include 2 to 3 levels of esophageal biopsies”
Acid suppression recommendations: “Barrett’s esophagus is proposed to be an absolute contraindication to acid suppression wean; relative contraindications to weaning acid suppression include earlier erosive esophagitis, earlier failed acid suppression discontinuation attempt(s) with rebound esophagitis, or hiatal hernia; if acid suppression is weaned in these high-risk situations, we believe close follow-up endoscopy is warranted to assess for rebound pathology [which happened in nearly 20%].” And, “our practice is to empirically de-escalate acid suppression in children without contraindications to doing so when there is no gross esophagitis and biopsies show no or minimal inflammation (generally less than 5 eosinophils per high powered field).”
Consider doing endoscopy off acid suppression for approximately three months: “To maximize the information yield from the initial endoscopy, a patient may first wean off acid suppression approximately 3 months before endoscopy to permit evaluation for both anatomy and esophagitis off acid suppression. Subsequent surveillance is performed according to our algorithm and within at most 6 to 12 months of any acid suppression changes.”
The authors do not generally recommend pH-Impedance. “There are no consensus “normal” values for pH-impedance reflux parameters in either healthy or EA children, and pH-impedance has failed to show any predictive correlation with actual esophagitis in multiple pediatric studies. In particular, children with EA with “normal” numbers of reflux events cannot adequately clear their refluxate in the context of poor esophageal motility and can still develop reflux injury. pH-impedance tracings in EA require manual review by an experienced reader, with automated analysis being highly unreliable in the setting of low baseline impedance values.”
Limitations: 1. Some of the actionable findings may have been expected based on prior endoscopies (e.g. prior stricture) and could influence value of symptoms like dysphagia. 2. This population was skewed to patients with more severe EA as it is a subspecialty center. One indicator was that their group had 24% with long-gap EA compared to an overall expected rate of 10% in the general EA population 3. Retrospective study 4. Many of the patients were not truly “surveillance” endoscopies but were done due to reported symptoms
My take: It’s unfortunate that this article did not get published in a more mainstream pediatric journal (e.g. JPGN, J Pediatr, Pediatrics) or a more mainstream gastroenterology journal (eg. Gastroenterol, Clin Gastroenterol Hepatol, AJG) as this article provides a lot of great data and useful advice. More than 70% of subjects had actionable findings during the course of their follow-up, including more than 40% of 1 year-olds.
The algorithms above suggest that at minimum, EA patients should have endoscopy every 5 years (likely starting between 12-18 months). More frequent endoscopy (every 2-3 years) may be worthwhile in those with risk factors (e.g. long gap EA, hiatal hernia, and prior esophagitis) and follow-up endoscopy is needed sooner if change in therapy (stricture dilation, esophagitis treatment or treatment de-escalation).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
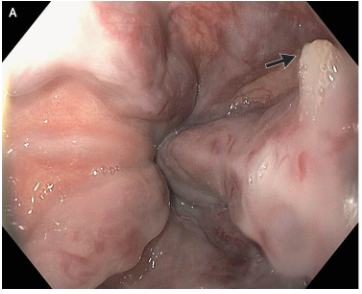
M Najem, E Dong. N Engl J Med 2024;390: e47. Esophageal Varices, White-Nipple Sign, and Portal Hypertensive Gastropathy
This case reported on a 66 year old with cirrhosis and variceal bleeding. “One varix had a “white-nipple sign” (Panel A, arrow), which indicates recent variceal hemorrhage and results from the formation of a fibrin plug at the site of a resolved thrombus.”
“Though not widely mentioned as a stigma of recent variceal hemorrhage, this finding was first reported by Chung and Lewis in 1984 [4]. They described it as a white nipple on top of a varix protruding into the lumen and noted its presence in up to 5% of cases of variceal bleeding. It was thought to represent a platelet-fibrin plug at the site of recent variceal rupture. They noted that dislodgement would be accompanied by jet-like bleeding and called it ‘Mount St. Helens’ sign’ due its volcanic-like eruption…As Chung and Lewis [4] initially suggested, it should ‘alert the endoscopist to take urgent measures to avert a disaster’. Recognizing it as such, attempts to dislodge the lesion must be avoided and endoscopic therapy should be undertaken.”
#NASPGHAN19 Liver Symposium (excellent presentation by Dr. Romero on varices in children and portal hypertension)
Time to Adjust the Knowledge Doubling Curve in Hepatology For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
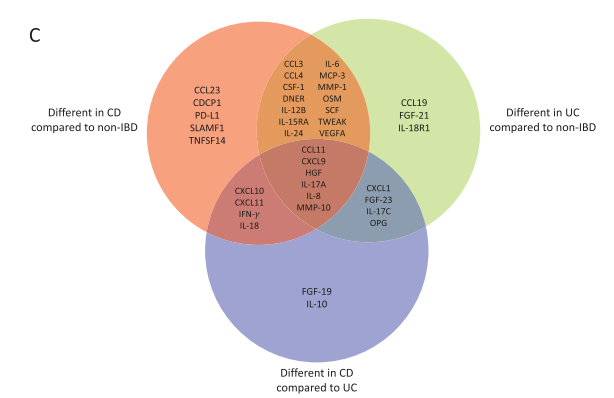
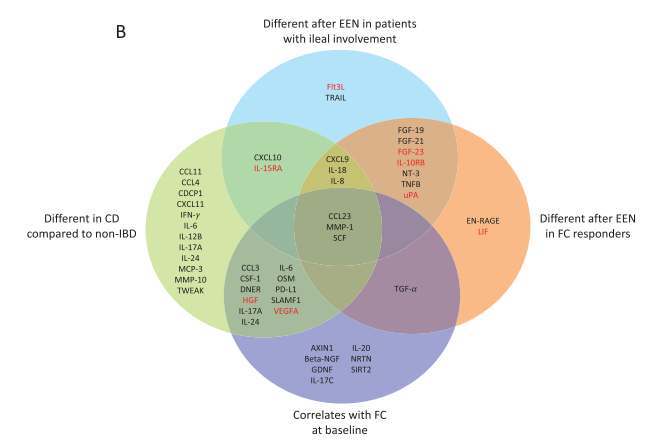
Background/Methods: The authors characterized the plasma levels of inflammation-related proteins (IRPs) in children with CD and ulcerative colitis (UC) compared with noninflammatory controls (non-IBD) and explored the effect of EEN in children with CD. Population included children with CD (n = 53), UC (n = 11), and non-IBD (n = 19). For 18 children with active CD, IRPs were measured before and after 8 weeks of EEN.
Key findings:
Compared with non-IBD, patients with active UC and CD had different levels of 27 (24 raised, 3 decreased) and 29 (26 raised, 3 decreased) IRPs, respectively.
Exclusive enteral nutrition modified the levels of 19 IRPs (13 increased, 6 decreased including CCL23, interleukin-24, interleukin-6, and MMP-1).
More pronounced changes in IRP profile were observed in patients with ileal involvement and a ≥50% decrease in fecal calprotectin during EEN.
The discussion notes that “these profiles also helped to uncover some of the underlining pathological mechanisms, with CD demonstrating enhanced levels of IRPs related to IFN-γ and Th1-associated pathways, whereas in UC we observed an enrichment in IRPs related to Th17 pathways.”
My take (borrowed from authors): Inflammation-related protein profiles could help to stratify patients likely to respond to treatment with EEN.
, Venn diagram of the proteins found to be signifcantly different between each IBD subtype compared to non-IBD controls and between each IBD subtype.Venn diagram summarizing the main significant (P ≤ .05) differences or correlations found in IRPs. Proteins highlighted in red were shown to significantly interact with thiopurines
Methods: Using a population-based claims database in Japan, the authors identified patients who were prescribed a clarithromycin-based first regimen of Hp eradication between 2015 and 2018.
Key findings:
Among 54,055 patients, 568 (1.05%) developed gastric cancer (GC) during the follow-up period (mean, 3.65 years).
The cumulative incidence of GC was 1.64% at 3 years, 2.02% at 4 years, and 2.36% at 5 years in potassium-competitive acid blocker (PCAB) users and 0.71% at 3 years, 1.04% at 4 years, and 1.22% at 5 years in H2RA users.
Limitations: retrospective study with issues of selection bias and confounding.
In the discussion, the authors note PCABs are being used not only for Hp eradication but for peptic ulcers, reflux and several abdominal symptoms. “According to the results of our study, longer use of PCABs was particularly associated with the increased risk of GC after Hp eradication…it might be better to switch strong acid inhibitors including PCABs ad PPIs to H2RAs before reaching a lengthy prescription period (eg. more than 3 years).”
This multicenter, prospective, randomized controlled, noninferiority trial enrolled patients (n=516) with treatment naive H pylori infection from 5 clinical centers. All patients received vonoprazan at 20 mg 2/day. The high dose amoxicillin was 750 mg 4/day and the low dose 1000 mg 2/day.
Key findings:
The high-dose amoxicillin combination with vonoprazan regimen, for either 10 or 14 days, was effective and safe in eradicating H pylori, whereas the low-dose amoxicillin regimen for 10 days was less effective. The high-dose per protocol eradication rates were 90.9% vs 94.5 for 10 vs 14 days compared to 82.0% in the low-dose per protocol eradication rate (for 14 days).
My take: These studies indicate that PCABs are more effective at healing erosive esophagitis as well as H pylori gastritis. However, particularly in patients with Hp infection, the use of PCABs is associated with an increased risk of gastric cancer. The exact long-term risk of strong acid inhibition is unclear, especially in those without a history of Hp infection.
Background: “Coconut water (CW) possesses anti-inflammatory properties, can potentially manipulate the microbiome, is a rich source of dietary potassium,” and may be an effective treatment for mild to moderate ulcerative colitis (UC).
Methods: Along with standard medical therapy, four hundred mL of CW (200 mL 2/day) or placebo fluid was administered for 8 weeks to adults (CW, n = 49; placebo, n = 46) with mild to moderate UC
Key findings:
Clinical response (57.1% vs 28.3%; odds ratio [OR], 3.4), remission (53.1% vs 28.3%; OR, 2.9), and proportion of patients with fecal calprotectin (FCP) <150 μg/g (30.6% vs 6.5%; OR, 6.3) all significantly favored CW group
There was not a significant difference in endoscopic outcomes
The authors indicate CW may be a useful adjunct for mild to moderate colitis but should be avoided in those patients taking medications that affect potassium and those with chronic kidney disease.
My take: This would be a good study to repeat to confirm whether CW is helpful for colitis. Certainly too much CW (a high FODMAP beverage) can contribute to a laxative effect and elevated potassium in some people. If a person with colitis is stranded on an island, CW may help until a rescue arrives.
In this prospective observational real-world treatment registry…
Key findings:
Of 1515 adalimumab-treated patients, 763 (50.4%) were classified as responders at 6 months
Compared with nonresponders, responders were less likely to have moderate to severe symptoms (55.6% vs 33%), or require steroids (45.5% vs 17.3%) or opiates (6.6% vs 1.3%) at baseline
During follow-up evaluation, using stabilized inverse probability of treatment weighting, responders were 34% less likely to experience serious infections compared with nonresponders (hazard ratio, 0.66)
The study results are similar to a registry-based rheumatoid arthritis study by Strangfeld et al (Ann Rheu m Dis 2011; 70: 1914-1920), which showed effective treatment was associated with less steroid use and a decline int risk of serious infections.
My take: This study indicates that lack of control of CD increases the risk for complications and infections. So, while patients are concerned about medication adverse effects, the complications of foregoing treatment or ineffective treatment are usually more concerning.
Methods: This was a multicenter retrospective review of patient characteristics and evaluation of all hematochezia events in patients (n=121 patients with 180 events) with CHD <6 months admitted to acute care cardiology unit at 3 high-volume tertiary care centers from February 2019 to January 2021. In total, 61% of affected patients had single-ventricle physiology (38% hypoplastic left heart syndrome). Most patients (81%) were full-term.
Key findings:
77% of hematochezia events were benign, and 23% were due to necrotizing enterocolitis (NEC). There were no surgical interventions for NEC or deaths from NEC.
Those with NEC were significantly younger (34 vs 56 days, P < .01) and smaller (3.7 vs 4 kg, P < .01). Single-ventricle physiology was significantly associated with NEC.
Bloodwork (CBC, WBC, CRP, Blood Culture) did not aid diagnosis
My take: If concerned about NEC which is increased in those with congenital heart disease, obtain an AXR. Overall, the outcomes of NEC in this cohort were good –all resolved with medical management.