MR Jia et al. J Pediatr Gastroenterol Nutr. 2024;79:850–854. Delay in diagnosis is associated with decreased treatment effectiveness in children with rumination syndrome
In this retrospective single-center study with 247 patients, the authors evaluated whether the time from symptom onset to diagnosis over time and whether it was associated with symptom resolution.
Key findings:
- The median age at symptom onset was 11 years and median age at diagnosis was13 years
- Among the 164 children with outcome data, 47 (29%) met criteria for symptom resolution after treatment
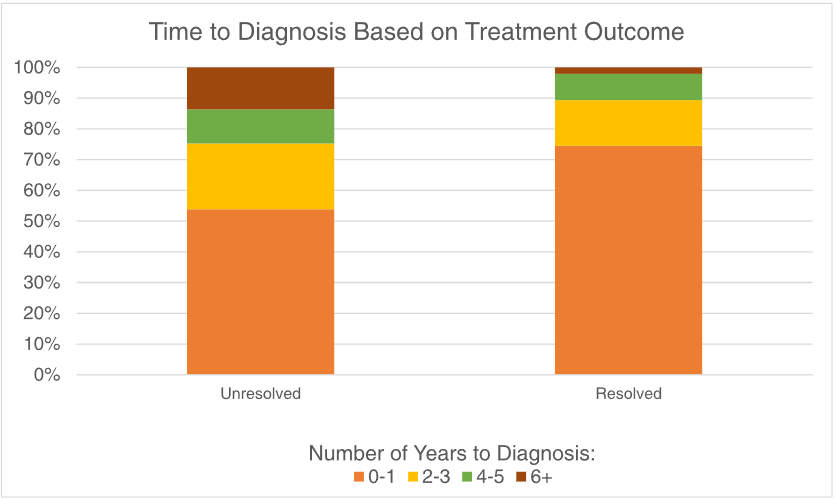
- A longer time to diagnosis was associated with a lower likelihood of symptom resolution after treatment (p = 0.01)
In the discussion, the authors note that “we suspect that one contributing factor to worse outcomes associated with diagnostic delays is the excessive testing leading to over‐medicalization of DGBIs…Our findings are the first to show that diagnostic delay contributes to poorer outcomes in children with RS, which highlights the importance of a timely diagnosis.” In fairness to the authors, other parts of the manuscript state that the delay in diagnosis is associated with worse outcomes but does not attribute causality.
Limitations:
- The patient cohort is derived from a specialized referral center (Nationwide Children’s)
- Recall bias
My take:
- While I concur that a timely diagnosis of rumination syndrome is useful, it is unproven that a delayed diagnosis contributes to a worse outcome. The outcome differences could more easily be explained by a selection bias. Patients who never recovered from rumination symptoms previously may be less likely to respond to treatment regardless of when treatment is instituted. Perhaps attributing poor outcomes to delayed diagnosis, rather than a selection bias, is due to a confirmation bias.
- Another important finding is that the more than 70% of patients did NOT have resolution of their symptoms. Realizing that many patients have some symptoms after treatment helps gastroenterologists set reasonable goals.
Related blog posts:
- Most Kids with Rumination Respond to Specialized Treatment
- Internet Survey: Lots of People Have Rumination
- Expert Advice for Diagnosis and Treatment of Rumination Syndrome
- The Half Empty Glass: Rumination Outcomes
- High-resolution Esophageal Manometry for Rumination Syndrome.
- Costs of Rumination (You don’t have to be Vinny Gambini to make the diagnosis)
- Jose Garza: What’s New in Motility (Part 2)
- Jose Garza: What’s New in Motility (Part 1)