In this pilot study, 12 individuals completed a web-based curriculum for VCE proficiency.
Key finding:
Participants showed significant improvement in knowledge (P = 0.041) and photo recognition posttests (P = 0.015). All participants who completed the curriculum found it helpful and reported that they would recommend it to their colleagues
The discussion notes that “Studies have demonstrated that competence with VCE develops in an endoscopist after reading 10–15 VCE studies (6,10). There are some newer guidelines that suggest that this number may be higher…[and] it requires continuous practice. Pediatric gastroenterologists may feel their skills are not adequate when VCEs are not performed on a consistent basis at their institution”
Previous studies have shown an association between the early use of antibiotics and an increased risk of inflammatory bowel disease. A recent study examined all the children born in Denmark from 1995-2009 and followed them up to 2013 via a prospectively maintained database.
During a median 9.5 years (9.3 million total person-years), CD was diagnosed in 208 of 979,039 children.
Key findings:
Antibiotic use in the first year of life was associated with a higher risk of CD (adjusted hazard ratio, 1.4)…with the highest risk with ≥6 courses of antibiotics (adjusted hazard ratio, 4.1)
The cumulative risk of CD at the 11th birthday for children exposed to antibiotics in their first year of life was 0.16% compared to 0.11% for children unexposed to antibiotics in their first year of life.
My take: This study indicates that antibiotics (and/or serious infections) are associated with an increased the risk of pediatric Crohn’s disease but the absolute risk is very low. We still have a lot to learn about how environmental exposures, including diet, infections, antibiotics, and pollution, contribute to the increasing prevalence of inflammatory bowel disease.
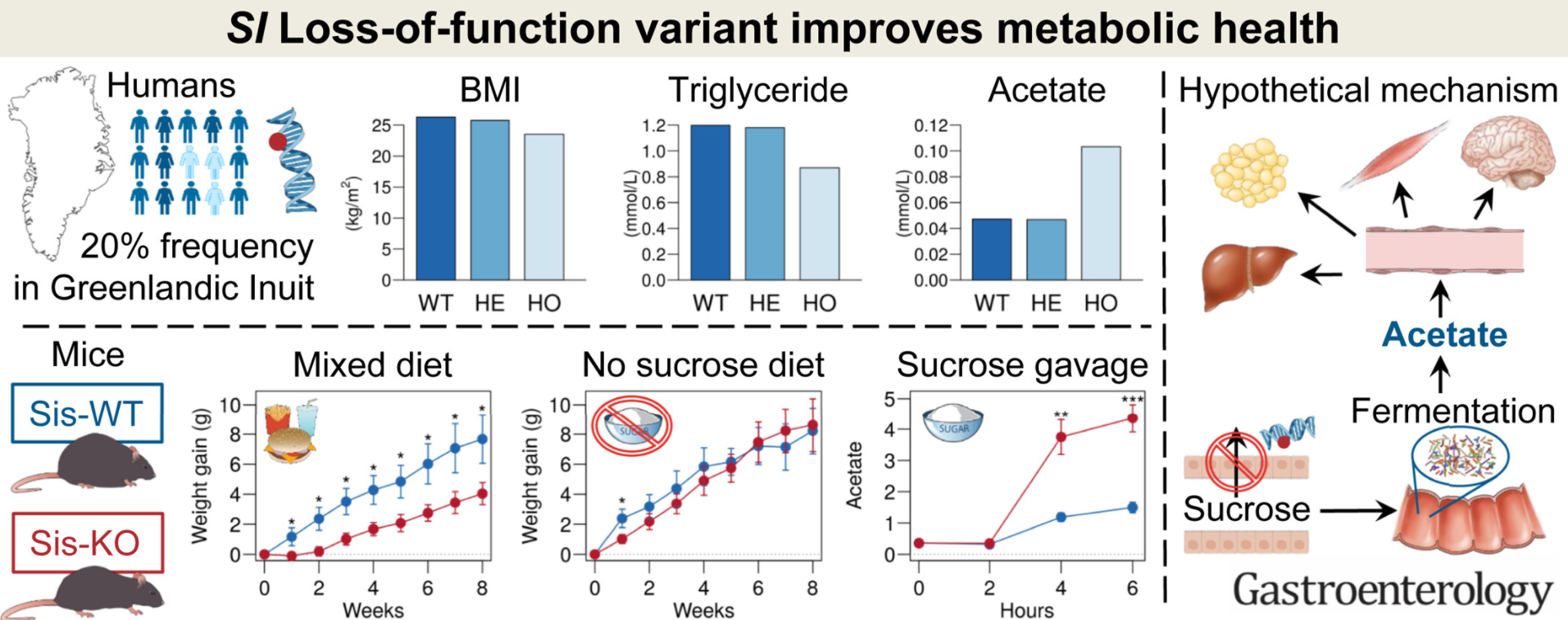
It is well-recognized that genetic mutations that persist often confer some advantages. For example, sickle cell trait (but not disease) provides protection against malaria.
Methods: “The association between c.273_274delAG and phenotypes related to metabolic health was assessed in 2 cohorts of Greenlandic adults (n = 4922 and n = 1629). A sucrase-isomaltase knockout (Sis-KO) mouse model was used to further elucidate the findings”
Key findings:
Homozygous carriers of the variant had a markedly healthier metabolic profile than the remaining population, including lower body mass index ( –2.0 kg/m2; P = 3.1 × 10–5), body weight (–4.8 kg; P = 5.1 × 10–4), fat percentage (–3.3%; P = 3.7 × 10–4), fasting triglyceride (–0.27 mmol/L; P = 2.3 × 10–6), and remnant cholesterol (–0.11 mmol/L; P = 4.2 × 10–5).
The metabolic profile “was likely mediated partly by higher circulating levels of acetate observed in homozygous carriers” (0.056 mmol/L; P = 2.1 × 10–26), and partly by reduced sucrose uptake, but not lower caloric intake.
“These findings were verified in Sis-KO mice, which, compared with wild-type mice, were leaner on a sucrose-containing diet, despite similar caloric intake, had significantly higher plasma acetate levels in response to a sucrose gavage, and had lower plasma glucose level in response to a sucrose-tolerance test.”
My take: It should not be surprising that a genetic condition that results in limited sucrose intake would have health benefits. Perhaps correcting this condition will result in unexpected health issues similar to health issues that can develop in those with celiac disease after institution of a gluten-free diet (Gastroenterol 2013; 144: 912-17).
Background: “Proton pump inhibitors (PPIs) are among the most commonly used medications in the United States, if not the world. Observational studies have demonstrated that PPI use has increased over time and that 7%–15% of patients use these medications at any time, with the prevalence increasing to 40% for patients 70 years or older…In a large observational study examining ambulatory visits of PPI users, nearly two-thirds had no clear indication for PPI use.”
Some of the best practice advice:
Best Practice Advice 2 All patients taking a PPI should have a regular review of the ongoing indications for use and documentation of that indication. This review should be the responsibility of the patient’s primary care provider.
Best Practice Advice 3 Most patients with an indication for chronic PPI use who take twice-daily dosing should be considered for step down to once-daily PPI.
Best Practice Advice 4 Patients with complicated gastroesophageal reflux disease, such as those with a history of severe erosive esophagitis, esophageal ulcer, or peptic stricture, should generally not be considered for PPI discontinuation.
Best Practice Advice 5 Patients with known Barrett’s esophagus, eosinophilic esophagitis, or idiopathic pulmonary fibrosis should generally not be considered for a trial of de-prescribing.
Best Practice Advice 7 Patients at high risk for upper gastrointestinal bleeding should not be considered for PPI de-prescribing.
Best Practice Advice 10 The decision to discontinue PPIs should be based solely on the lack of an indication for PPI use, and not because of concern for PAAEs (PPI-associated adverse events).
My take: There are a lot of individuals who could benefit from de-prescribing PPIs.
When I first saw this title, I mistakenly thought the title indicated that celiac disease (CD) occurred less often in those with inflammatory bowel disease (IBD). This would have been surprising given previous studies have found the opposite. In fact, this study confirms the bidirectional associated risk between patients with CD and in patients with IBD but with a twist. Most IBD treatments were associated with a lower risk of developing CD than those who were not treated.
Database study: Of the 72,965,940 individuals in the database (1999-2020), 133,400 had celiac disease (CD) (0.18%), 191,570 (0.26%) had ulcerative colitis (UC), and 230,670 (0.32%) had Crohn disease.
Key findings:
Patients with IBD were more likely to have a diagnosis of celiac disease (odds ratio [OR], 13.680), with a greater association with Crohn disease (OR 24.473).
Treated patients with IBD with UC and with Crohn disease, respectively, had a lower risk association with CD compared to those not undergoing IBD treatment, specifically corticosteroids (OR, 0.407 and 0.585), 5-aminosalicylates (OR, 0.124 and 0.127), immunomodulators (OR, 0.385 and 0.425), and anti-tumor necrosis factor drugs (OR, 0.215 and 0.242)
A new diagnosis of CD after 1 year of IBD diagnosis, was 1.59% for Crohn disease and 0.90% for UC compared to 0.16% in patients without IBD (P<0.0001)
A new diagnosis of IBD, Crohn disease and UC respectively, in patients with celiac disease was 2.75% and 1.11% compared to 0.29% and 0.25% in the non-celiac population (P<0.0001)
A new diagnosis of IBD and celiac disease among patients with microscopic colitis was 10.5% and 2.6% respectively; a new diagnosis of microscopic colitis among patients with celiac disease was 0.01%
My take: This study confirms the bidirectional associated risk between IBD and celiac disease. The risk of developing celiac disease in those with IBD may be lower in those receiving some treatments; however, this assertion is limited by the nature of a database study.
This study evaluated the effects of IB-stim® (Innovative Health Solutions, Versailles, IN, USA) in 20 patients (11-19 years old) with functional pain. This external auricular device with a battery powered generator that creates percutaneous electrical nerve field stimulation (PENFS), targeting cranial nerves V, VII, IX, and X. This device which has been associated with improvement in functional abdominal pain previously was evaluated for its effects on resting and evoked pain and nausea, sleep and psychological functioning, and long-term outcomes.
Key Findings:
During pain evoked by Water Load Symptom Provocation Task (WL-SPT), visual analog scale (VAS) pain intensity and nausea were lower following PENFS compared with baseline (p = 0.004 and p = 0.02, respectively)
After PENFS, resting VAS pain unpleasantness (p = 0.03), abdominal pain (p < 0.0001), pain catastrophizing (p = 0.0004), somatic complaints (0.01), functional disability (p = 0.04), and anxiety (p = 0.02) exhibited significant improvements, and some were sustained long-term.
Self-reported sleep improved after PENFS (p’s < 0.05) as well as actigraphy-derived sleep onset latency (p = 0.03). The authors note that, paradoxically, patients receiving neuromodulators had more trouble with sleep at baseline. “It is hard to tease out if these differences are due to the medications themselves or if the patients on these medications have more severe symptoms that may have a bigger impact on their life”
In assessing predictors of response to PENFS therapy, those with higher pain catastrophizing and somatization had lesser reduction in VAS pain scores, while those with high anxiety had lesser improvements in functioning.
Study limitations: small sample size and lack of control/sham group
In this limited study, PENFS was associated with improvements in pain intensity and nausea through visual analog scales and validated questionnaires. Disability, pain catastrophizing, somatization, and anxiety reduced after four weeks of PENFS and effects were sustained at 6–12 months post-treatment.
My take: Auricular stimulation if feasible (in terms of cost) is a good alternative to pharmacologic therapy. It would be of interest to study outcomes of patients who received this treatment modality compared with those who were treated by well-qualified pain psychologists.
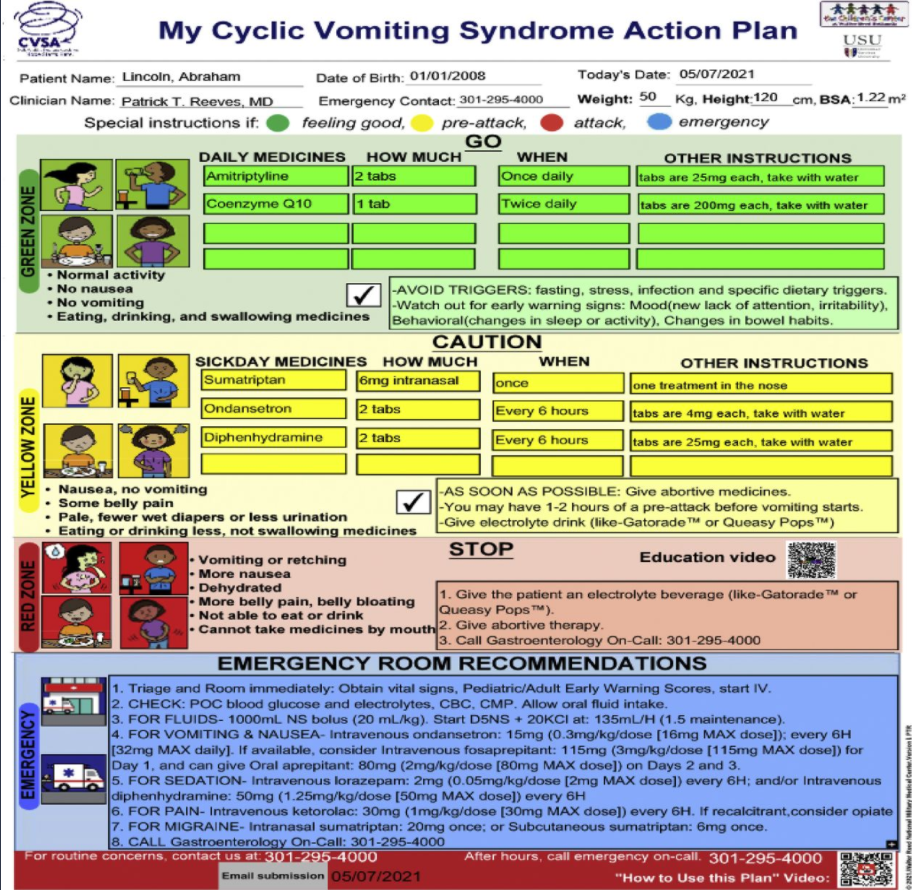
Similar to the constipation action plan (see blog link below), the authors have created a stepwise pictographic CVS action plan (CVSAP).
Image is from Pat Reeves twitter feed and corresponds to figure in study (pg 175)
Key points:
A composite readability score of 5.32 was consistent with a fifth-grade level.
Patients/caregivers (n = 70) judged the CVSAP to be of high quality with consumer information rating form rating of 84.2%
Six medical librarians rated the CVSAP to have 93% understandability and 100% actionability, and 33 clinicians completing the SAM generated a suitability rating of 87.5%
On the listed ED management, the authors note “consider fosaprepitant…and can give oral aprepitant on days 2 and 3.” It should be noted that oral dosing afterwards is generally not required as fosaprepitant can last 2-3 days after a single dose. In addition, many use a maximum dose of 150 mg rather than 115 mg. Also, the ED dosage of several agents need to be tailored to the individual based on weight and other medications. Lower doses of many of the medications in the protocol are often effective.
My take: Patients with cyclic vomiting syndrome, like those with constipation, are likely to benefit from clearly articulated plans for maintenance treatment, escalation approaches and for ED management. The need for ED management may lessen with more consistent treatment approaches.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
This retrospective study (n=45) shows that supplemental water added to blenderized tube feeds may have detrimental effects.
Key finding:
Patients receiving <20% thin liquids were less likely to undergo chest X-rays during follow-up than patients receiving larger amounts of thin liquids (10% in the minimal thin group versus 48% in the greater thin group, P = 0.03)
This relationship remained significant after controlling for underlying pulmonary disease, aspiration, method of feed administration (bolus or continuous feeds), fundoplication status, and oral intake status. CXRs likely indicate concern for pulmonary outcomes related to feedings.
From JPGN twitter feed
My take: Many thick formulas may be difficult to administer via GT. However, using too much water may hinder the benefits of a blenderized diet. Larger prospective studies are needed to determine optimal viscosity diets in these vulnerable populations.
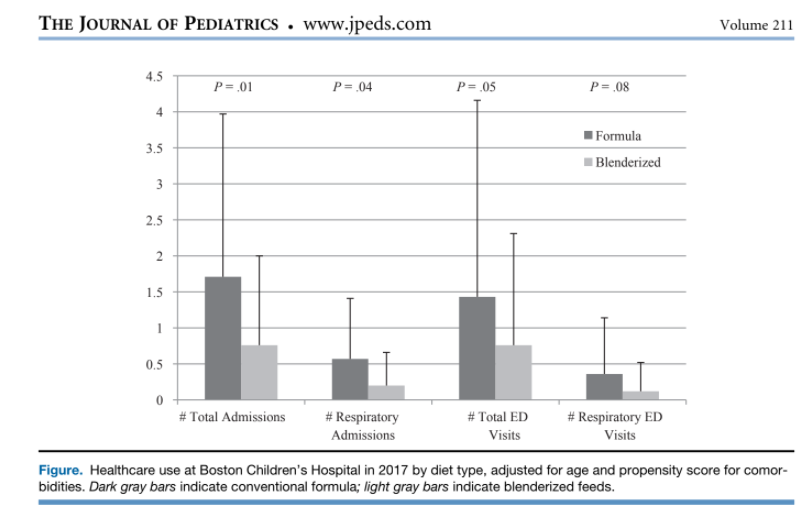
The Boston group has several related articles (Thanks to Alison Miller for sharing these articles):
B Hron et al. J Pediatr 2019;211:139-45. Health Outcomes and Quality of Life Indices of Children Receiving Blenderized Feeds via Enteral Tube
Blenderized diets were associated with decreased healthcare use, improved symptom scores, and increased patient satisfaction compared with conventional formulas.
B Hron, R Rosen. JPGN 2020; 70: e124–e128. Viscosity of Commercial Food-based Formulas and Home-prepared Blenderized Feeds
This article shows that adding 90 mL of water can reduce viscosity of blenderized formula from >6000 cP to ~1000 cP. The authors suggest that those patients with significant reflux may benefit from higher viscosity formulas: “Low viscosity formulas such as Kate Farms and Compleat may not be ideal for patients fed via gastrostomy with significant reflux, in whom extremely thick or possibly moderately thick liquids may have a beneficial impact.”
Commercial food-based formulas vary even more widely, with some meeting criteria for thin liquids (Kate Farms Pediatric 1.2 and Compleat Pediatric), slightly thick (Harvest), mildly thick (Nourish), moderately thick (Compleat Organic Blends, Liquid Hope), and extremely thick (Real Food Blends).
Specific viscosity (cP) listed in Table 1 of this article: