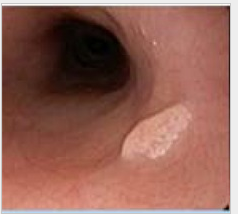
This is a case report of 4 cases of esophageal squamous papilloma (ESP); Three out of the 4 cases of ESP identified at our institution were positive for HPV in situ hybridization.
“Chronic mucosal irritation due to GERD or HPV is thought to be the most common cause of ESP…a recent study failed to identify a relationship between the prevalence of HPV and the occurrence of ESP in pediatric patients”
“Small esophageal lesions can be managed by excisional biopsy; however, conservative management is advised when the disease is extensive to avoid mucosal scarring and stenosis…Acid suppression may decrease ongoing inflammation.”
“Vaccinating children with active HPV infection could theoretically increase the immune response and potentially aid in clearance of lesions caused by the disease.”
“A 17-year-old … presented with cachexia, nonbilious, nonbloody emesis, lower abdominal discomfort, and decreased oral intake for four days and 40 lb weight loss for 1 year”…Lipase was 4544 U/L, and abdominal ultrasound was reported as normal. Due to “persistent emesis, despite being on bowel rest… CT abdomen and pelvis was performed, which showed a massively dilated stomach and duodenum with cutoff at the third portion of the duodenum..due to the severity of the obstruction, duodenojejunal anastomosis, and gastrostomy tube placement were performed.”
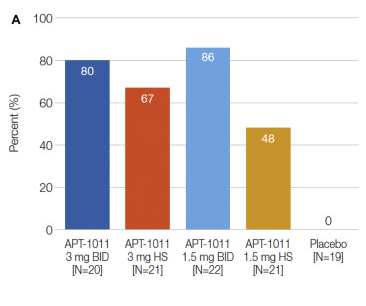
Methods: In this randomized, double-blind, placebo-controlled, dose-finding, phase 2b trial, 106 adults with EoE received 1 of 4 APT-1011 (fluticasone propionate oral disintegrating tablet) doses or placebo for a 12-week induction period and 40 weeks of maintenance.
Key findings:
Histologic response (≤6 eosinophils per high-power field at Week 12) rates were 0% for placebo, 80% for APT-1011 3 mg twice daily (BID), 67% for 3 mg at bedtime (HS), 86% for 1.5 mg BID, 48% for 1.5 mg HS (P < .001 for all groups vs placebo).
There was also improvement in treatment group in dysphagia and EoE Endoscopic Reference Score (EREFS); the EREFS improved from 4.5 to 2.3 for 3 mg BID, 5.3 to 2.1 for 3 mg HS, 4.6 to 1.7 for 1.5 mg BID, 5.3 to 2.9 for 1.5 mg HS vs 5.2 to 4.5 for placebo. See Figure 2 for 52 week trend in EREFS.
Candidiasis: For the 3-mg BID group, oral and esophageal candidiasis was 40% in Part 1 and 32% in Part 2, 18% and 16% for 1.5 mg BID, and 5% and 7% for 3 mg HS (same subject)
Low morning cortisol noted 3 times in part 1 and 5 times in part 2. “All cortisol test abnormalities resolved upon retesting, with no dose adjustment or interruption of treatment.” Adrenal suppression is expected to be low because “FP undergoes extensive first-pass metabolism to inactive metabolites, with bioavailability demonstrated as <1%”
My take: A fluticasone ODT would represent a big improvement compared to current situation of asking families to either spray a pulmonary inhaler down their throat or to create a budesonide slurry using either honey or splenda. How much would this cost?
Histologic responders at Weeks 12. Interestingly, the 1.5 mg BID had a modestly higher response rate at 12 weeks, 26 weeks, and 52 weeks than the the 3 mg BID and the 3 mg qhs dosing groups.
100 adults enrolled in a multisite prospective observational study in which 55 underwent dilatation. Key findings:
In nondilated patients, the association between eos/hpf and symptoms was moderate (ρ = 0.49; P < .001) based on the symptom-based EoE activity index (EEsAI); for a 10-eos/hpf increase, the predicted EEsAI increased by 2.69 (P = .002)
In patients dilated 1 or less and more than 1 year before index endoscopy, this association was abolished (ρ = -0.38; P = .157 for ≤1 y and ρ = 0.02; P = .883 >1 y)
Limitations: sample size (only 25% subset of total cohort due to missing data), cross-sectional study design
My take: This finding is a double-edge sword. The good part is that dilatation improves dysphagia despite ongoing inflammation which may be refractory to current medical treatments. The bad part is this dissociation in symptoms makes it less likely for patients to be adherent to therapy.
Design: Patients completed 1 week of observation prior to randomization to 1 of 2 counterbalanced groups: OLP for 3 weeks followed by a 3-week control period or control period for 3 weeks followed by OLP for 3 weeks. During the OLP period, participants took 1.5 mL of an inert liquid placebo twice a day.
Key findings:
The mean (SD) pain scores were significantly lower during open label placebo (OLP) treatment compared with the control period (39.9 [18.9] vs 45.0 [14.7]; difference, 5.2; 95% CI, 0.2-10.1; P = .03)
Patients took nearly twice as many hyoscyamine pills during the control period compared with during the OLP period (mean [SD] number, 3.8 [5.1] pills vs 2.0 [3.0] pills; difference, 1.8 pills; 95% CI, 0.5-3.1 pills)
My take: It is a mistake to consider placebo as a treatment for functional abdominal pain. In many children, pain fluctuates and may improve with reassurance, distraction, healthier diets, and physical activity. However, we also need more effective therapies including pain psychology, dietary approaches and medications. The idea that placebo helps is misleading and undermines the fact that patients with functional disorders need effective treatment.
“Let me say at the outset that in my primary care clinic I practice low-value care. Not every day, but often enough. Probably every week”
“Choosing Wisely was an immediate public relations win for the medical profession in 2012, demonstrating that doctors were stepping up to address low value and high costs in medicine. Ten years later, however, it’s clear that making lists and publicizing them are not sufficient to reduce low-value care.1 “
“In the years since Choosing Wisely lists were first released, researchers have noted that specialty societies rarely select income-generating treatments provided by their members for inclusion on the lists.4“
“In short, Choosing Wisely has allowed doctors (and medical societies) to look like they are addressing low-value care without actually being forced to make any substantive changes.”
“My experience mirrors the findings of a 2015 study that used surveys, interviews, and focus groups to assess how patients understood low-value care. The study found ‘quite powerfully” that patients favored “replacing excessive tests with time for clinicians to talk, listen and personalize'”
“If Choosing Wisely is to continue, the specialty societies that have participated in it should celebrate its 10th anniversary by coming together to rethink and reinvent it.”
My take: While there are many factors that make it hard to eliminate low-value care, much is related to Upton Sinclair’s maxim: “It is difficult to get a man to understand something when his salary depends on his not understanding it.”
Case: A 4 yo developed abdominal distention and crepitus after gastrostomy tube (GT) placement. An AXR (see below) showed subcutaneous emphysema (especially in left abdomen). There was no pneumoperitoneum or extravasation of contrast with fluoroscopy. Due to persistent distention, a CT scan was obtained three days after tube placement. The CT scan confirmed appropriate intragastric location of GT and nonspecific dilatation of bowel loops without pneumoperitoneum; the dilated bowel was attributed to an ileus and improved over the next few days. Thanks to colleague for sharing information.
My take: Isolated subcutaneous emphysema is rarely identified after GT placement and requires careful evaluation to assure appropriate insertion site (1,2).
In this retrospective study, among those who developed skin reactions to anti-TNF agents, 71 (64%) continued anti-TNF and 40 (36%) switched to ustekinumab (UST). Key findings:
Switching to UST had a higher rate and odds of resolution of skin findings (29/40 (73%) vs. 24/71 (34%); p <0.0001) and combined remission (21 (52%) vs. 22 (31%); p=0.03) vs. continuing anti-TNF at 6 months
Patients (n=181) on established maintenance IV infliximab who switched to SC CT-P13 were included in this retrospective multi-centre cohort study. Key findings:
Treatment persistence rate was high (N=167, 92.3%) and only 14 patients (7.7%) stopped treatment during the follow-up period. There were low rates of immunogenicity with no change in clinical disease activity indices or biomarkers
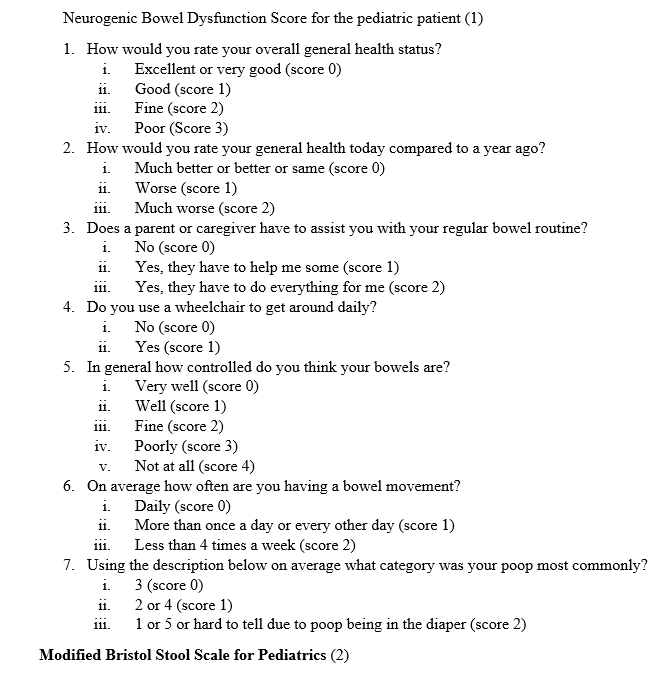
This prospective study (n=80) expands on previous observations regarding the use of a transanal irrigation device for neurogenic bowel management.
Key points:
The neurogenic bowel dysfunction (NBD) score improved at both time points (<6 months, >6 months) by 14 and 13 points respectively. 94% and 98% had improved NBD score at time 1 and time 2 respectively
Patient satisfaction was high, though 8 patients discontinued device early on due to either discomfort or poor results
NBD score can used to monitor treatment effectiveness
This article describes a retrospective review of seven patients with a dual diagnosis of inflammatory bowel disease (IBD) and chronic recurrent multifocal osteomyelitis (CRMO). In their cohort 4 of 6 were receiving anti-TNF therapy at the time of CRMO diagnosis. Misleading statements from this article:
The triad of IBD, CRMO and psoriasis has not been reported previously to their knowledge
“It seems unlikely that anti-TNF-alpha therapy would promote its [CRMO] development”
In JPGN Reports (not available on pubmed), Cordesse et al (JPGN Reports; November 2020 – Volume 1 – Issue 2 – p e007) identified the association of IBD, CRMO and psoriasis; in addition, they identified a paradoxical reaction to anti-TNF-alpha therapy; in this case series of three patients, anti-TNF-alpha therapy triggered CRMO and stopping anti-TNF-alpha therapy led to resolution of CRMO in two of the cases.
In a response to a letter to the editor (Hochman JA. JPGN 2022; DOI: 10.1097/MPG.0000000000003407. Faulty Information Regarding CRMO and IBD), Dushnicky et al (DOI: 10.1097/MPG.0000000000003433) note that JPGN Reports is not available on Pubmed; however, the articles that have described this association are near the top of a google search if one looks for “IBD, CRMO and Psoriasis.” Interestingly, in their response to the letter to the editor, the authors did not amend their claim that anti-TNF therapy is unlikely to promote CRMO despite being furnished with information showing that it can. In my view, the situation with CRMO is similar to psoriasis which can be treated with anti-TNF therapy and can paradoxically be caused by anti-TNF agents as well.
My take:
CRMO is important to recognize due to its association with IBD and to realize that antibiotics are not an effective treatment.
Anti-TNF-alpha agents can cause CRMO in some patients.
In 2022, a web browser search (eg Google), in addition to Pubmed, is probably worthwhile when claiming that this is the first case of xyz ‘to our knowledge.’