Methods: Retrospective chart review of 86 patients transplanted between 2003 and 2013
Key findings:
Intestinal graft survival was 71% and 65% after 5 and 10 years, respectively
Five-year graft survival was attained in 79% of patients with a history of anatomic intestinal failure (n=63) compared with 45% with functional intestinal failure (n=22) (P = 0.0055).
In their cohort, graft-versus-host and post-transplant lymphoproliferative disease were 11 times greater and 8 times greater in the functional compared with anatomic intestinal failure group. “Severe functional gastrointestinal diseases are more likely to be component of inherited multisystem disorders not fully correctable with ITx (intestinal transplantation) alone.”
Graft survival depends on avoidance of severe infectious and immunological complications including GVHD, whereas inclusion of a liver graft provides no obvious survival benefit
My take: In this cohorts, intestinal transplantation outcomes have improved for anatomic intestinal failure but not for functional intestinal failure. “Reduced success with functional intestinal failure may reflect inherently increased susceptibility to complications in this group.”
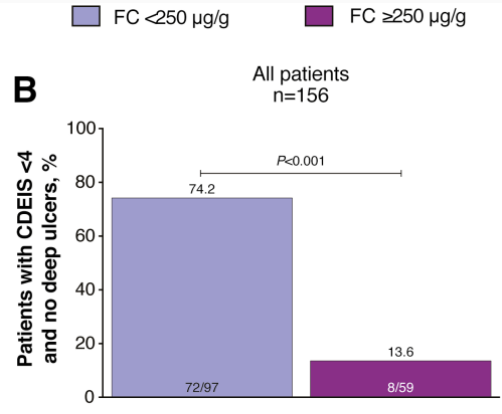
The proportion of patients who achieved the primary end point CDEIS <4 and no deep ulcers was significantly greater for those with FC <250 µg/g (74%; P < 0.001)
Fecal calprotectin <250 µg/g, CRP <5 mg/L, and CDAI <150 gave a sensitivity/specificity of 72%/63% and positive/negative predictive values of 86%/42% for CDEIS <4 and no deep ulcers 48 weeks after randomization
My take: Fecal calprotectin levels are useful for monitoring mucosal healing. Levels less than 250 are encouraging. Levels less than 100 are better.
Proportion of patients achieving mucosal healing (CDEIS <4) and no deep ulcers in (B) all patients by FC cutoff at week 48 after randomization
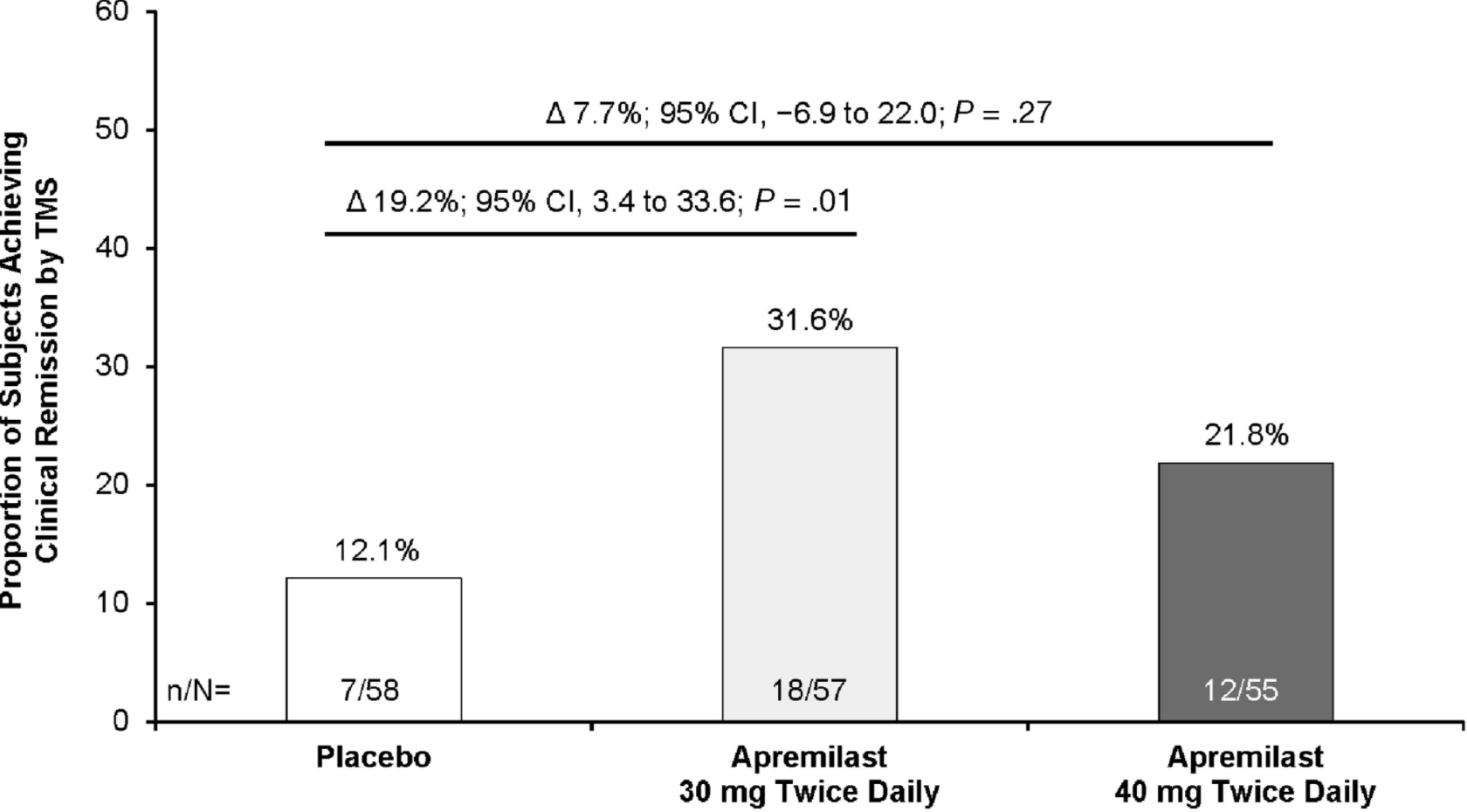
Clinical remission was achieved at week 12 by 31.6% of patients in the 30 mg apremilast group and 12.1% of patients in the placebo group (P = .01). However, only 21.8% of patients in the 40 mg apremilast group achieved clinical remission at week 12 (P = .27 compared with placebo)
At week 52, clinical remission was achieved by 40.4% of patients initially assigned to the apremilast 30 mg group and 32.7% of patients initially assigned to the apremilast 40 mg group.
Methods: Microbiota was prospectively analyzed in 49 patients with active CD at baseline, week 6, and week 30
Key Findings:
Increased proportions of Lachnospiraceae and Blautia were associated with IFX efficacy; the combined increase of these taxa at week 6 showed 83.4% and 84.2% accuracy in predicting clinical response at weeks 14 and 30, respectively, with a predictive value of 89.1% in predicting endoscopic response at week 30
IFX diminished CD-related gut microbial dysbiosis by modifying microbiota composition and function
“We found histologic evidence of UC activity (Geboes score ≥ 2B.1) in biopsies from 182 patients (65%) and endoscopic evidence of UC activity in 149 patients (53%) (substantial agreement, κ = 0.60).”
“Histologic features of UC activity were associated with increased rates of systemic corticosteroid use, colectomy, and hospitalization in the entire cohort (P < .05 for all) and associated with increased rates of systemic corticosteroid use in an analysis limited to patients in endoscopic remission (P < .001).”
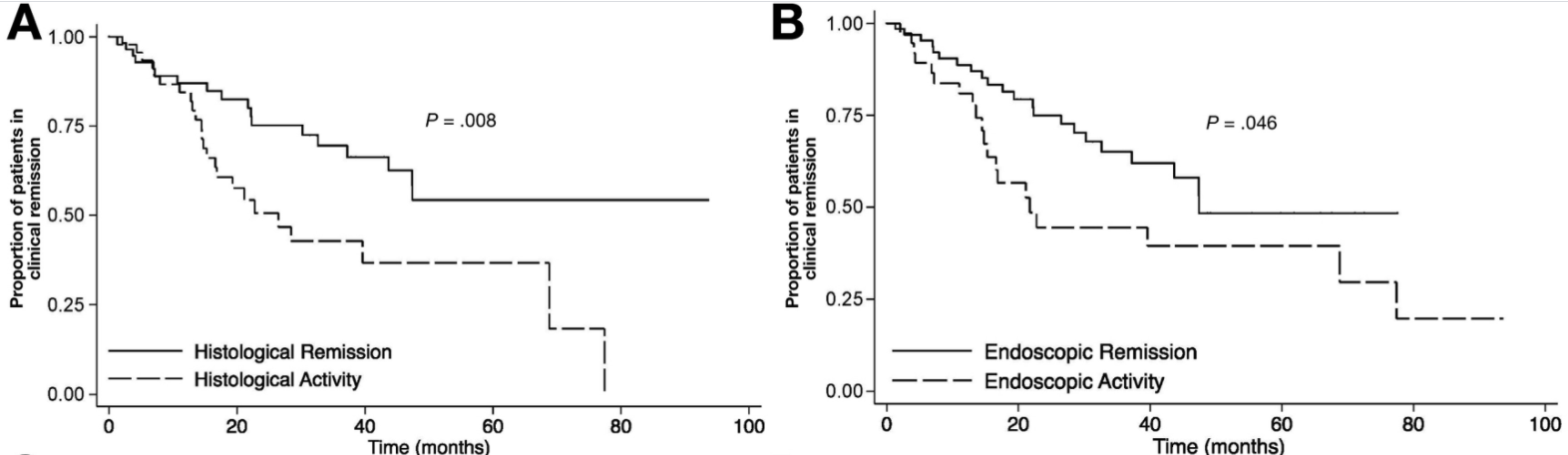
At ileo-colonoscopy, 63% of patients had endoscopic healing and 55% had histologic evidence of healing. The level of agreement between endoscopic and histologic activity was fair (62%, K = 0.2250, P = .0064)
On multivariate analysis, only histologic healing was associated with decreased risk of clinical relapse (hazard ratio [HR], 2.05; 95% CI, 1.07–3.94; P = .031), medication escalation (HR, 2.17; 95% CI, 1.2–3.96; P = .011), and corticosteroid use (HR, 2.44; 95% CI, 1.17–5.09; P = .018).
Kaplan-Meier analysis of effect of endoscopic and histologic activity on (A) clinical relapse-free survival versus histologic healing, (B) clinical relapse-free survival versus endoscopic healing
D Kevans et al. Inflamm Bowel Dis 2020; 26: 1722-1729. Histological Markers of Clinical Relapse in Endoscopically Quiescent Ulcerative Colitis Key finding: In endoscopically quiescent UC (n=76), active histological inflammation …[is] adjunctive histological marker associated with increased likelihood of disease relapse. The associated editorial (1730-32 by Asher Kornbluth) quotes Voltaire: “A wise Italian says that the best is the enemy of the good.” He notes that there is “a very real risk of abandoning an effective drug while chasing the goal of some yet to be universally defined histologic remission.” Currently organizational guidelines (ACG, AGA, ECCO, IOIBD) do NOT suggest the use of histologic normalization as an endpoint at this point.
My take: These studies show that histologic healing in ileal Crohn’s disease and in ulcerative colitis are associated with better outcomes that endoscopic appearance. However, there are a lot questions because many patients, possibly a majority, will not achieve histologic healing despite aggressive treatment. Related technical issues include how many biopsies are needed to assess histology and having a validated histologic assessment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
I did not have the opportunity to hear this #NASPGHAN20 lecture but Dr. Benchimol has shared his slides. Link to Dropbox Slides: IBD Clinical Science: Year in Review
Some of the key points on slides (links to articles below):
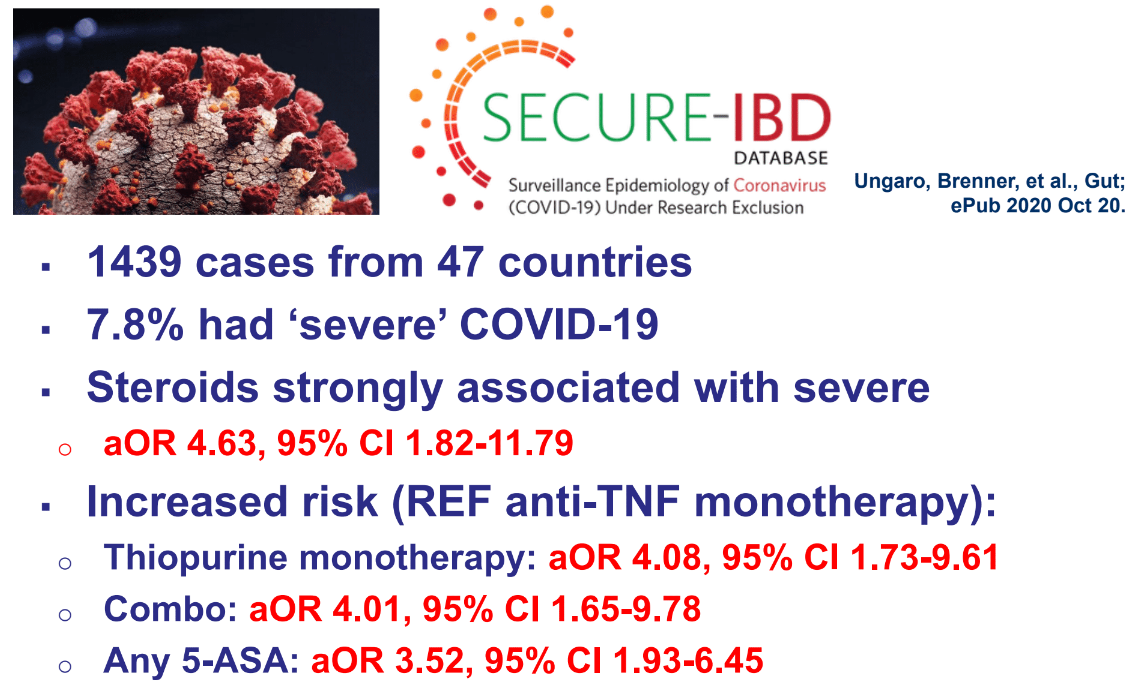
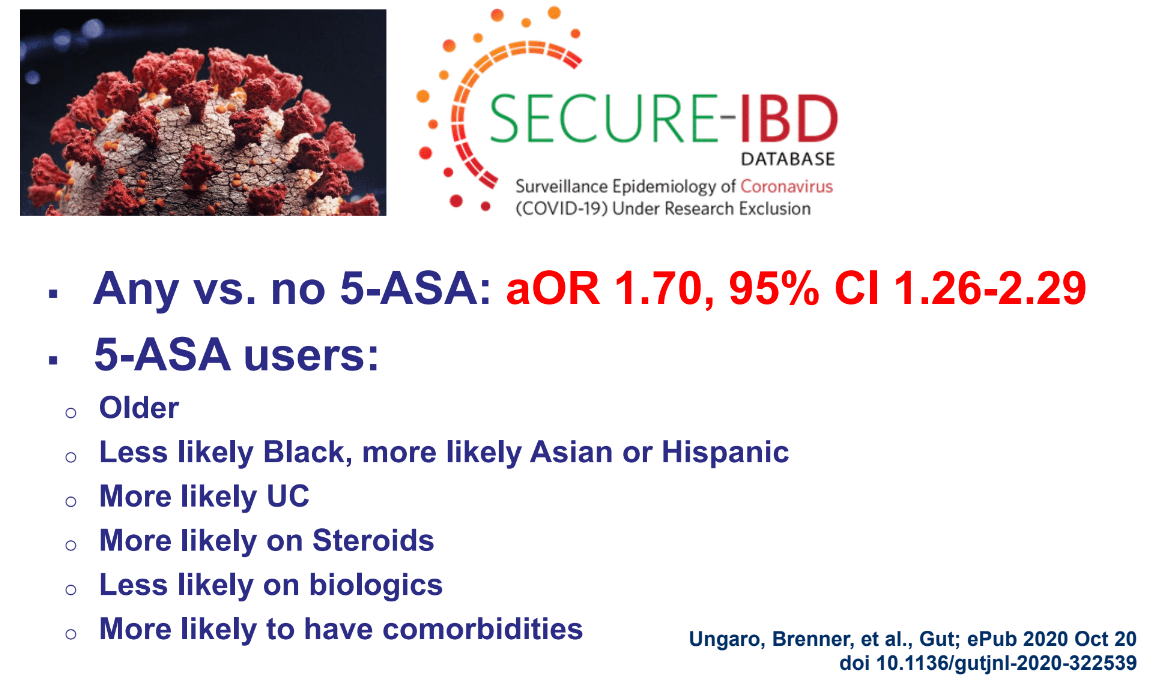
Lots of data on COVID-19 and IBD. Steroids and Thiopurines are associated with more severe disease whereas anti-TNF agents are not
Lower intestinal barrier function is associated with increased risk for development of Crohn’s disease
More greenspace associated with lower rates of development of IBD
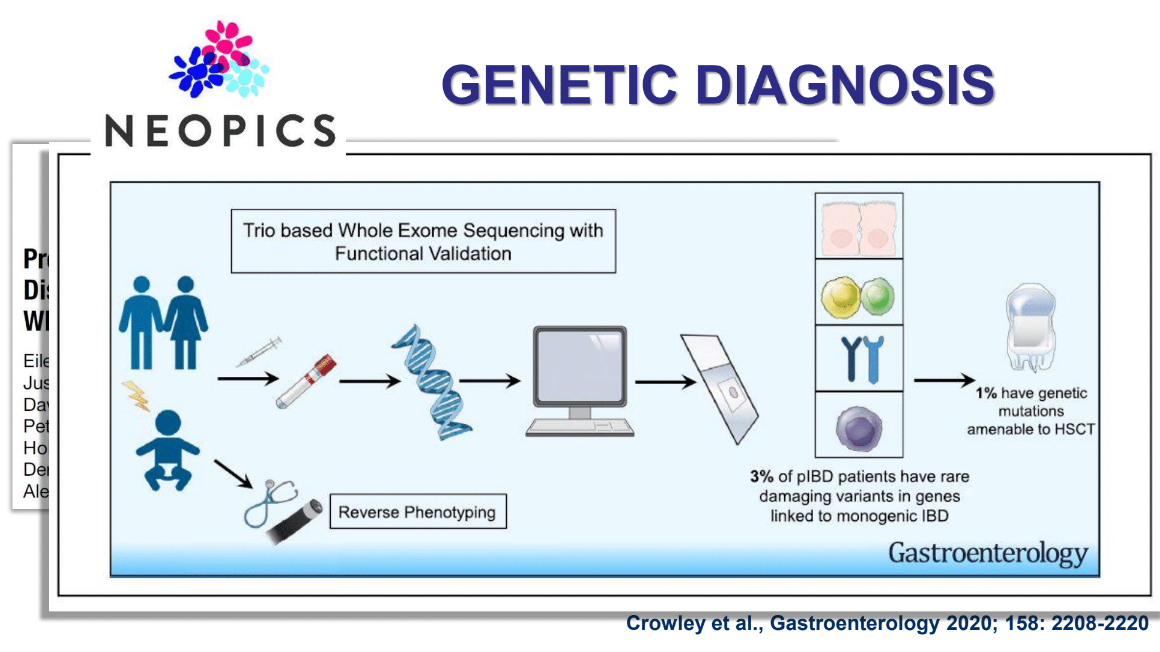
Exome sequencing has shown ~3% of pIBD with genetic mutations linked to monogenetic IBD & 1% with mutations which could benefit from HSCT. Identifying specific defects may lead to other treatments as well (eg. Leflunomide for TTC7A deficiency). Related blog posts:
Early biologic therapy associated with better long-term outcomes in adult and pediatric IBD
Reviewed data on adalimumab showing improvement in growth and relationship between good titers and clinical response (related post: IBD Update -September 2020)
Also, there will be a webinar for both patients and health care providers on November 19 with the SECURE-IBD steering committee as guests to go over the new data.
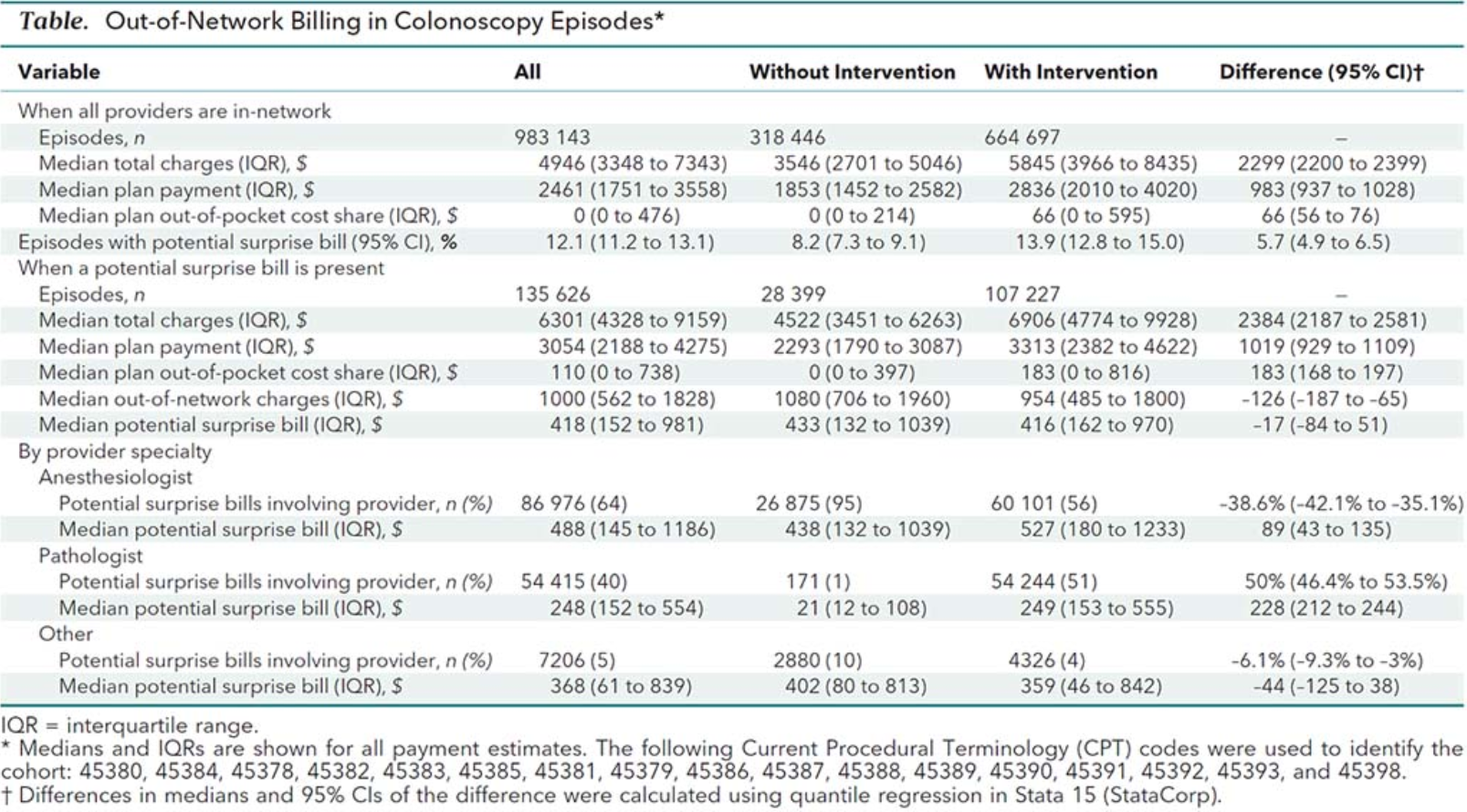
Background: “Federal law eliminates consumer cost sharing for multiple methods of colorectal cancer screening, including colonoscopy when done by an in-network provider. However, some patients having screening incur considerable out-of-pocket costs because out-of-network bills are not included in federal mandates. “Surprise billing” articles are widespread in the research literature and lay press . To date, the frequency of unexpected patient costs for screening colonoscopy have yet to be rigorously quantified.”
This study with ~983,000 procedures, which was conducted between 2012-2017, shows that it is common to get additional charges from a screening colonoscopy (which is supposed to be covered). Despite using an in-network physician, these charges can be due to “out-of-network” costs from anesthesia or pathology. This can also occur when anesthesia bills the colonoscopy as a diagnostic procedure rather than as a screening procedure.
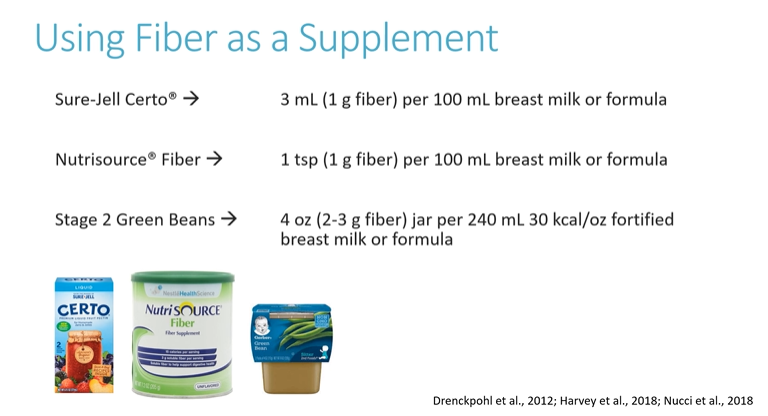
One useful resource for NASPGHAN members (NASPGHAN Nutrition Pearls) has been the short monthly nutrition pearl videos (about 10 of them so far). Here are some pointers from the most recent of these.
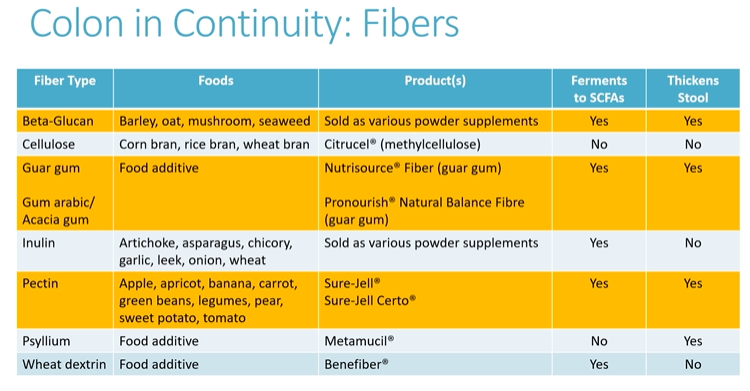
In October: Fiber for Short Bowel Syndrome –Beneficial for those with a colon in continuity:
Commercial products with limited data supporting use in short bowel syndromeAll of the fiber products are fermented in colon and may be beneficial. Highlighted products are more likely to help with stool consistency (thickening).
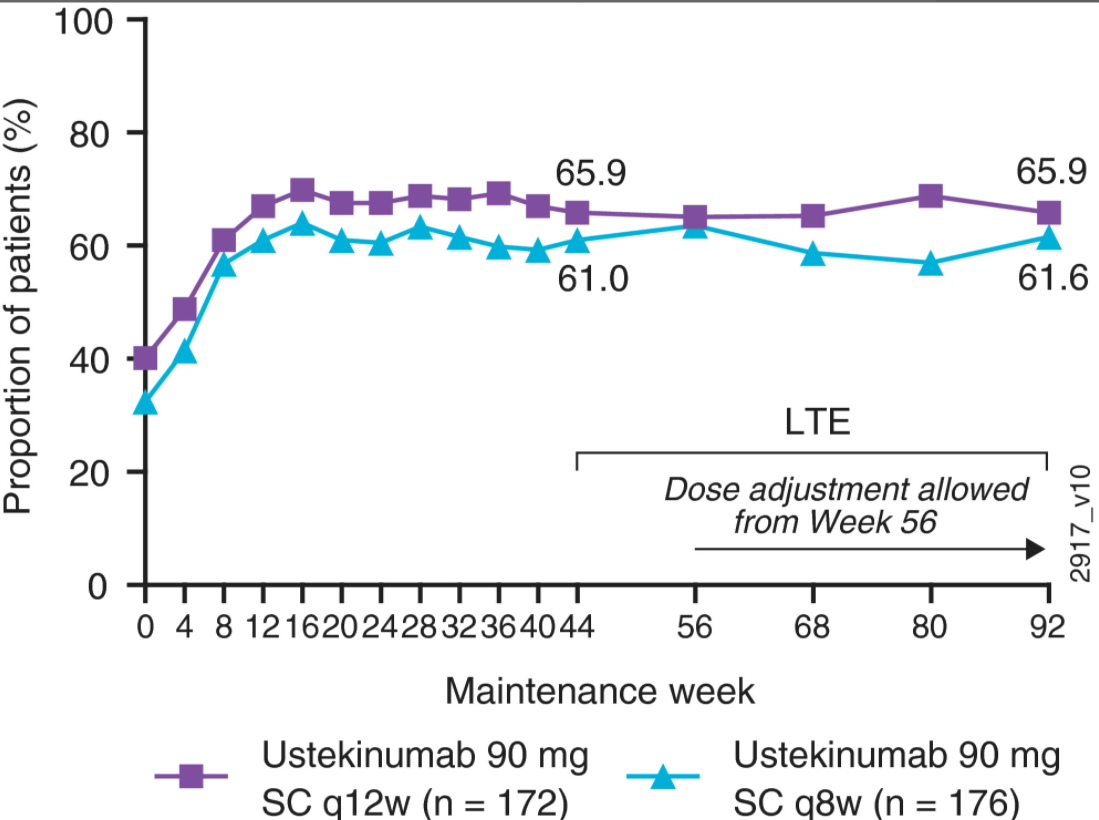
Methods: Overall, 399 (adult) “responders to intravenous ustekinumab induction and who were randomised to maintenance therapy were treated in the long‐term extension (115 received subcutaneous placebo, 141 received ustekinumab 90 mg every 12 weeks [q12w], and 143 received ustekinumab 90 mg q8w). Placebo treatment was discontinued at unblinding after week 44”
Key Findings:
Symptomatic remission rates (stool frequency = 0/1; rectal bleeding = 0) at week 92 were, 64.5% and 67.6% in the ustekinumab q12w and q8w groups, respectively ((Intent-to-treat population).
At week 44 of maintenance, measures of UC disease activity (eg Mayo scores) were generally comparable among patients randomised to ustekinumab q12w and q8w with 46.1% and 52.4% in clinical remission and 56.7% and 61.5% with endoscopic improvement respectively
Among randomised patients treated in the long‐term extension, 78.7% and 83.2% of patients receiving q12w and q8w, respectively, attained symptomatic remission at week 92; >95% of patients in symptomatic remission at week 92 were corticosteroid‐free
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
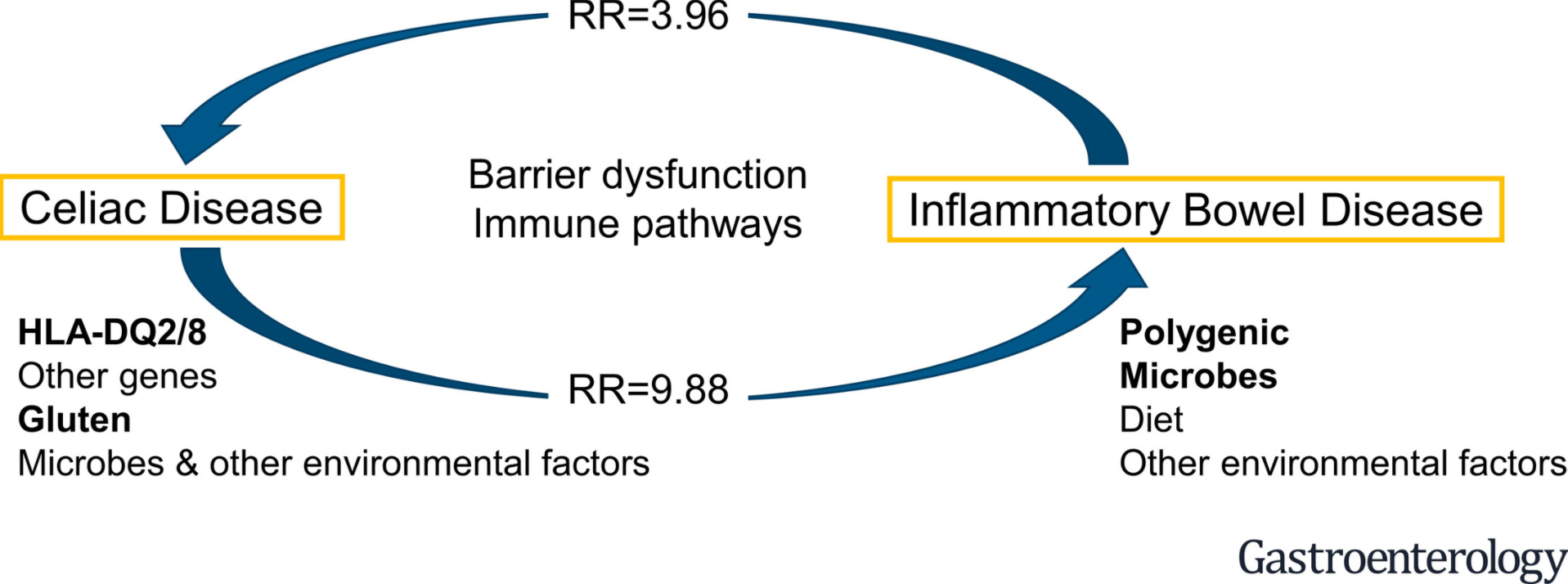
Methods: The authors identified 65 relevant studies after searching databases including MEDLINE, EMBASE, CENTRAL, Web of Science, CINAHL, DARE, and SIGLE through June 25, 2019 for studies assessing the risk of CeD in patients with IBD, and IBD in patients with CeD
Key findings:
Among patients with celiac disease, there was an increased risk of IBD vs controls (RR 9.88; 95% CI 4.03–24.21); the risk was greater for Crohn’s disease than ulcerative colitis
Among patients with inflammatory bowel disease, there was an increased risk of celiac disease vs controls (risk ratio [RR] 3.96; 95% confidence interval [CI] 2.23–7.02); however, this finding needs to be interpreted with a lot more caution.
The population-based studies that identified this risk relied on ICD codes.
Celiac diagnosis is much more difficult in patients with IBD. Overdiagnosis is possible due to increased surveillance, and misinterpretation of serology (eg. false positive serology). In addition, the pooled prevalence in this study of 0.75%, while greater than the controls of 0.3%, remains lower that the current worldwide prevalence of approximately 1%.
Only more prospective cohort studies will prove a definitive increase in risk.
My take: In patients with either IBD or celiac disease, clinicians should consider additional diagnoses in patients with ongoing symptoms.
Diagnosis of constipation is primarily based on history and physical exam –not abdominal xray (AXR). In a recent quality improvement study (G Moriel et al. J Pediatr 2020; 225: 109-116. Reducing Abdominal Radiographs to Diagnose Constipation in the Pediatric Emergency Department), ED physicians were trying to improve adherence to evidence-based guidelines for diagnosis of constipation in otherwise healthy children. In this article, the authors note evidence “has shown abdominal radiographs to be unreliable in establishing an association between clinical symptoms of constipation and fecal load on abdominal radiographs.”
As part of the study, the researchers provided two 20-minute presentations to the pediatric emergency department providers and sent emails to them and to resident housestaff. The email for ED provider’s included the provider’s baseline abdominal radiograph frequency. After study was initiated, a followup email was sent with similar information with key information on the project along with individualized data.
Key findings:
After the QI interventions, the total percentage of abdominal radiograph decreased to 18% (from 36% at baseline). This 18% decrease was significant ( P < .001) and sustained over a 12-month follow-up period.
The average length of stay was 1.07 hours longer for children who had an abdominal radiograph.
Clinically important return visits to the emergency department were uncommon during the postintervention phase (125/1830 [6.8%]), and not associated with whether or not an abdominal radiograph was performed at the initial visit.
While the study focused on healthy children, the authors noted that the overall population (6 mo-18 years) experienced a decline in AXR usage, regardless of exclusion criteria. At baseline the rate of AXR was 39.5% (1550/3926) which decreased to 20.7% (478/2311).
One interesting piece of data was showing that this intervention resulted in a sustained reduction for 12 months after the intervention observation period, which mitigates the potential influence of the Hawthorne effect.
My take: In my view, the keys to this intervention was providing individualized metrics as well as having leadership in establishing this project. The individualized metrics help physicians recognize when they are outliers and to motivate them to address this.
A recent study (SE Tarbell et al J Pediatr 2020 225: 109-108. Children with Functional Nausea—Comorbidities outside the Gastrointestinal Tract) highlights the frequent comorbidities in children with functional nausea. The authors have combined prospective and retrospective elements with specific questionnaires and review of the electronic medical records.
Key points:
High rates of comorbidities were noted: Abdominal pain 94%, Headache 83%, Orthostatic Intolerance 81%, Fatigue 75%, Disturbed sleep 71%, Anxiety 59%, and Constipation 57%. Other frequent findings included vomiting in 51%, Allergies 54%, , Joint Pain 46%, Hypermobility in 37%.
69.5% of subjects missed more than 10 days of school due to their symptoms.
There was extensive testing in this cohort (n=63), including 96 endoscopies, and 199 radiologic tests. In addition, 4 patients had cholecystectomies.
Among 64 EGDs, 28 were considered abnormal. The authors claim that 6 had specific findings: H pylori (n=2), polyps (n=2), celiac disease (n=1), and lactase deficiency (n=1).
It is likely that H pylori and celiac disease could have been identified/suspected by non-invasive testing; these two findings may make a diagnosis of functional nausea more tricky.
Lactase deficiency could be considered a normal finding.
The authors state that 32 of 59 AXRs had “moderate to severe constipation” based on stool burden
Overall, this article makes some useful points about the high rate of comorbidities with functional nausea but I disagree with some of the other discussion points.
The authors claim that “negative tests can reassure families of the absence of a more serious underlying condition.” This assertion has been disputed in other studies. In one study (A Rolfe et al. JAMA Intern Med. 2013;173(6):407-416 Full text: Reassurance After Diagnostic Testing With a Low Pretest Probability of Serious Disease), the authors conclude that ‘diagnostic tests for symptoms with a low risk of serious illness do little to reassure patients, decrease their anxiety, or resolve their symptoms, although the tests may reduce further primary care visits.’
The authors also have a permissive attitude regarding AXRs saying “a radiograph may validate a diagnosis of constipation.” Yet the preponderance of evidence indicates that AXRs are not needed or recommended for the diagnosis of constipation. The juxtaposition of this statement on page 107 of this issue with the next article on page 109 which details a quality improvement process of reducing abdominal radiographs to diagnose constipation in the ED is interesting. The ED physicians in the next article are trying to adhere to evidence-based guidelines; in this article, the authors correctly note that evidence “has shown abdominal radiographs to be unreliable in establishing an association between clinical symptoms of constipation and fecal load on abdominal radiographs.”
My take: Tarbell et al show that in patients with functional nausea, nausea is the tip of the symptom iceberg. Generally, radiographic and endoscopic diagnostic studies have very low yield and should be discouraged.