K Papamichael et al.Clin Gastroenterol Hepatol 2024; 22: 2134-2136.
Higher Adalimumab Concentration Is Associated With Complete Fistula Healing in Patients With Perianal Fistulizing Crohn’s Disease
In this multicenter retrospective review with 183 patients, the adalimumab (ADM) levels were examined with respect to healing of perianal fistulas. Most patients (82%) had complex perianal fistulizing CD.
Key findings:
- 87 patients (48%) received intensified dosing at the time of therapeutic drug monitoring (TDM)
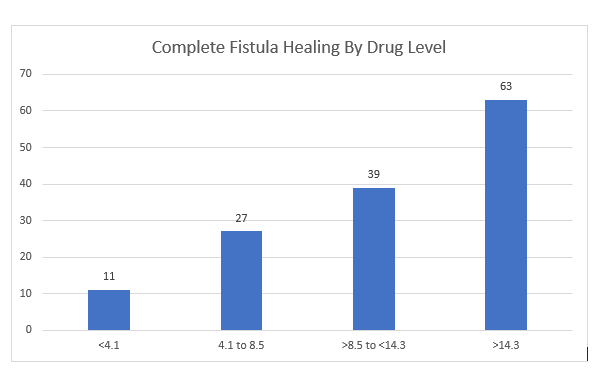
- Patients with complete fistula healing (CFH) had higher median ADM levels: 12.9 compared to 6.1 for those witout CFH
- “Optimal ADM concentration associated with CFH was 12.2 mcg/mL” which had positive predictive value of 64% and negative predictive value of 80%. Among those with ADM >12.1, CFH was achieved in 64% compared to 20.5% in those with concentrations <12.1 (Odds ratio, 5.7). “Even higher drug levels may be needed.”
My take: There is a lot of data supporting TDM, including proactive TDM, with anti-TNF agents like adalimumab and infliximab. This study shows that with fistulizing disease higher drug levels are needed to achieve better outcomes.
Related blog posts:
- Proactive Therapeutic Drug Monitoring and Better Outcomes in Pediatric Crohn’s Disease (2024)
- Picking Apart the SERENE-CD Study & Constipation Vibrating Capsule FDA Approved
- Expert Consensus: New Recommendations for Therapeutic Drug Monitoring (2021)
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD? (2019)
- Proactive Therapeutic Drug Monitoring -Different Time Points
- Implications of Serene Studies
- SERENE Study: Does a Higher Induction Dose of Adalimumab Help for Crohn’s Disease?
- Low Anti-TNF Levels or Antibodies Are Associated with Antibodies to Subsequent Anti-TNF Agent
- Better Levels –>Better Outcomes with Adalimumab
- “Do Not Stop Anti-TNF Medications in Children with IBD When They Are Working”
- For Next Insurance Appeal: TDM for Adalimumab & Satire on PA
- Here’s the Proof That Proactive Therapeutic Drug Monitoring Improves Outcomes in Children with Crohn’s Disease
- Kids Are Different: Therapeutic Drug Monitoring