A Goyal et al. JPGN 2020; 71: 563-582 Full text (free). Anemia in Children With Inflammatory Bowel Disease: A Position Paper by the IBD Committee of the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition.
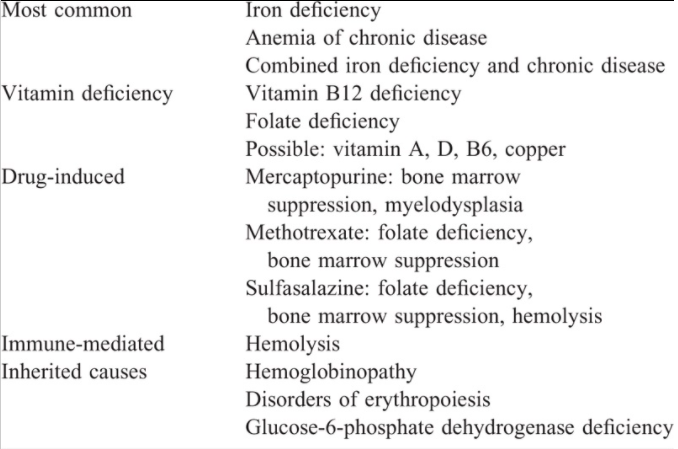
Main Types of Anemia in Inflammatory Bowel Disease:
- “IDA is the most common cause of anemia in children with IBD. True iron deficiency results from a number of factors, including chronic blood loss secondary to gastrointestinal bleeding, decreased iron absorption because of tissue or systemic inflammation and from reduced absorptive surface area. “
- “Functional iron deficiency (FID) results from high levels of circulating hepcidin, which binds to and disables the iron transporter, ferroportin. Under the influence of hepcidin, ferroportin-mediated export of intracellular iron is stalled, leaving the iron trapped within the enterocytes and macrophages… the underlying inflammation, which induces hepcidin production can result in anemia secondary to FID.”
- Anemia of chronic disease (ACD) “occurs from various downstream pathways secondary to inflammation.”
Table 4:
Recommended Testing
- Screening Tests: “initially a complete blood count (CBC), CRP, and ferritin levels should be performed. If a patient is found to be anemic, then testing should include CBC with differential, including mean corpuscular volume (MCV), mean corpuscular Hgb concentration (MCHC), red cell distribution width (RDW), reticulocyte count, CRP, serum ferritin, and transferrin saturation (TSAT)”
- Serum iron level … is … unreliable in the assessment of iron deficiency as the level fluctuates with several variables.
- Transferrin saturation (TSAT) is a measure of the iron content in the circulating transferrin and reflects the availability of utilizable iron
Treatment of Anemia
- In mild anemia (Hgb ≥10 g/dL) and/or quiescent disease, oral iron should be tried first.
- Parenteral iron is indicated when oral iron is ineffective or poorly tolerated, in patients with moderate-severe anemia and/or with active inflammation.
- According to ECCO guidelines, an IV replacement goal of achieving of ferritin level of up to 400 μg/L is more likely to prevent recurrence of anemia…a transferrin saturation of 50% and serum ferritin of 800 μg/L should not be exceeded
- Regarding iron effects on microbiome: studies indicate that dysbiosis at baseline worsens the unfavorable shifts in microbiome with oral iron therapy…Our position, however, is that further studies are required in humans before any reliable conclusions can be drawn. [My question: have the effects of oral iron supplementation on the microbiome been compared to IV iron supplementation on the microbiome?]
- Table 6 lists various iron products including costs and dosing.
- The hypersensitivity reactions to parenteral iron are mostly secondary to iron nanoparticles that trigger complement activation-related pseudo-allergy (CARPA)….It is important that parenteral iron be administered by trained personnel. Emergency medications and resuscitative equipment should be available during these infusions.
My take: This is a useful resource for a very common problem.
Related blog posts:
- CHOP QI: Anemia in IBD Pathway
- Iron Injectables | gutsandgrowth
- More Iron Infusions, Less Blood Transfusions in Kids with Inflammatory Bowel Disease; COVID-19 Transmission in Children | gutsandgrowth
- Inadequate treatment of anemia in IBD
- Is It Right? Anti-TNF Therapy Does Not Fix IBD-Related Anemia
- Be Aggressive! Treating Anemia Associated with Inflammatory Bowel Disease | gutsandgrowth
- Microcytic Anemia Review | gutsandgrowth
- IBD Update January 2015 (Part 2) | gutsandgrowth
- Help with hepcidin | gutsandgrowth
- Inadequate treatment of anemia in IBD | gutsandgrowth
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition